Professional Documents
Culture Documents
Smartboy Mixed
Uploaded by
BremaDamanikOriginal Title
Copyright
Available Formats
Share this document
Did you find this document useful?
Is this content inappropriate?
Report this DocumentCopyright:
Available Formats
Smartboy Mixed
Uploaded by
BremaDamanikCopyright:
Available Formats
Articles
“Smart boys” and “sweet girls”—sex education needs in Thai
teenagers: a mixed-method study
Uraiwan Vuttanont, Trisha Greenhalgh, Mark Griffin, Petra Boynton
Summary
Lancet 2006; 368: 2068–80 Background In Thailand, rapid increases in economic prosperity have been accompanied by erosion of traditional
Department of Primary Care cultural and religious values and by negative effects on sexual health of young people. We investigated knowledge,
and Population Sciences, attitudes, norms, and values of teenagers, parents, teachers, and policymakers in relation to sex and sex education in
University College London,
Chiang Mai, Thailand, with a view to informing sex education policy.
417 Holborn Union Building,
Highgate Hill, London N19
5LW (U Vuttanont MSc, Methods We selected six secondary schools for maximum variation in socioeconomic background, religious
Prof T Greenhalgh MD, background, and location. Methods were: narrative interviews with key stakeholders, and analysis of key policy
M Griffin PhD, P Boynton PhD)
documents; questionnaire survey of 2301 teenagers; 20 focus groups of teenagers; questionnaire survey of 351 parents;
Correspondence to:
and two focus groups of parents. Qualitative and quantitative data were assessed separately with thematic and
Dr Petra Boynton
p.boynton@pcps.ucl.ac.uk statistical analysis, respectively, then combined.
Findings We noted five important influences on Thai teenagers’ sexual attitudes and behaviour: ambiguous social
roles leading to confused identity; heightened sexual awareness and curiosity; key gaps in knowledge and life skills;
limited parental input; and impulsivity and risk-taking. Male teenagers aspire to be “smart boys”, whose status
depends on stories of sexual performance and conquests. Female teenagers, traditionally constrained and protected
as “sweet girls”, are managing a new concept of dating without their parents’ support, and with few life skills to
enable them to manage their desires or negotiate in potentially coercive situations. School-based sex education is
biologically focused and inconsistently delivered.
Interpretation Results of this large exploratory study suggest five approaches that could be developed to improve sex
education: targeted training and support for teachers; peer-led sex education by teenagers; story-based scenarios to
promote applied learning; local development of educational materials; and use of trained sexual health professionals
to address learning needs of pupils, teachers, and parents.
Background manufacturing sector and international tourism. These
In November, 2005, Thailand’s Social Development and changes have been accompanied and underpinned by
Human Security Minister Watana Muangsook suggested urbanisation, westernisation, moderation of cultural and
that police officers should be stationed outside motels to religious norms, and the expansion of Thailand’s
prevent teenagers meeting for sex during a public festival. infamous sex industry. A substantial (and largely un-
The decision provoked intense public debate and an developed) rural economy remains (details of sources
editorial in Thailand’s national newspaper, The Nation: available from authors on request). Sexual health is an
increasingly important public health issue.2–4 In a recent
“Hardly a day goes by without a new, sensational study or cross-sectional survey, 43% of Thai girls aged 17 years or
opinion poll informing us about how youths are beginning
younger reported having sexual intercourse; one in five
to have sexual intercourse at an ever-younger age…
Agonising parents, teachers and social workers express of these reported this experience as coercive, and one in
outrage, lamenting Thailand’s cultural degradation and four became pregnant.5 Other studies in Thailand have
start blaming permissive Western influences for young documented increasingly early sexual debut, low rates of
people’s ‘loose sexual behaviour’. Such moral indignation contraceptive use by adolescents, a growing burden of
does nothing to reduce the widespread hypocrisy toward HIV and other sexual transmitted diseases in young
sex that has always existed in this society. These people, rising rates of teenage pregnancy and illegal
sermonising adults are inclined to paint an idyllic picture
of a puritanical Thai society, which probably has never
abortion, and the exchange of sex for money or gifts.6–9
existed, where dutiful sons and daughters grow up under These trends are similar to those in other countries in
the watchful eyes of their role model parents, keeping transition and worldwide.10–12
vows of celibacy until their marriage.”1 The coexistence in a society of traditional and
contemporary values and lifestyles produces a complex
Thailand is a country in the midst of rapid social, context for the transition from child to adult and for the
economic, and cultural change. In one generation, it has development and evaluation of sexual health education
changed from being dependent mostly on agricultural interventions for teenagers (panel 1). The teenage period
exports to having one of the most successful economies in any society is characterised by tension, transition,
in southeast Asia, reaping the benefits of an expanding risk-taking, and conflict.13 Traditionally, Thai teenagers
2068 www.thelancet.com Vol 368 December 9, 2006
Articles
have been expected to move smoothly from childhood Structural factors (ie, economic resources, policy
into adulthood while respecting their parents and their supports, social norms, government and governance,
religion; girls are required to be docile, submissive, businesses, workforce organisations, faith communities,
modest, and disinterested in sex until marriage. Male justice systems, mass media, educational systems, and
and female individuals (especially the young) should not healthcare systems) have an important effect on
be alone together. The relative permissiveness towards teenagers’ sexual choices and their response to sex
teenage culture, identity, and risk-taking seen in more education.26 Where influences such as homelessness,
developed (western) societies is not present in many abject poverty, lack of basic education, or subjugation of
transition countries, especially where religious norms women predominate, sex education is often difficult or
are strong in the older generation.13 Parents in such impossible to implement.27,28 In less extreme situations,
countries may overtly reject and even stigmatise their strong arguments exist for sex education interventions
own teenagers’ values and behaviour, leading to failure of being explicitly holistic, and being developed and
communication and loss of family support at the time evaluated within this wider structural frame.29 Countries
when it is most needed.14 undergoing rapid social and economic transition offer a
Systematic reviews of randomised trials of teenage sex shifting baseline of structural influences, raising the
education (mostly done in western countries) have shown likelihood that an intervention aimed at changing teenage
that although improvements in sexual health knowledge sexual behaviour will fail to have the anticipated effect.
and specific skills were commonly achieved, very few Research that seeks to explore the effect of several
interventions had a significant effect on sexual behaviour dynamic and conflicting cultural and social influences on
or outcome.15–17 The largely disappointing outcomes of the perceptions, standards, and actions of teenagers,
school-based sex education are probably due to the fact parents, teachers, and policymakers should have a broad
that few programmes: were firmly based on theoretical scope and methods. We aimed to inform the development
models of behaviour change; assessed what the target of sex education policy in Chiang Mai by finding out:
population of teenagers actually know, believe, and do; what teenagers know, believe, and value about sex and
acknowledged and addressed the emotional and inter- sexual health; what parents, teachers, and policymakers
personal aspects of sex as well as the biological ones; were believe and value; what areas of dissonance and tension
appropriately tailored to the child’s health literacy and exist within and between groups; how perceptions and
stage of development; took full account of cultural values, behaviours are shaped and constrained by prevailing
practical constraints, and other contextual issues; were of cultural influences; and what is currently being delivered
sufficient intensity and duration; were implemented as in terms of school-based sex education and how it is
intended; and had been optimised in a formal pilot phase perceived by all stakeholders.
before the trial began.18–25 We aimed to address how sex
education was delivered within Chiang Mai and focus Methods
particularly on the successes and problems of school-based Study design and setting
sex education in relation to this existing evidence. We did a mixed-method study based in six secondary
schools in Chiang Mai, the largest of the six provinces in
Panel 1: Thailand in transition the upper north region of Thailand with a population of
about two million, of which 11·2% are teenagers.7
Political system Concern about HIV/AIDS in this region has led to the
Feudal→Neo-capitalist introduction of a wide range of intensive interventions,
Information including school-based interventions that represent some
Restricted→Widespread of Thailand’s most progressive policies on the provision
of sex education.
Religion The study had five components: preliminary field study
Buddhist→Multi-faith or secular to gather background data and seek institutional consents;
Religiosity questionnaire survey of secondary-school-age pupils
High→Low (ages 12–21; median age 15; total 2301); focus group study
of pupils (total 185 in 20 groups of eight to 12 pupils);
Geography questionnaire survey of 351 parents; and focus group
Rural→Urbanised study of parents (total 23 in two groups).
Social values
Respects the old→Celebrates youth Procedures
Collectivist→Individual Ethics approval was obtained from University College
Trusting→Sceptical London research ethics committee, and all data were
Modesty→Self-expression obtained and stored according to requirements of the UK
Male dominated→Gender equality Data Protection Act 1998. Approval, consent, and input to
the design of the study were obtained from the governing
www.thelancet.com Vol 368 December 9, 2006 2069
Articles
body or equivalent of the individual schools during an sexual health choices are made (and in which sex
extensive consultation phase (in 2002) before the main education interventions are delivered).
fieldwork (2003–05). A summary of the main phase of For the questionnaire surveys, we modified the WHO
the project was prepared in Thai and provided to all questionnaire29 in accordance with its creators’
participants to introduce the research. Participants in the instructions: “This instrument is intended to be no more
focus groups gave verbal consent after reading the than a point of departure for investigators wishing to
information sheets or consented by completing their study the sexual and reproductive health of young people.
questionnaires. Questionnaires were distributed to It should always be adapted to local circumstances and
pupils with an emphasis that completion was voluntary priorities and, wherever possible, be used in conjunction
and that one option was to return a blank questionnaire with qualitative methods of investigation”. Other sexual
in the sealed envelope. health projects in different countries have successfully
In the preliminary phase, UV (previously a sexual used and adapted this measure.30,31
health nurse from Chiang Mai) interviewed six sex Following the guidelines produced by the questionnaire’s
education teachers and policymakers known to her. A authors, we adjusted the questionnaire to create a 73-item
snowball technique was then used, in which each self-completion pen and paper instrument that included
interviewee referred the researcher to one or two further yes or no, Likert scale, and open-ended questions. Items
colleagues for possible interview. covered knowledge of sexually transmitted infections
In selecting the six secondary schools, we aimed for (STIs), safer sex, condom use, awareness of sexual and
maximum variation in socioeconomic background of reproductive health services, communicating about sex,
pupils, prevailing cultural norms, religion, and religiosity, and reproductive health knowledge.
geographical location (urban or rural), and current We did additional analyses to assess internal validity
approach to providing sex education. Within schools, we and check that participants demonstrated consistency of
offered the questionnaire to an entire year group (which, responses amongst other similar questions on the
in Thailand, includes children of different ages, since questionnaire. For example, the following levels of
skipping or repeating a year is not uncommon) and asked agreement were identified: κ=0·314 for how to act in a
teachers to help identify individual pupils with particular relationship and sexual feelings and emotions, κ=0·631
characteristics (such as “sporty”, “studious”, “beautiful”, for using contraception and condoms, κ=0·505 for
or [general] “risk-takers”) for focus groups. We recruited contraception and abortion, κ=0·475 for condoms and
parents for the questionnaire survey through the schools, abortion, κ=0·244 for whether respondents had heard of
and a subsample of these participants volunteered for HIV and knew you could have a blood test to check for
two focus groups. the infection, and κ=0·219 for where respondents had
In the preliminary field study, we aimed to map key heard of HIV and recalled being taught about preventing
structural influences and stakeholder perspectives on infection.
sexual health issues for teenagers in Chiang Mai. Our Questionnaires were piloted in English and in Thai,
data sources are shown in panel 2. We summarised these and further refinement of questions was undertaken to
data to provide an outline of the key social, political, produce a definitive instrument that was acceptable and
economic, and technological context in which teenage comprehensible to the target respondents and which
produced reliable responses. Detailed psychometric
properties of the instrument will be published separately.
Panel 2: Data sources for preliminary field study
Most pupils chose to complete the questionnaire at
15 narrative interviews with public health specialists, sex school; a few chose another private place of their
education policymakers, local religious leaders, and preference, such as their home. Parents were recruited
schoolteachers, in which individuals were invited to give through their child’s school (eg, after a parent-teacher
personal accounts of their work in this area. 14 of these meeting) and asked to complete a ten-item pen and paper
15 participants were unknown to the investigator (UV) at the questionnaire that assessed their sexual health knowledge,
start of the study and were recruited via a snowball attitudes towards sex education, and views about teenagers
technique, which allowed identification of key professionals and sex on a five-point Likert scale. The researcher (UV)
working in this area to be identified. was present during distribution and completion of
Analysis of national and local policy documents on sexual questionnaires in schools to provide additional support or
health and sex education, including public health literature information to participants. Participants sealed question-
naires in envelopes before giving them to the researcher.
Analysis of school resources on sex and relationships Focus groups for teenagers (20 groups of eight to 12)
(curriculum summaries, videos, audiotapes, teacher were held in school and facilitated by UV. We asked them
handbooks, and sex education leaflets) in more detail about their sexual and reproductive health
A literature review on sexual health and sex education in knowledge, views about sex education and suggestions for
Thailand (and, where relevant, internationally) improvements to their current sex education. To encourage
discussion, we used a structured vignette (panel 3); we
2070 www.thelancet.com Vol 368 December 9, 2006
Articles
had developed this projection instrument in a previous
research study to promote discussion on sensitive topics.32 Panel 3: Structured vignette story used in teenage focus groups
Focus group participants are told a story about an Mali (meaning “flower”) is the same age as you. Her parents are very strict and they tell
individual of the same age and sex as themselves. The her that she must not get a boyfriend until she has finished her secondary school.
story is told in short sections, and after each section the
[Prompt: How do you think Mali would feel? What do you think she would do?]
storyteller stops and asks the group “what would this
person do or feel at this point?”. Mali meets a boy, Somchai (meaning “handsome boy”) at school and he invites her to
Parent focus groups were also held on school premises meet him in the evening.
and facilitated by UV. They were asked about their own [Prompt: How do you think Mali would feel? What do you think she would do?]
memories of sex education, their views about the sex
She goes to meet Somchai, and he suggests that they go together to the fair outside the
education their teenagers were receiving, and their
village in the evening. He indicates that he likes her very much (and they’ll have a great
suggestions for changes and improvements to current sex
time being together).
education.
[Prompt: How do you think Mali would feel? What do you think she would do? How do
Data analysis you think Somchai would feel. What do you think he would do?]
Numerical data were entered into SPSS version 12. After the fair, they go to the park, and they begin kissing. Somchai is very keen to have sex
Descriptive data were produced for sex, age, level of with Mali.
education, and religion. Responses to the questionnaire
[Prompt: How do you think Mali would feel? What do you think she would do? How do
were compared between male and female teenagers with
you think Somchai would feel? What do you think he would do?]
the χ² test.
Qualitative data were audiotaped, transcribed in Thai, Later, Mali is also keen to have sex.
and translated into English. A sample from each [Prompt: How do you think Mali would feel? What do you think she would do? Do you
qualitative data source (teen focus groups, parent focus think Mali would think about using a condom? Do you think she feel strongly about using
groups, narrative interviews) was analysed and coded a condom? Why do you think she would feel that way?]
independently by UV, PB, and TG, and discussions were
Somchai says he has no condom.
held between the three researchers to explore key themes
further and resolve discrepancies in interpretation.33 On [Prompt: What do you think Mali would do next? Why do you think she will do that way?
the basis of this discussion, we developed coding matrices What do you think Somchai would do?]
for thematic analysis based on Ritchie and Spencer’s
framework approach,34 and entered data from all where there was less discussion of the questionnaire,
transcripts into these. This allowed us to identify key response rates were slightly lower (but still 84% or
themes, explore discourses, compare these across greater). Table 2 shows demographic details of the study
respondents, and generate hypotheses where appropriate. participants. Because of the mixed methods used in this
Once preliminary data had been generated from the study, the qualitative and quantitative findings are
various empirical sources, a further phase of data reported together to present a detailed picture of each
synthesis was undertaken, in which we sought to build topic.
up a rich picture of the area of study. This phase required The most prominent theme to emerge from the
considerable discussion amongst the authors, re-analysis preliminary background phase was the coexistence of
of data sources as new hypotheses emerged, and several conflicting social and cultural influences on
progressive focussing to refine emerging themes.33 Chiang Mai society as a whole and on teenagers in
particular, especially in widespread media images of sex
Role of the funding source and sexuality. HIV/AIDS was a matter of great concern to
The sponsor of the study had no role in study design, policymakers and much effort was put into developing
data collection, data analysis, data interpretation, or programmes to raise awareness and promote safe sex
writing of the report. The corresponding author had full messages. Although the question of how sex education
access to all the data in the study and had final ought to be delivered was a popular topic in local and
responsibility for the decision to submit for publication. national media, no national consensus or strategy existed,
resulting in uncertainty and institutional inertia.
Results Sex education curricula and methods of delivery differed
Table 1 shows the characteristics of the six schools and widely between schools, but biological issues (bodily
the different samples for the questionnaire survey and changes, differences between the sexes) were prioritised
focus groups that were drawn from each school. Overall, over practicalities (eg, how to put on a condom) and there
2301 pupils and 351 parents completed the questionnaire was almost no formal teaching about emotional issues or
(with response rates ranging from 84% to 100%). In some negotiation skills. Homosexuality was sometimes
schools, pupils encouraged each other to complete the mentioned briefly. Public-health advisers supported
questionnaire in classroom settings, which explains the school-based sex education in principle, but they were
high response rates shown in table 1; in other schools rarely proactive in working with, or advising, schools.
www.thelancet.com Vol 368 December 9, 2006 2071
Articles
School type Number of Location Religious Ongoing School population Questionnaire sample Focus group sample(s)
secondary- affiliation sexual-health
school-age initatives
pupils
Socioeconomic Sex Age Number Characteristics Number Characteristics
status range (response
(years) rate)
A Government 100 Suburban Located in HIV prevention Mostly poor Mixed 6–18 53 of 55 M and F aged 1 groups M “high risk” group
expanded Buddhist project in (96%) 12–18 years
primary* temple area collaboration
with local NGO
B Government 200 Suburban None HIV prevention Mostly poor Mixed 6–16 67 of 72 M and F aged 2 groups 1 M “sporty” group,
expanded in collaboration (93%) 12–16 years 1 mixed general group
primary with GOs and
NGOs
C Government 200 Urban Located in HIV prevention Mostly poor Mixed 6–17 96 of 96 M and F aged 2 groups 1 M and 1 F general
(municipality) Buddhist and sex (100%) 13–17 years group
expanded temple area education in
primary secondary
school pilot
project
D Government 2000 Urban None HIV prevention Mixed poor Mixed 13–18 691 of 889 M and F aged 2 groups 1 M and 1 F general
(district) in collaboration and middle (78%) 13–21 years group
with GOs income
E Government 2300 Urban None HIV prevention Mixed poor Mixed 12–18 869 of 1002 M and F aged 4 groups 1 mixed “high risk”
(provincial) in collaboration and middle (87%) 12–19 years group, 1 mixed
with GOs income “studious”, 1 F and 1 M
“sporty”.
F Private 1300 Urban Supported HIV prevention Mixed poor Mixed 6–18 525 of 623 M and F aged 9 groups 1 M and 2 F general
by in collaboration and middle (84%) 12–19 years groups, 1 M “sporty”,
Protestant with GOs and income 1 mixed “beautiful” M
charity NGOs and “charming” F,
1 mixed “studious”,
1 mixed “high risk”
Total .. 6100 .. .. .. .. .. .. 2301 779 M, 1522 F 185 80 M, 95 F aged
aged 13–15 years
12–18 years
GO=governmental organisation. NGO=non-governmental organisation. M=male. F=female. Expanded primary means that the school began as a primary school and subsequently added additional year groups
to make up for limited local secondary provision. Two parent focus groups were recruited from schools B and E; 351 parents were recruited from school F.
Table 1: Characteristics of schools and field studies by school
Teachers admitted feeling uncomfortable delivering to the effect of rapid social and cultural transition on
sex education. Curricula were widely modified, and sexual knowledge, attitudes, and behaviour, which we
sometimes overtly censored, by the individuals charged grouped under five broad headings: role ambiguity and
with delivering them; such decisions were strongly confused identity; awareness, curiosity, and desire;
affected by personal values (about the immorality of sex), knowledge and skills gaps; limited parental input; and
beliefs (especially that sex education leads to sex), impulsivity, risk taking, and coercion. Each theme was
knowledge of sexual health, and past experiences affected very strongly by pupils’ sex, and to a lesser extent
(especially memories of their own sex education). by their age, school background, and personality (eg
“studious”, “sporty”, or identified by teachers as [general]
“It depends on the head teacher and teachers in each “risk takers”). We consider these themes in turn below.
school. Head teacher or teachers who are enthusiastic
and keen to give information about HIV/AIDS to their
Teenagers in this study had a dual value system and
students asked us to go to school and preparing students conflicting aspirations. On the one hand, they aspired to
for us. But in some schools, when we asked for giving modern relationships and gender roles, in which boys
education in their schools, they refused and said, ‘There and girls can date, show public affection, and experiment
is no HIV in our students—no need to go to our with sex before marriage is permitted. On the other hand,
school’.” teenagers frequently stated that they valued modesty and
Public health adviser, Chiang Mai, PH2 virginity (in girls) and respected, and sought to obey,
their parents. They were pulled towards traditional norms
The focus group and the questionnaire data revealed a through their religion, kinship ties, and sometimes
number of recurring and inter-related sub-themes related school culture; and towards western norms by mass
2072 www.thelancet.com Vol 368 December 9, 2006
Articles
shown by their comments about the fictional characters
Teenagers (n=2301)* Parents (n=351)
in the vignette scenario.
Sex
“If we do not have boyfriend or girlfriend, we seem to be
Male 918 (40·1%) 146 (41·6%)
out of fashion or we have a problem”.
Female 1373 (59·9%) 205 (58·4%)
Age (years) Female pupil, aged 15 years, focus group TF9
Teenagers “Mali would go to see Somchai. She would be stressed
12 7 (0·3%) .. and uncomfortable, she was under pressure”.
13 249 (10·9%) ..
Male pupil, aged 14 years, focus group TF15
14 449 (19·7%) ..
15 466 (20·4%) .. The teenagers’ response to the structured vignette
16 456 (20·0%) .. revealed very traditional and stereotypical constructions
17 418 (18·4%) .. of gender. Mali, as a traditional Thai girl, was expected to
≥18 231 (10·0%) .. be modest, quiet, sweet natured, and obedient. Participants
Parents acknowledged and approved of Mali’s role as a modern,
20–30 .. 8 (2·3%) fashionable teenager with a boyfriend. They described her
31–40 .. 140 (39·9%) as “in love” with Somchai and wanting him to love her,
41–50 .. 186 (53%) but many believed that Mali alone was responsible for
≥51 .. 17 (4·8%) moral aspects of the relationship, for urging restraint, and
Grade† for the provision and proper use of contraception.
Teenagers “She was the same age as us; she should have knowledge
8 (age >12) 482 (21%) .. about this. It depended on Mali [if ] she wanted to have
9 (age >13) 575 (25%) .. sex or not. Mali should tell Somchai that it was not
10 (age >14) 404 (17·6%) ..
right”.
11 (age >15) 455 (19·8%) .. Female pupil, aged 14 years, focus group TF18
12 (age >16) 381 (16·6%) ..
Parents
Boys projected their gender identities onto the male
character Somchai, expressing the high value they placed
Primary 1‡ .. 61 (17·4%)
on “being a man” and “being smart” (ie, sexually aware,
Primary 2 ... 93 (26·5%)
sexually proficient, and with several sexual partners). This
Secondary 1 .. 75 (21·4%)
male identity was expected to be enacted, displayed, and
Secondary 2 .. 44 (12·5%)
rehearsed in discussions with other boys.
Technical .. 25 (7·1%)
University .. 45 (12·8%) “Somchai would show off to his friends that he was a
Postgraduate .. 3 (0·9%) man and doing well in having sex with the girl. They
Other 5 (1·4%) would think that it was smart to have sexual experiences.
They would want to show off to their friends that they had
Religion
a number of sexual partners. Some would develop their
Buddhist 2183 (95·2%) 324 (92·3%)
scores. It was a shame for the others who had never had
Catholic 19 (0·8%) 16 (4·6%) sex.”
Protestant 73 (3·2%) 1 (0·3%) Male pupil, aged 15 years, focus group TF3
Muslim 7 (0·3%) 10 (2·8%)
None 1 (0·0%) 0 Although sexual competitiveness and performance were
Other 10 (0·4%) 0 widely viewed as a central aspect of masculinity, this
*Denominators vary slightly because of missing responses. †Because it is perception coexisted with more traditional views, in which
common for children to repeat school years, there is no upper age limit for any young men were required to respect and protect girls, and
grade. ‡Primary 1 refers to years 1–4, primary 2 to years 5–7, secondary 1 to years not “take advantage” of them or get them pregnant.
1–3, and secondary 2 to years 5–6.
Somchai’s physical coercion of Mali was seen as both
Table 2: Demographic data on research participants “natural” (because the character was viewed as an ideal
type “modern” male with particularly uncontrollable
urges) but at the same time morally unacceptable.
media influences (especially fashion) and perceived peer “If Somchai was a human, he should feel guilty. It was
pressure. Pupils from very traditional and religious wrong to having sex with Mali by forcing her. If he was a
schools expressed somewhat more traditional values than good man, he should respect the girl.”
did those from cosmopolitan and secular schools, but
Male pupil, aged 14 years, focus group TF12
role confusion was evident in all groups.
Many teenagers, especially girls, experienced these In the parents’ focus groups, parents expressed
inherent conflicts as confusion or personal stress, as concern about the effect of rapid social change on their
www.thelancet.com Vol 368 December 9, 2006 2073
Articles
children’s sexual awareness and behaviour. They masturbate. Their confusion illustrated the mixed
remarked on the earlier age of puberty, and felt that this, messages of traditional Thai culture (masturbation is a
along with media pressure, had made their children taboo topic, sinful, dirty and unhealthy, and does not
sexually aware before they were psychologically ready for occur in women and girls) and western culture
sexual relationships. They were saddened at the perceived (masturbation is normal, harmless, and useful in learning
decline in morality amongst teenagers, but confused about our bodies, especially for women and girls).
about how to protect their children from the moral and Whereas male sexual desire was expressed in terms of
physical dangers of premature sex. activity and performance, female desire was often given
“Children in this generation go out with the opposite sex
legitimacy and explained in the context of “love”, in
even when they are in school uniform. The boys go to which sex was a means of confirming feelings for, and
pick the girls up at their front doors. The girls are braver trust in, a partner. This posed a dilemma for girls; if they
than the boys, they go to the boys, have a kiss by the did not have sex, their partner might be angry or feel they
road! They will go with their friends. In the past, did not love or trust them. Many focus group participants
adolescents respected and obeyed the elders. But now, believed that Somchai would use this argument to
they are out of control”.
persuade Mali to have sex, and that Mali’s fears of losing
Father, focus group PF1 her boyfriend would lead her to have sex against her true
wishes. Some male participants believed Mali would
Most parents expressed clear disapproval of their “love Somchai more” after a good sexual performance.
children having sex before marriage. But they accepted The findings from the questionnaire (full details
that teenage boys’ sexual impulses were increasingly available from the authors; table 3) showed that teenagers’
powerful and that their sons “probably would” have knowledge of sex and sexual health issues was highly
sexual encounters at a young age. Their approach to their variable. Some questions, such as “have you heard of
daughters was less permissive. In the past, even if a AIDS?” received “yes” responses, indicating that students
teenage girl wanted a dating relationship, social norms had noticed many of the HIV campaigns being run in
and strict parenting would have limited her opportunities the region. However, responses to questions on many
to do so. Parents in our focus groups recognised that other topics (especially condom use) indicated that fewer
dating is now a fact of life, but saw it as conflicting with students believed that these issues had been taught. For
family values and with the ideal type “sweet girl” who is example, although school curriculum and HIV prevention
modest, obedient, and respectful of her parents. classes claim to cover condom use as integral to sex
Almost all the teenagers in this study showed a high education, some participants who indicated that they had
degree of awareness of, and curiosity about, sex and heard of HIV stated later in the questionnaire, and in
sexuality. An aspect of the field work that we did not focus group discussions, that they were not confident
foresee was the extent to which the teenagers in the focus about condom use. Most respondents recalled basic
groups seized the opportunity to ask questions of the biology and awareness of the term “HIV”, but many
researcher. Boys’ questions centred on what happens in recalled no coverage of homosexuality, the practicalities
the sexual act and how to perform sexually. Girls wanted of condom use, the details of what HIV actually is, and
to know how get and keep a boyfriend and how to manage sexually transmitted infections (STIs) other than HIV,
a sexual situation. Younger pupils in particular were even though all these topics were part of the school sex
preoccupied with the mechanics of sex. education curriculum. Half the pupils recalled sex
Questions typical of those asked by teenagers younger education on how to act in a relationship, even though
than 16 years were: this topic was not on the curriculum—perhaps because
“We wanted to know how boys think about girls and how
the issue had been discussed informally in class, or
girls think about boys.” because they had misunderstood the question. Girls
recalled receiving more education than did boys, and
“Is it true that the females have vaginal discharge when overall, their knowledge was greater.
they have sex needs?” The shortage of practical sessions, life-skills training,
or discussion about emotional issues in sex education
“Is it true that the male will leave the female after he has probably explained pupils’ widespread confusion about
sex with her?” the risks and options in the different stages of the vignette
scenario. For example, although most pupils’ question-
“How can I manage my desire while I am with the naire responses suggested that they knew that any sexual
opposite sex?”
encounter could result in pregnancy or STI, they never-
theless felt that Mali was unlikely to get pregnant if this
“How should girls act when having relationships?”
was her first time, Somchai was unlikely to have a
A common topic of curiosity was masturbation. Pupils sexually transmitted disease if he did not have sex very
wanted to know if it was right or wrong, could be often, and Somchai and Mali would not need a condom if
potentially harmful, and whether there was a right way to they were in a “safety period” (a vague and inconsistent
2074 www.thelancet.com Vol 368 December 9, 2006
Articles
Number (%) of pupils who recalled that this topic was covered in sex education classes p*
Girls Boys
Observed frequency Expected frequency Observed frequency Expected frequency
Have you heard of AIDS?
Yes 1327 (99·0%) 1319·8 849 (97·6%) 856·2 0·01
No 11 (0·8%) 12·7 10 (1·1%) 8·3
Don’t know 3 (0·2%) 8·5 11 (1·3%) 5·5
Can people take a blood test to find out whether they have HIV?
Yes 1313 (97·7%) 1308·7 836 (96·9%) 840·3 0·23
No 8 (0·6%) 11·6 11 (1·3%) 7·4
Don’t know 23 (1·7%) 23·7 16 (1·9%) 15·3
Can people protect themselves from
HIV?
Yes 1288 (96·1%) 1283 828 (95·2%) 833 0·55
No 17 (1·3%) 18·2 13 (1·5%) 11·8
Don’t know 35 (2·6%) 38·8 29 (3·3%) 25·2
How our bodies develop
Yes 1125 (84·1%) 1069·9 655 (73·8%) 710·1 <0·0001
No 94 (7%) 113 94 (10·6%) 75
Don’t know 119 (8·9%) 115·1 139 (15·7%) 102·9
What HIV/AIDS is
Yes 875 (65%) 766·1 396 (44·6%) 504·9 <0·0001
No 421 (31·3%) 503·9 415 (46·8%) 332·1
Don’t know 50 (3·7%) 75·9 76 (8·6%) 50·1
Contraception and birth control
Yes 848 (63%) 727·1 358 (40·4%) 478·9 <0·0001
No 432 (32·1%) 524·5 438 (49·4%) 345·5
Don’t know 65 (4·8%) 93·4 90 (10·2%) 61·6
Sexually transmitted infections other than HIV/AIDS
Yes 836 (62·5%) 732·9 379 (43·1%) 482·1 <0·0001
No 435 (32·5%) 510·9 412 (46·8%) 336·1
Don’t know 67 (5%) 94·1 89 (10·1%) 61·9
Pregnancy and having a baby
Yes 830 (61·9%) 698·8 331 (37·3%) 462·2 <0·0001
No 452 (33·7%) 564 485 (54·7%) 373
Don’t know 59 (4·4%) 78·2 71 (8·0%) 51·8
How to act in a relationship
Yes 800 (59·4%) 724·2 403 (45·3%) 478·8 <0·0001
No 394 (29·3%) 437 332 (37·3%) 289
Don’t know 152 (11·3%) 184·8 155 (17·4%) 122·2
How to use a condom
Yes 747 (55·5%) 729·3 464 (52·2%) 481·7 0·0002
No 530 (39·4%) 523·3 339 (38·1%) 345·7
Don’t know 69 (5·1%) 93·3 86 (9·7%) 61·7
Sexual feelings and emotions
Yes 668 (49·6%) 731·4 546 (61·5%) 482·6 <0·0001
No 473 (35·1%) 391·6 117 (19·9%) 258·4
Don’t know 205 (15·2%) 222·9 165 (18·6%) 147·1
Being bisexual (someone who finds both men and women sexually attractive)
Yes 612 (45·5%) 574·7 342 (38·6%) 379·3 0·001
No 589 (43·8%) 607·2 419 (47·2%) 400·8
Don’t know 143 (10·6%) 162·1 126 (14·2%) 106·9
(Continues on next page)
www.thelancet.com Vol 368 December 9, 2006 2075
Articles
(Continued from previous page)
Being lesbian (women who find other women sexually attractive)
Yes 575 (42·8%) 469 203 (22·9%) 309 <0·0001
No 670 (49·8%) 747·6 570 (64·3%) 492·4
Don’t know 100 (7·4%) 128·4 113 (12·8%) 84·6
Being gay (men who find other men sexually attractive)
Yes 529 (39·5%) 460·3 236 (26·6%) 304·7 <0·0001
No 707 (52·8%) 750·9 541 (61·0%) 497·1
Don’t know 104 (7·8%) 128·8 110 (12·4%) 85·2
Abortion
Yes 510 (37·9%) 428·3 201 (22·6%) 282·7 <0·0001
No 755 (56·1%) 815·6 599 (67·5%) 538·4
Don’t know 80 (5·9%) 101·2 88 (9·9%) 66·8
Does a person with HIV always look unhealthy?
Yes 481 (35·9%) 539·8 409 (47%) 350·2 <0·0001
No 335 (25%) 314·8 184 (21·1%) 204·2
Don’t know 525 (39·1%) 486·4 277 (31·8%) 315·6
*Comparing proportion responding yes, no, or don’t know between boys and girls. Percentages based on number with known responses.
Table 3: What Thai teenagers remember being taught in sex education classes
notion of a time in her menstrual cycle when Mali could particularly desire, lust, and frustration. Girls also
not get pregnant) or if they used the withdrawal method mentioned desire, but were equally likely to discuss love
or a vaginal pessary. Participants also did not know where or anxiety over the future of a relationship. Traditionally
Somchai and Mali might actually obtain condoms or girls are expected to be more interested in and taught
access sexual health services locally. more about feelings and emotions than are boys. We
Overall, girls seemed to recall more information from believe that these findings are more a reflection of boys’
lessons than did boys, whereas boys were more likely to interest in sex and a desire to have sex, than a wider view
respond that they did not recall or had not been taught or awareness of the diverse range of feelings and
many sexual health topics (table 3). For example, girls emotions that can accompany a sexual relationship.
were more likely than boys to recall being taught about Although a high proportion of participants of both
pregnancy and having a baby, abortion, and how our genders said they had heard of HIV/AIDS, more girls
bodies develop. This difference might have arisen than boys recalled being taught what HIV/AIDS is,
because sex education for girls is linked to informing possibly because girls’ teaching addressed this topic, or
them about menstruation, often taught in a context of because girls were more interested or concerned about
fertility, meaning that topics such as pregnancy, birth, the issue. Other research has shown that boys might
abortion, or physical development might also be taught receive less information or pay less attention to sex
in these lessons. Boys might be excluded from classes in education programmes35–36 than do girls, which might be
which menstruation is discussed, or perhaps are reflected in our findings.
discouraged from paying attention to something that is More girls than expected recalled being taught about
constructed by teachers as a girl’s issue. This discrepancy sexuality (being lesbian or gay). In a country where
could also explain why, within the qualitative data, both homosexuality is taboo, boys in particular might be
boys and girls were more likely to see negative unwilling to reveal that they recall being taught about
consequences of sex as being the fault and the being gay. Evidence from teacher interviews indicated
responsibility of a girl. that sexuality was not always discussed, because of
Interestingly, boys seemed to recall more often than teachers’ discomfort, religious beliefs, or a fear that
expected, and more often than did girls, that they had mentioning homosexuality might lead to young people
been taught about sexual feelings and emotions. This “becoming gay”.
topic did appear in the curriculum, but interviews with Evidence suggests that girls worldwide are often given
teachers suggested that it was often not taught because education on sex (particularly menstruation, pregnancy,
the teacher’s lack of skills or confidence. Although boys and birth), but in many societies (including Thailand)
recalled being taught this information in class, they because of unequal status girls are unable to put this
might have actually learned about feelings and emotions education into action, particularly in sexually coercive
through the media or peers. The qualitative accounts situations.17,18,22,35,36 Boys are assumed to be “naturally”
from boys did mention emotions relating to sex, sexual and so might not be offered sex education, or
2076 www.thelancet.com Vol 368 December 9, 2006
Articles
might be expected to be less attentive to it than are
90
girls.35–36 Additionally, boys might not be taught Boys
Girls
gender-specific issues associated with girls (such as 80
pregnancy or menstruation), which again places more
70
responsibility for learning about and controlling sexual
Proportion (%)
activity with girls. 60
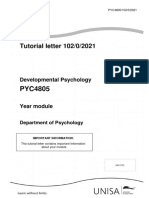
Teenagers were most likely to talk to their peers or 50
relationship partners about sex, with mothers (for girls)
40
and older friends (for boys) the next preferred source
(figure). Traditionally, Thai parents do not discuss sex 30
with their children, although mothers may prepare
20
their daughters for menstruation. Pupils were highly
unlikely to seek conversations about sex with teachers, 10
doctors, or nurses, possibility because of fear of 0
punishment and respect for authority, or lack of access
er
nd
nd
or
rse
he
he
lin
ien
ch
ct
rie
rie
Nu
ot
t
to services.
Sib
Do
Fa
Fr
rlf
rf
Te
M
de
gi
y/
Ol
Teachers and young people expressed additional
Bo
concerns about training materials and information on
sex education. Teachers were provided with school text Figure: To whom do Thai teenagers talk about sex?
books with a main focus on the biological aspects of
sex, and little focus on relationships or feelings. Some sex and the availability of sexual health and termination
teachers found these materials unhelpful and reported of pregnancy services.
that their pupils often asked for information that was “Give us real examples, what happens to people who
outside these texts. Pupils noted that they used other have sex when they are at school age, such as getting
materials where available, particularly the internet, pregnant and dropping out of school?”
films, or magazines, to access information about sex.
Female pupil, aged 13, focus group TF1
They often used these materials to fill in the gaps in
their sex education—specifically how to act in a Questionnaire data about parents’ attitudes to sex
relationship, or what to do in a romantic situation. education (table 4) showed several important in-
Parents and teachers raised a concern that these other consistencies. Although more than 90% of parents believed
source materials were often westernised and were not that sex education and reproductive health services should
always suited to traditional Thai culture or appropriate be available to teenagers, and almost as many felt that their
for the ages of the children using them. We observed children could talk about any sex related matters with them,
tensions caused by exposure to multiple messages from a similar proportion also felt that adolescents should not
existing materials, which do not always include have a boyfriend or girlfriend, and three-quarters said they
information that pupils want, and informal education would punish their child for having a sexual relationship.
by the media, which might not be accurate or More than 70% of parents did not believe that sex education
appropriate to a transitional culture. should be taught in schools, but only 10% were prepared to
Throughout the research, teachers, policymakers, be the first source of information about sex for their
healthcare staff, pupils, and parents all used the children. Almost a third felt that sex education leads to sex.
principal investigator (UV) as an informal source of sex Parents in the focus groups generally acknowledged the
information and advice. They asked her advice on what importance of sex education, and felt that it should focus
they should be teaching young people, or how to act in mainly on biological facts and the practicalities of
relationships. They wanted her to recommend contraception (possibly, parents with more liberal attitudes
resources, evaluate existing sex education programmes, might have been more willing to take part in focus groups
and supplement existing materials. Young people in than were those with traditional views). But they admitted
particular used UV as someone to add to the gaps in they were uncomfortable talking about sex with their son
their existing sex education, and this research became or daughter, and only did so superficially and occasionally.
an informal (and unplanned) means of doing this. This situation was attributed as much to lack of factual
Overall, Thai teenagers were enthusiastic about sex knowledge as to embarrassment:
education and requested more of it, especially around
managing relationships and negotiating in potentially “I did not know how to answer about periods. I only told
sexual situations. Most pupils did not plan to have sex her that if a girl had a period and had sex with a boy, she
after sex education, but they wished to be forearmed could get pregnant. ‘You should not have a sexual
with knowledge, especially practical knowledge about relationship with anybody. If you had sex you would have a
baby as I had’. This was what I told my daughter.”
what to do and how to act. Pupils also wanted
meaningful information on the consequences of having Mother, focus group PF2
www.thelancet.com Vol 368 December 9, 2006 2077
Articles
cognitive dissonance around their conflicting identities,
Number (%) of parents who agreed
with this statement (n=351)* intense sexual desire, limited knowledge and skills, and
resistance to parental domination. The very contemporary
It is necessary to talk about sexual health with children when they 320 (91%)
are adolescents scenario of Somchai and Mali finding themselves alone
Adolescents should not have a boyfriend or a girlfriend 319 (93%) together (traditionally, boys and girls would not have had
There should be reproductive health services available to 292 (83%) the opportunity to be alone together) was seen as a
adolescents powerful catalyst for sexual intimacy. Pupils used
Your children can talk and discuss all matters, including sex-related 284 (81%) metaphors depicting explosive natural phenomena and
matters, with you loss of control—describing male and female individuals,
Parents should punish their children if they have sexual relationships 231 (66%) for example, as “fire and oil” that should not be mixed.
It is embarrassing when talking about sexual health with children 108 (31%)
“Let it be, they could not wait. In that stage, they would
Sex education induces adolescents to decide to have sexual 93 (27%) not think about anything. They were in the mood. They
experiences
would lose their [desire] if they were worrying about
Sex and relationships should be taught about in school 95 (27%) using the condom.”
Teaching about contraception increases the likelihood of sexual 57 (16%)
relationships in adolescents Male pupil, aged 15 years, focus group TF7.
Parents should be the first people to teach their children about sex 34 (10%)
and relationships
These descriptions suggest that when physical
separation is traditionally the main way of controlling
There were no statistically significant differences in these responses by sex (Pearson χ2 test). *Percentages based on the sexual act, self-restraint is not expected and condom
number with known responses and accounting for missing data.
use is routinely and explicitly avoided. These are
Table 4: Attitudes of Thai parents towards teaching children about sex important messages for sex educators.
Discussion
One or two parents saw sex as a taboo subject and did In this study we aimed to inform the redesign of sex
not plan to raise it at all. But most gave strict warnings to education policy in Chiang Mai by exploring knowledge,
their children about becoming involved in what they saw attitudes, norms, and values of teenagers, parents,
as premature sexual relationships, and saw no reason teachers, and policymakers and placing these in the
for them to understand sex until a definitive adult wider social, cultural, educational, and economic context
relationship was imminent. Some parents said they of modern-day Thailand. Using a combination of
would welcome group sex-education lessons themselves, questionnaires and focus groups, and drawing heavily
covering factual knowledge and lessons on how to talk on narrative methods (especially the structured vignette
with young people about sex. technique), we have shown five important influences on
In summary, teenagers sought information that was Chiang Mai teenagers’ sexual attitudes and behaviour:
clear, non-judgemental, and non-prescriptive to help ambiguous social roles leading to confused identity,
them make complex choices in a modern world, but the heightened sexual awareness and curiosity, critical gaps
data from parents indicated a high degree of confusion in knowledge and life skills, limited parental input, and
and ignorance about sex and sexual health, a lack of (consequent on all these) an impulsive and volatile
confidence in addressing sexual issues with their approach to intimate encounters. Idealised gender roles
teenagers, and a perception that their main role in sex (the “smart boy” whose status depends on stories of
education was to instruct their child not to have sex. sexual performance and conquests, and the sweet girl
The themes discussed above seemed to contribute to a who despite her western dress and willingness to have
pattern of behaviour characterised by mutual mistrust relationships, retains traditional submissiveness and
between adolescents and parents, secrecy and lacks negotiating skills) and increasing opportunities for
disobedience, impulsivity, risk taking, and (sometimes) privacy create the preconditions for coercive, unprotected
sexual coercion of girls by boys. Teenagers viewed strict sex.
and traditional Thai parenting as having negative Chiang Mai teenagers have reasonable knowledge of
consequences: biological issues from sex education but are confused
“Mali would escape from home. She would lie to [her
and uncertain about how to obtain or use contraception,
parents] that she would go to her friends’ home for avoid pregnancy and transmission of STIs, negotiate
reading”. personal and intimate relationships, and find sources of
support and advice. Many parents lack the knowledge,
Male pupil, aged 14 years, focus group TF10
confidence, and contemporary values to be able to give
Focus group participants explained the unfolding meaningful support to their children. The largely didactic
vignette scenario in terms of an impulsive and irresistible and biological sex education curriculum fails to meet
passion on the part of both the male and female pupils’ expressed need for more applied knowledge, life
characters, whose ability to think and plan rationally skills, and confidence training. Boys seem likely to
about their sexual relationship was diminished by misunderstand and forget key issues, while being overly
2078 www.thelancet.com Vol 368 December 9, 2006
Articles
concerned about sexual performance and conquests. Thailand do not have the relevant life skills and could be
Girls seem to receive more sex education than do boys, sources of misinformation (for example about a
but this difference may support existing stereotypes, in non-existent “safety period”) and entrenched values
which girls are assigned responsibility for managing sex (such as the smart boy ideal). With these caveats in mind,
(although many do not actually have the power to do so). the input of teenagers themselves to sex education
These findings are similar to those from other interventions should be explored further.
countries.35,36 Third, the popularity and success of the vignette
Existing sex education programmes in Chiang Mai are scenario in prompting discussion and critical reflection
popular with teenagers. However, our findings suggest a about sexual health in this study shows the potential
need for a substantially broadened sex education value of story-based methods in sex education40 Evidence
curriculum that addresses and challenges gender from other countries suggests that thinking through the
stereotypes, develops practical and life skills, explicitly range of consequences (both positive and negative) of a
considers situations in which sexual coercion may arise, potential sexual encounter can lead to a reduction in
and is delivered consistently across different schools and risk-taking behaviours.41 Since the story is inherently
by different providers. both chronological (it unfolds over time) and malleable
As an exploratory study that was not designed to test (there are several possible endings to an unfinished
the effect of a specific intervention, and that only story), it is an ideal vehicle for the delivery of
investigated what participants say they do rather than consequence-based education. Different media, such as
what they actually do, the research reported here can film, magazine articles, and popular music might be
only generate hypotheses about the key influences on used creatively for active learning.
sexual risk taking in Chiang Mai teenagers. Its main Fourth, we found that because of the coexistence of
strengths were the inclusion of a native Thai health-care traditional and contemporary cultures and value systems,
worker, trained in sexual health research, as the principal western sex-education materials cannot be transferred
investigator; extensive preliminary fieldwork to build comprehensively to the Thai context. Materials that are
relationships with participating schools; a large and locally developed and that draw critically and eclectically
heterogeneous sampling frame; mixed quantitative and on western resources and images are probably essential
qualitative methods; and an analytic approach that to the success of a complex intervention.
contextualised the findings in a wider frame of rapid Fifth, in our study, the researcher (UV) was used
social transition. Its main limitations were that several extensively by pupils, parents and teachers as a source of
of the schools (and most parents interviewed) were knowledge and advice. This finding suggests a potential
relatively affluent, and the study was (for practical intervention in the form of a trained professional who is
reasons) limited to a single region within Thailand, so confident and comfortable with delivering sex-education
the generalisability of findings to Thai teenagers in support to a range of audiences. Such an individual
general has not been established. With this important could work flexibly with pupils, parents, and teachers to
limitation in mind, further studies are now needed to address knowledge gaps and develop skills and
develop appropriate interventions aimed at addressing confidence in areas identified by them. He or she could
the critical factors suggested by this study, and to test act as an acceptable and effective mechanism, for
these systematically. example, for delivering a school-based sex-education
First, our findings indicated that strong head-teacher curriculum to parents.
support greatly enhanced the delivery and uptake of In conclusion, our findings affirm the huge amount of
school sex education, that Thai teachers might not have work already done in Chiang Mai to develop and deliver
adequate knowledge or confidence to deliver sexual appropriate HIV awareness and school-based sex-
health advice, that talking about sex might conflict with education programmes in the context of rapid cultural
teachers’ personal or professional values or with transition and overwhelming media pressure on
classroom culture, and that teachers might censor or teenagers. We have also identified several possibilities
adapt evidence-based intervention packages in the light that could help sex-education teams and researchers to
of personal beliefs or past experience.37 Targeted training, refine existing interventions and develop support for sex
support, and mentoring of teachers is probably a educators. The study design is potentially transferable to
prerequisite for the effective and consistent delivery of a other contexts in developing and transition countries.
broader sex education curriculum. Contributors
Second, we found that peers were the preferred source U Vuttanont conceptualised the study and undertook the field research
of information by all age groups and by both sexes, and in Thailand, with methodological support from the other authors.
P Boynton, U Vuttanont, and T Greenhalgh analysed the qualitative data.
that both parents and teachers have limitations as sex PB, U Vuttanont, and M Griffin analysed the quantitative data.
educators. Peer-led sex education has some theoretical P Boynton, T Greenhalgh, and U Vuttanont synthesised the data from
advantages (especially acceptability and influence) but different sources and wrote the paper.
has not been consistently shown to produce better Conflict of interest statement
outcomes.38,39 Our findings suggests that teenagers in We declare that we have no conflict of interest.
www.thelancet.com Vol 368 December 9, 2006 2079
Articles
Acknowledgments 20 Kirby D. Effective approaches to reducing adolescent unprotected sex,
We thank the pupils, parents, educators, and health-care staff who pregnancy, and childbearing. J Sex Res 2002; 39: 51–57.
participated in this research; Henry Potts (CHIME, University College 21 Cowan FM. Adolescent reproductive health interventions.
London) for advice on statistical analysis; and the reviewers of this paper Sex Transm Infect 2002; 78: 315–18.
for their detailed feedback. 22 Oakley A, Fullerton D, Holland J, et al. Sexual health education
interventions for young people: a methodological review. BMJ 1995;
References 310: 158–62.
1 The Nation. Editorial. The Nation (Bangkok), Nov 14, 2005. 23 Jejeebhoy SJ. Adolescent sexual and reproductive behavior: a review
2 Internation Planned Parenthood Federation. IPPF Country Profiles: of the evidence from India. Soc Sci Med 1998; 46: 1275–90.
Thailand. 2001: http://ippfnet.ippf.org/pub/IPPF_Country (accessed 24 Wight D, Abraham C. From psycho-social theory to sustainable
Nov 22, 2006). classroom practice: developing a research-based teacher-delivered sex
3 United Nations Educational, Scientific and Cultural Organization. education programme. Health Educ Res 2000; 15: 25–38.
Thailand—demographic characteristics of adolescents. 2001: http:// 25 Buston K, Wight D, Hart G, Scott S. Implementation of a
www.unescobkk.org/ips/arh-web/case studies/thailand/1/.htm teacher-delivered sex education programme: obstacles and facilitating
(accessed Nov 22, 2006). factors. Health Educ Res 2002; 17: 59–72.
4 United Nations Educational, Scientific and Cultural Organization. 26 Buckingham D, Bragg S. Young people, sex and the media. The facts
Thailand—programme responses to ARSH problems. 2001: http:// of life? Basingstoke: Palgrave Macmillan, 2004.
www.unescobkk.org/ips/arh-web/case_studies/thailand/3.htm
(accessed Nov 22, 2006). 27 Sumartojo E. Structural factors in HIV prevention: concepts,
examples, and implications for research. AIDS 2000; 14 (suppl 1):
5 Allen DR, Carely JW, Manopaiboon C, et al. Sexual health risks S3–10.
among young thai women: implications for HIV/STD prevention and
contraception. AIDS Behav 2003; 7: 9–21. 28 UNAIDS Inter Agency Task Team (IATT) on Education. HIV
prevention and education—a strategic approach. Geneva: IIEP
6 Isarabhakdi P. Factors associated with sexual behavior and attitudes Publications-UNESCO; 2002.
of never-married rural Thai youth. Warasan Prachakon Lae Sangkhom
1999; 8: 21–44. 29 Cleland J, Ingham R, Stone N. Asking young people about sexual and
reproductive behaviours: illustrative core instrument. 2000: http://
7 Agence France Presse. Thailand: rate of HIV infection grows among www.who.int/reproductive-health/adolescent/docs/qestionnaire_
Thai teenagers. CDC News Update. Paris: Agence France Presse, intro.pdf (accessed Nov 27, 2006).
2003.
30 Puri M, Cleland J. Extent of sexual coercion among young female
8 Warakamin S, Takrudtong M. Reproductive health in Thailand: an migrant carpet and garment factory workers in Nepal. 2006:
overview. 1998. Southampton: Southampton Statistical Sciences Research Institute,
9 Chemnasiri T, Plipat T. Related behaviours to HIV infection of 2006.
students in Moa5, round 10. Bangkok: International Conference of 31 Mohammed EM, Mohammed K, Farahani FKA, et al. Reproductive
AIDS, 2004. knowledge, attitudes and behaviour among adolescent males in
10 Nicoll A, Gill ON. The global impact of HIV infection and disease. Tehran, Iran. Int Family Plan Perspect 2006; 32: 35–44.
Commun Dis Public Health 1999; 2: 85–95. 32 Greenhalgh T, Helman C, Chowdhury AM. Health beliefs and folk
11 Burtney E, Duffy M. Young people and sexual health: individual social models of diabetes in British Bangladeshis: a qualitative study. BMJ
and policy contexts. Basingstoke: Palgrave Macmillan, 2004. 1998; 316: 978–83.
12 World Health Organization. Sexually transmitted infections: issues in 33 Parker I, Burman E. Discourse analytic research: repertoires and
adolescent health and development. WHO Discussion Papers on readings of texts in action. Hove and New York: Taylor and Francis,
Adolescence. Geneva: WHO, 2004. 1993.
13 Dasen PR. Rapid social change and the turmoil of adolescence: a 34 Ritchie A, Spencer L. Qualitative data analysis for applied policy
cross-cultural perspective. Int J Group Tensions 2002; 29: 17–49. research. In: Bryman A, Burgess RG, eds. Analyzing qualitative data.
14 Campbell C, Foulis CA, Maimane S, Sibiya Z. “I have an evil child at London: Routledge, 2001.
my house”: stigma and HIV/AIDS management in a South African 35 Hilton G. Sex education—the issues when working with boys.
community. Am J Public Health 2005; 95: 808–15. Sex Educ 2001; 1: 35–41.
15 DiCenso A, Guyatt G, Willan A, Griffith L. Interventions to reduce 36 Measor L, Tiffin C, Fry K. Gender and sex education: a study of
unintended pregnancies among adolescents: systematic review of adolescent responses. Gend Educ 1996; 8: 275–88.
randomised controlled trials. BMJ 2002; 324: 1426. 37 Oshi DC, Nakalema S, Oshi LL. Cultural and social aspects of
16 Johnson BT, Carey MP, Marsh KL, Levin KD, Scott-Sheldon LA. HIV/AIDS sex education in secondary schools in Nigeria. J Biosoc Sci
Interventions to reduce sexual risk for the human immunodeficiency 2005; 37: 175–83.
virus in adolescents, 1985–2000: a research synthesis. 38 Kirby D. Effective approaches to reducing adolescent unprotected sex,
Arch Pediatr Adolesc Med 2003; 157: 381–88. pregnancy, and childbearing. J Sex Res 2002; 39: 51–57.
17 Kirby D. Effective approaches to reducing adolescent unprotected sex, 39 Campbell C, MacPhail C. Peer education, gender and the
pregnancy, and childbearing. J Sex Res 2002; 39: 51–57. development of critical consciousness: participatory HIV prevention
18 Pedlow CT, Carey MP. Developmentally appropriate sexual risk by South African youth. Soc Sci Med 2002; 55: 331–45.
reduction interventions for adolescents: rationale, review of 40 Greenhalgh T, Collard A, Begum N. Sharing stories: complex
interventions, and recommendations for research and practice. intervention for diabetes education in minority ethnic groups who do
Ann Behav Med 2004; 27: 172–84. not speak English. BMJ 2005; 330: 628.
19 Robin L, Dittus P, Whitaker D, et al. Behavioral interventions to 41 Ross MW, Ekong E, Ogungbade GO. Year cohort of Nigerian military
reduce incidence of HIV, STD, and pregnancy among adolescents: a personnel. Cape Town: AIDS Impact Conference, 2005.
decade in review. J Adolesc Health 2004; 34: 3–26.
2080 www.thelancet.com Vol 368 December 9, 2006
You might also like
- 450 968 1 SMDocument8 pages450 968 1 SMBremaDamanikNo ratings yet
- Fox 1968Document7 pagesFox 1968BremaDamanikNo ratings yet
- 2010 2011 2014 2015 Mental Health Mental Illness Activities Health Canada Public Health Agency Canada EngDocument71 pages2010 2011 2014 2015 Mental Health Mental Illness Activities Health Canada Public Health Agency Canada EngBremaDamanikNo ratings yet
- 1 PBDocument8 pages1 PBBremaDamanikNo ratings yet
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5806)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (897)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (401)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (842)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (589)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (345)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1091)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- Background: Adolescents' Use of Social Media, Which Has Increased Considerably in TheDocument3 pagesBackground: Adolescents' Use of Social Media, Which Has Increased Considerably in TheShamaica SurigaoNo ratings yet
- MAPEH 1stQUARTERLASDocument20 pagesMAPEH 1stQUARTERLASSirawai National High SchoolNo ratings yet
- 2021 Nghệ an Phân TíchDocument12 pages2021 Nghệ an Phân TíchTrang Nguyễn100% (1)
- Flashman & Gambetta (2014) - Thick As Thieves: Homophily and Trust Among DeviantsDocument43 pagesFlashman & Gambetta (2014) - Thick As Thieves: Homophily and Trust Among DeviantsRB.ARGNo ratings yet
- Human Development: Meaning, Concepts and ApproachesDocument13 pagesHuman Development: Meaning, Concepts and ApproachesBuaga Marc Marius MNo ratings yet
- Mental Health Counselor in Greensboro NC Resume Anita JonesDocument2 pagesMental Health Counselor in Greensboro NC Resume Anita JonesAnitaJonesNo ratings yet
- Health: Quarter 1-Module 6Document25 pagesHealth: Quarter 1-Module 6Niko Igie Albino Pujeda0% (1)
- Ootd Preferences Simple Contra Trendy and The Level of Self-Confidence of Grade 12 Students in MiinhsDocument43 pagesOotd Preferences Simple Contra Trendy and The Level of Self-Confidence of Grade 12 Students in MiinhsChristian RamosNo ratings yet
- Long Term Development in Sport and Physical Activity 3.0Document48 pagesLong Term Development in Sport and Physical Activity 3.0Anderson TeixeiraNo ratings yet
- Death and DyingDocument52 pagesDeath and DyingKaren HernandezNo ratings yet
- MS Student Planner SY1617Document186 pagesMS Student Planner SY1617International School ManilaNo ratings yet
- Raising Siblings Without RivalryDocument32 pagesRaising Siblings Without RivalryMoveshade74100% (1)
- Chapter 3Document12 pagesChapter 3Richele RoquillasNo ratings yet
- RFST ProjectDocument74 pagesRFST ProjectSakib Hasan Dhruba100% (3)
- Pyc4805 Tutorial GuideDocument19 pagesPyc4805 Tutorial GuideMelissaNo ratings yet
- Post Test FacilitatingDocument9 pagesPost Test FacilitatingGibriel SllerNo ratings yet
- DO s2018 006 PDFDocument7 pagesDO s2018 006 PDFRaquelito Belmonte CenalNo ratings yet
- Defining Child Sexual AbuseDocument14 pagesDefining Child Sexual AbuseAndreas Springfield GleasonNo ratings yet
- PerDev Q2 Mod1 Dynamics-of-Attraction-and-Love v5Document26 pagesPerDev Q2 Mod1 Dynamics-of-Attraction-and-Love v5Lyster AvilesNo ratings yet
- Jean Jacques RousseauDocument6 pagesJean Jacques RousseauRokeyaNo ratings yet
- Argument Paper FinalDocument5 pagesArgument Paper Finalapi-512832188No ratings yet
- Awareness in Teenage PregnancyDocument7 pagesAwareness in Teenage PregnancyEdwardJohnG.CalubIINo ratings yet
- IELTS Academic Writing Task 1Document2 pagesIELTS Academic Writing Task 1Rania ChokorNo ratings yet
- 18 BibliographyDocument29 pages18 BibliographyAnju Dwivedi ShuklaNo ratings yet
- Philippine Supreme Court Jurisprudence: Home Law Firm Law Library Laws JurisprudenceDocument43 pagesPhilippine Supreme Court Jurisprudence: Home Law Firm Law Library Laws JurisprudenceAudrin Agapito deasisNo ratings yet
- The Model of Threats To Information and Psychological Security Taking Into Account The Hidden Information Destructive Impact On The Subconscious of AdolescentsDocument4 pagesThe Model of Threats To Information and Psychological Security Taking Into Account The Hidden Information Destructive Impact On The Subconscious of AdolescentsMinh DangNo ratings yet
- The Effects of Smartphone Addiction To The Mental Health Among Nursing StudentsDocument59 pagesThe Effects of Smartphone Addiction To The Mental Health Among Nursing StudentsJustine CagatanNo ratings yet
- Find Your EdgeDocument56 pagesFind Your EdgeSpeed Skating Canada - Patinage de vitesse CanadaNo ratings yet
- SJPO2015 ResultsDocument9 pagesSJPO2015 ResultsLin MinhtooNo ratings yet
- Chirp The Family Life CycleDocument3 pagesChirp The Family Life CycleJoshua MwanguNo ratings yet