You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5796)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1091)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (589)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (345)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (400)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Routes Into Nursing: (Apprenticeship Options Also Available)Document1 pageRoutes Into Nursing: (Apprenticeship Options Also Available)Zeeshan ShafqatNo ratings yet
- Impaired Oral Mucous MembraneDocument2 pagesImpaired Oral Mucous Membranemai_serpic100% (1)
- Health Card TeachersDocument3 pagesHealth Card TeachersRuselle N. NavarroNo ratings yet
- Contextualized SBM Tool 2021Document20 pagesContextualized SBM Tool 2021Ruselle N. NavarroNo ratings yet
- DLL - Mathematics 1 - Q1 - W8Document5 pagesDLL - Mathematics 1 - Q1 - W8Ruselle N. NavarroNo ratings yet
- DLL - Mapeh 1 - Q1 - W8Document4 pagesDLL - Mapeh 1 - Q1 - W8Ruselle N. NavarroNo ratings yet
- Equivalent Record Form Checklist 2021Document2 pagesEquivalent Record Form Checklist 2021Ruselle N. NavarroNo ratings yet
- DLL - MTB 1 - Q1 - W8Document4 pagesDLL - MTB 1 - Q1 - W8Ruselle N. NavarroNo ratings yet
- My Home A Sense of Identity Grade 2 Primary Level PDFDocument3 pagesMy Home A Sense of Identity Grade 2 Primary Level PDFRuselle N. NavarroNo ratings yet
- Math g4 m1 End of Module AssessmentDocument8 pagesMath g4 m1 End of Module AssessmentRuselle N. NavarroNo ratings yet
- Ipcrf For Teacher 1-3Document17 pagesIpcrf For Teacher 1-3Ruselle N. NavarroNo ratings yet
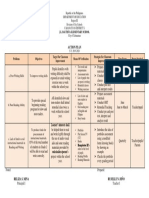
- Action Plan: J.L. Bautista Elementary SchoolDocument1 pageAction Plan: J.L. Bautista Elementary SchoolRuselle N. NavarroNo ratings yet
- Optimized Hemodynamic Therapy in Cardiac Surgery Patients: Length of ICU Stay ComplicationsDocument2 pagesOptimized Hemodynamic Therapy in Cardiac Surgery Patients: Length of ICU Stay ComplicationszomweNo ratings yet
- KSR International Membership Application Form - 201603 - WebsiteDocument2 pagesKSR International Membership Application Form - 201603 - Websiteseb2008No ratings yet
- Analysis of Veterinary Service Delivery in Uganda An Application of The Process Net-Map ToolDocument25 pagesAnalysis of Veterinary Service Delivery in Uganda An Application of The Process Net-Map ToolKYALIGONZA GEOFREYNo ratings yet
- A Prospective Observational Study On Drug Utilisation Evaluation of High Alert Drugs Used in A Tertiary Care HospitalDocument4 pagesA Prospective Observational Study On Drug Utilisation Evaluation of High Alert Drugs Used in A Tertiary Care HospitalBaru Chandrasekhar Rao0% (1)
- Master of Midwifery CourseworkDocument6 pagesMaster of Midwifery Courseworkf1vijokeheg3100% (2)
- Acute Coronary Syndrome PDFDocument8 pagesAcute Coronary Syndrome PDFVedranaJovanovicNo ratings yet
- Log Book GCFM MockDocument135 pagesLog Book GCFM Mocknurul asyikin abdullahNo ratings yet
- Technological University of The PhilippinesDocument5 pagesTechnological University of The PhilippinesIsha BalangueNo ratings yet
- Maternal and Foetal Outcomes in Pregnancy With Gestational Thrombocytopenia: A Prospective Observational StudyDocument6 pagesMaternal and Foetal Outcomes in Pregnancy With Gestational Thrombocytopenia: A Prospective Observational StudyIJAR JOURNALNo ratings yet
- Anaphylactic ShockDocument29 pagesAnaphylactic ShockHIND100% (7)
- Riverside County Teachers Union Letter To The Riverside County Office of EducationDocument2 pagesRiverside County Teachers Union Letter To The Riverside County Office of EducationBeau YarbroughNo ratings yet
- Universiti Teknologi Mara: Confidential LG/JULY 2021/ELC121/120 (SET 2)Document11 pagesUniversiti Teknologi Mara: Confidential LG/JULY 2021/ELC121/120 (SET 2)Dayah SuhaidiNo ratings yet
- Nano Soma SprayDocument10 pagesNano Soma SprayNano SomaNo ratings yet
- Informative EssayDocument5 pagesInformative EssayCharelle SolomonNo ratings yet
- Colic Keys PDFDocument8 pagesColic Keys PDFCristina GMNo ratings yet
- Tugas Bahasa Inggris 2Document6 pagesTugas Bahasa Inggris 2yuly sukmawatiNo ratings yet
- Revenue Cycle Management Comprehensive Solutions - 0Document4 pagesRevenue Cycle Management Comprehensive Solutions - 0avinashn1984No ratings yet
- Better Outcomes Lower Costs FSG&GIH Spring 2012Document18 pagesBetter Outcomes Lower Costs FSG&GIH Spring 2012iggybauNo ratings yet
- International Journal of Ophthalmology and Clinical Research Ijocr 5 088Document6 pagesInternational Journal of Ophthalmology and Clinical Research Ijocr 5 088Nurfarahin MustafaNo ratings yet
- Clinical and Ethical Consideration of PerimortemDocument76 pagesClinical and Ethical Consideration of Perimortemtata marethaNo ratings yet
- Facial Intake Form: Personal InformationDocument6 pagesFacial Intake Form: Personal InformationCrystal-Jae0% (1)
- Perspective: Plant-Based Eating Pattern For Type 2 Diabetes Prevention and Treatment: Efficacy, Mechanisms, and Practical ConsiderationsDocument11 pagesPerspective: Plant-Based Eating Pattern For Type 2 Diabetes Prevention and Treatment: Efficacy, Mechanisms, and Practical ConsiderationsdgmtfmNo ratings yet
- Application Form: Philippine Registry For Persons With Disabilities Version 4.0Document5 pagesApplication Form: Philippine Registry For Persons With Disabilities Version 4.0ANNA MARY GINTORONo ratings yet
- This Study Resource WasDocument4 pagesThis Study Resource WasMyra Cheriece MorrowNo ratings yet
- NURS FPX 6618 Assessment 1 Planning and Presenting A Care Coordination ProjectDocument6 pagesNURS FPX 6618 Assessment 1 Planning and Presenting A Care Coordination Projectzadem5266No ratings yet
- Diseases of Digestive SystemDocument87 pagesDiseases of Digestive SystemEdgar Jr. CustodioNo ratings yet
- Fetalix: Fetal-Inspired Biomaterials For IVD RegenerationDocument13 pagesFetalix: Fetal-Inspired Biomaterials For IVD RegenerationHugo PrazeresNo ratings yet
- I. Ethical Consideration in Leadership and Management A. Moral Decision MakingDocument12 pagesI. Ethical Consideration in Leadership and Management A. Moral Decision MakingJessa Mae OhaoNo ratings yet