You might also like
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (589)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (401)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (842)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (897)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5806)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (345)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1091)
- 1 Haunted Perron ManorDocument185 pages1 Haunted Perron Manormiguel ghanemNo ratings yet
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Megger Test Form-NewDocument2 pagesMegger Test Form-NewShahadad PNNo ratings yet
- Practical Foundation Design With Staad Foundation AdvancedDocument384 pagesPractical Foundation Design With Staad Foundation AdvancedPratyush Kumar100% (3)
- Hetron Fabrication Process PDFDocument57 pagesHetron Fabrication Process PDFDyah AyuNo ratings yet
- Toy Racing Car Plans PDFDocument10 pagesToy Racing Car Plans PDFsalomão sibaldeNo ratings yet
- Warehouse Order ProcessingDocument67 pagesWarehouse Order ProcessingYogitha BalasubramanianNo ratings yet
- Assessment of The Environmental Impact of Land ReclamationDocument37 pagesAssessment of The Environmental Impact of Land ReclamationtoufeeqahmedsathioNo ratings yet
- PARI - Storage Automation - ASRSDocument4 pagesPARI - Storage Automation - ASRSUmeshNo ratings yet
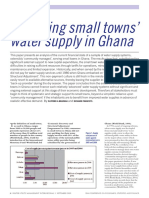
- Small Towns Water Upply in GhanaDocument4 pagesSmall Towns Water Upply in GhanaUMAR IDDRISUNo ratings yet
- XRays LectureSlides RW VL2Document18 pagesXRays LectureSlides RW VL2UMAR IDDRISUNo ratings yet
- Pnas 1405672111Document6 pagesPnas 1405672111UMAR IDDRISUNo ratings yet
- Simulations of SNR Efficiency of DTI Using Parallel Imaging and rFOV Acquisition at 3 T and 7 TDocument1 pageSimulations of SNR Efficiency of DTI Using Parallel Imaging and rFOV Acquisition at 3 T and 7 TUMAR IDDRISUNo ratings yet
- WbnotDocument2 pagesWbnotJeshiNo ratings yet
- Joint Department Admin Order No. 2Document8 pagesJoint Department Admin Order No. 2business permits and licenses div.No ratings yet
- Customer Satisfaction, Market Share and ProfitabilityDocument15 pagesCustomer Satisfaction, Market Share and Profitabilityxaxif826550% (2)
- COMM 400 Assignment #1 My StoryDocument4 pagesCOMM 400 Assignment #1 My StoryMegan 'Hall' AdamsNo ratings yet
- Whole Digital Communication PPT-libreDocument319 pagesWhole Digital Communication PPT-librePiyush GuptaNo ratings yet
- HFSS Datasheet WebDocument2 pagesHFSS Datasheet Webbecool_bcn75No ratings yet
- Project Plan For Implementation of ISO 20000 20000academy ENDocument7 pagesProject Plan For Implementation of ISO 20000 20000academy ENit20645984 Imashi H.M.G.G.M.No ratings yet
- Aprea 2002Document14 pagesAprea 2002VIKNESWARAN S KNo ratings yet
- Ignou Thesis FormatDocument8 pagesIgnou Thesis Formatdnr8hw9w100% (2)
- BRANIGAN - Eduard - A Point of View in The CinemaDocument6 pagesBRANIGAN - Eduard - A Point of View in The CinemaSonia RochaNo ratings yet
- Cornell-Engineers-Sample-Drawings PAGE1Document1 pageCornell-Engineers-Sample-Drawings PAGE1mohanumaNo ratings yet
- Sherwood Engineering VHF/UHF Test ResultsDocument7 pagesSherwood Engineering VHF/UHF Test ResultsIU8JTANo ratings yet
- M-VAT 012018 BIR Email Notification (EFiling of Tax Return)Document2 pagesM-VAT 012018 BIR Email Notification (EFiling of Tax Return)Don SumiogNo ratings yet
- A Level Chemistry Paper 1 Set 1Document20 pagesA Level Chemistry Paper 1 Set 1RUBANGAKENE DENISNo ratings yet
- Archmodels Vol.06Document5 pagesArchmodels Vol.06JJ PeterNo ratings yet
- Politeness in Friends TV Series Does It Represent American Value?Document7 pagesPoliteness in Friends TV Series Does It Represent American Value?Dieu LinhNo ratings yet
- 6599892Document127 pages6599892Dino Martin Mercado QuispeNo ratings yet
- Tarea I de EnglishDocument3 pagesTarea I de Englishjean carlos vasquezNo ratings yet
- Jacques Lacan - Seminar On The Purloined LetterDocument11 pagesJacques Lacan - Seminar On The Purloined LetterJose Jr OrquiaNo ratings yet
- Wa0001Document8 pagesWa0001varshasharma05No ratings yet
- Finals PPT Notes - Economic DevelopmentDocument6 pagesFinals PPT Notes - Economic DevelopmentGRACELINE JOY TOMENo ratings yet
- RA 11038 - ENIPAS Protected AreasDocument4 pagesRA 11038 - ENIPAS Protected AreasMarie Mariñas-delos ReyesNo ratings yet