You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5796)
- Advances in Studies of P Glycoprotein and Its Expression Regulators - 2018Document9 pagesAdvances in Studies of P Glycoprotein and Its Expression Regulators - 2018Aline DantasNo ratings yet
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Ervas e Especiarias Com Propriedades AntioxidantesDocument8 pagesErvas e Especiarias Com Propriedades AntioxidantesAline DantasNo ratings yet
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- Composi Æo Da Microbiota e Metila Æo de Genes Relacionados ObesidadeDocument9 pagesComposi Æo Da Microbiota e Metila Æo de Genes Relacionados ObesidadeAline DantasNo ratings yet
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Bisfenol e ObesidadeDocument23 pagesBisfenol e ObesidadeAline DantasNo ratings yet
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- Artigo Obesidade Contribui Äes de BlackburnDocument25 pagesArtigo Obesidade Contribui Äes de BlackburnAline DantasNo ratings yet
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- HPA Axis Dysregulation and Cortisol Activity in Obesity 2015Document18 pagesHPA Axis Dysregulation and Cortisol Activity in Obesity 2015Aline DantasNo ratings yet
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (400)
- With A Little Help From My Friends-The Role of Microbiota in Thyroid Hormone 2017Document5 pagesWith A Little Help From My Friends-The Role of Microbiota in Thyroid Hormone 2017Aline DantasNo ratings yet
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- EVS Assignment Question by Vedant Nagpal Answer 03Document1 pageEVS Assignment Question by Vedant Nagpal Answer 03Vedant NagpalNo ratings yet
- Topic 4.4 FormativeDocument2 pagesTopic 4.4 FormativebubbleteaNo ratings yet
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (589)
- Consti 4 PDFDocument110 pagesConsti 4 PDFRenceNo ratings yet
- Allied American University Online Course CatalogDocument89 pagesAllied American University Online Course CatalogAllied American University100% (1)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- 2012 RWCID Non-Resident Pool MembershipDocument1 page2012 RWCID Non-Resident Pool MembershipBrett Lord-CastilloNo ratings yet
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- Formative Assessment Impact of IrDocument3 pagesFormative Assessment Impact of Irapi-738511179No ratings yet
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- Dbrac1120315 Ovm TMPLT Test Config 2751661Document42 pagesDbrac1120315 Ovm TMPLT Test Config 2751661ganesh_24No ratings yet
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Statement of Account: Date Narration Chq./Ref - No. Value DT Withdrawal Amt. Deposit Amt. Closing BalanceDocument2 pagesStatement of Account: Date Narration Chq./Ref - No. Value DT Withdrawal Amt. Deposit Amt. Closing BalanceLoan LoanNo ratings yet
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (345)
- Saurashtra University B. Sc. IT (English) 2019Document3 pagesSaurashtra University B. Sc. IT (English) 2019Aditya PatelNo ratings yet
- ITCE419 - Final ExamDocument5 pagesITCE419 - Final ExamKANSNNo ratings yet
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- ELS Practice Exam 7Document17 pagesELS Practice Exam 7Deniz ElçinNo ratings yet
- Graphene-Based Conducting Inks 2Document3 pagesGraphene-Based Conducting Inks 2VishnuTejaChundiNo ratings yet
- 2021 Camanche Recreation Use FeesDocument9 pages2021 Camanche Recreation Use FeesBrian HarrisonNo ratings yet
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Consumer Buying Behavior Toeards Milk ProductDocument54 pagesConsumer Buying Behavior Toeards Milk ProductsuyoganuNo ratings yet
- Tutorial 06 Questions With Possible Solutions: IS333: Project Management - Semester I 2021Document5 pagesTutorial 06 Questions With Possible Solutions: IS333: Project Management - Semester I 2021Chand DivneshNo ratings yet
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1091)
- Tuner Studio App DebugDocument516 pagesTuner Studio App DebugFiv5ren MusicNo ratings yet
- Aeronautical Chart Users' Guide VFR Charting Products (Includes Sectional, Terminal Area, Caribbean, Flyway, and Helicopter Charts)Document61 pagesAeronautical Chart Users' Guide VFR Charting Products (Includes Sectional, Terminal Area, Caribbean, Flyway, and Helicopter Charts)MuhammadHassanBashirNo ratings yet
- BF PresentationDocument7 pagesBF PresentationWeb NovelNo ratings yet
- Oleg A. Starykh, Andrey V. Chubukov and Alexander G. Abanov - Flat Spin-Wave Dispersion in A Triangular AntiferromagnetDocument4 pagesOleg A. Starykh, Andrey V. Chubukov and Alexander G. Abanov - Flat Spin-Wave Dispersion in A Triangular AntiferromagnetGravvolNo ratings yet
- Traffic Freelancer FileDocument10 pagesTraffic Freelancer FileHsNo ratings yet
- 10 Typografi - Font KOKOHDocument1 page10 Typografi - Font KOKOHFarchan All in oneNo ratings yet
- Refresher Module - Surveying (Earthworks) : Methods of Calculating VolumeDocument2 pagesRefresher Module - Surveying (Earthworks) : Methods of Calculating VolumeOctavia BlakeNo ratings yet
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- Justice Brion's Penned CasesDocument409 pagesJustice Brion's Penned CasesKeking XoniuqeNo ratings yet
- Painting System No.: SSPC: The Society For Protective CoatingsDocument2 pagesPainting System No.: SSPC: The Society For Protective CoatingsanoopkumarNo ratings yet
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- DLP VIII How Land Masses and Bodies of Water Affects The TyphoonDocument5 pagesDLP VIII How Land Masses and Bodies of Water Affects The TyphoonNellen Bastismo100% (1)
- Year Date Year Date Discharge (M /S) Gauge Height (M) Discharge (M /S) Gauge Height (M)Document3 pagesYear Date Year Date Discharge (M /S) Gauge Height (M) Discharge (M /S) Gauge Height (M)Rajib MaharjanNo ratings yet
- Skill Trees 1-6-23 (40594786)Document21 pagesSkill Trees 1-6-23 (40594786)Scribble StixNo ratings yet
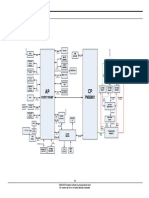
- Samsung GT-P1000 Galaxy Tab Level 3 Service ManualDocument49 pagesSamsung GT-P1000 Galaxy Tab Level 3 Service ManualabdelNo ratings yet
- Dawit Tesfai ResumeDocument4 pagesDawit Tesfai Resumeapi-444700983No ratings yet
- James Tyler Variax User Manual (Rev C) - FrenchDocument14 pagesJames Tyler Variax User Manual (Rev C) - Frenchwolfen667No ratings yet