You might also like
- GuaifenesinDocument2 pagesGuaifenesincoooleNo ratings yet
- Acetylcysteine: Mucolytic Adult: Inhalation 1-10 ML of 20% Solution q4-6h or 2-20 ML of 10%Document3 pagesAcetylcysteine: Mucolytic Adult: Inhalation 1-10 ML of 20% Solution q4-6h or 2-20 ML of 10%Aubrey Unique EvangelistaNo ratings yet
- ACETYLCYSTEINEDocument2 pagesACETYLCYSTEINEAubrey Unique EvangelistaNo ratings yet
- Drug StudyDocument7 pagesDrug Studykamirure02No ratings yet
- Cough 2020Document51 pagesCough 2020Noor SiddiquiNo ratings yet
- Note On Asthma in AdultDocument5 pagesNote On Asthma in Adultshivam1969No ratings yet
- Clinical Case Ent by Dr. NiazDocument37 pagesClinical Case Ent by Dr. NiazSiddiqur Rahman AkashNo ratings yet
- Antipyretics: Instiaty Tropical Infection Module 2017-2018 Dept of Pharmacology and Therapeutics FkuiDocument22 pagesAntipyretics: Instiaty Tropical Infection Module 2017-2018 Dept of Pharmacology and Therapeutics Fkuisalsa2506No ratings yet
- CececeDocument57 pagesCececeBSRT1A BERBANO, IAN JEWEL M.No ratings yet
- Cough, Cold and AllergiesDocument68 pagesCough, Cold and AllergiesLeonardo RanderNo ratings yet
- DrugmedsDocument52 pagesDrugmedsshirleyNo ratings yet
- Drug Administration 2011Document98 pagesDrug Administration 2011bagir_dm10No ratings yet
- Hard Copy Sublingual FinalDocument7 pagesHard Copy Sublingual FinalRaya Ibarra LumogdangNo ratings yet
- Generic Name: Propiverine HCl Brand Name: Mictonorm Classification: Urinary AntispasmodicDocument7 pagesGeneric Name: Propiverine HCl Brand Name: Mictonorm Classification: Urinary AntispasmodicMaRic Gabutin Guerra100% (1)
- Medications for Pain ManagementDocument8 pagesMedications for Pain ManagementapalestiNo ratings yet
- Nursing Pharmacology HandoutsDocument10 pagesNursing Pharmacology HandoutsMICHAELA TIMBOLNo ratings yet
- Drug StudyDocument186 pagesDrug StudyTheresa Sombilla FacunlaNo ratings yet
- LPRD in Children: Journal Reading Tita Puspitasari Supervisor: Dr. Ongka M. Saifuddin, SPTHT-KL (K)Document22 pagesLPRD in Children: Journal Reading Tita Puspitasari Supervisor: Dr. Ongka M. Saifuddin, SPTHT-KL (K)TitaPuspitasariNo ratings yet
- LPRD in Children: Journal Reading Tita Puspitasari Supervisor: Dr. Ongka M. Saifuddin, SPTHT-KL (K)Document22 pagesLPRD in Children: Journal Reading Tita Puspitasari Supervisor: Dr. Ongka M. Saifuddin, SPTHT-KL (K)TitaPuspitasariNo ratings yet
- GIT AgentsDocument51 pagesGIT AgentsEimhie Lee CasiNo ratings yet
- Drug Studies PsychDocument12 pagesDrug Studies PsychAnna Mendiola-BasbasNo ratings yet
- Drug CardsDocument11 pagesDrug CardsLizShermanNo ratings yet
- DrugsDocument5 pagesDrugsdeepika kushwah100% (1)
- ENTDocument1 pageENTAbdullaNo ratings yet
- Bronchodilators Guide for Asthma and COPDDocument5 pagesBronchodilators Guide for Asthma and COPDdeepika kushwahNo ratings yet
- Bronchial AsthmaDocument45 pagesBronchial Asthmaprincesszahra6498No ratings yet
- The Common Cold GuideDocument27 pagesThe Common Cold Guidehappyscottlee3438No ratings yet
- Common Pediatric Illnesses in The Er UrgentDocument46 pagesCommon Pediatric Illnesses in The Er UrgentDr mohamedNo ratings yet
- PEDI PEARLS: Dr. Cortes Guide to Common Pediatric Respiratory IssuesDocument46 pagesPEDI PEARLS: Dr. Cortes Guide to Common Pediatric Respiratory Issuesthomasfx10100% (1)
- MS RESPIbfrDocument13 pagesMS RESPIbfrEmeroot RootNo ratings yet
- EpilepsyDocument30 pagesEpilepsyabirami pNo ratings yet
- Classification (S) Therapeutic: Anti-Infectives Pharmacologic: FluoroquinolonesDocument9 pagesClassification (S) Therapeutic: Anti-Infectives Pharmacologic: FluoroquinolonesFildehl Janice Bomediano CatipayNo ratings yet
- Anatomy of the Upper Respiratory TractDocument7 pagesAnatomy of the Upper Respiratory TractGladys NacionNo ratings yet
- Salivary Gland: Prepared and Presented By: DR - Zafar Iqbal AhmedDocument23 pagesSalivary Gland: Prepared and Presented By: DR - Zafar Iqbal AhmedTajammul Rizwan KhattakNo ratings yet
- Chlorpromazine Drug StudyDocument7 pagesChlorpromazine Drug Studyjennachristy03100% (3)
- Six rights medication administrationDocument4 pagesSix rights medication administrationKayla CicciaNo ratings yet
- ANTICHOLINERGIC GROUP 7 PharmDocument21 pagesANTICHOLINERGIC GROUP 7 PharmDavid MharkNo ratings yet
- AtroventDocument1 pageAtroventSheri490100% (1)
- 2nd Drug StudyDocument39 pages2nd Drug StudyYanna Habib-Mangotara100% (3)
- Farmakoterapi Sistem Pencernaan Diare Konstipasi HepatitisDocument77 pagesFarmakoterapi Sistem Pencernaan Diare Konstipasi HepatitisRefika FahruNo ratings yet
- CH 54 UpperDocument41 pagesCH 54 UpperKate Angelique RodriguezNo ratings yet
- SalbutamolDocument1 pageSalbutamolMonica Lyka BancaleNo ratings yet
- Dengue: Subjective FindingsDocument5 pagesDengue: Subjective FindingsRaghu VenkatNo ratings yet
- Atropine SulfateDocument5 pagesAtropine Sulfateapi-3797941100% (1)
- General AnaesthesiaDocument5 pagesGeneral Anaesthesiayogesh.sontakke4487No ratings yet
- 02 Respi EmergenciesDocument133 pages02 Respi EmergenciesLizeil VelardeNo ratings yet
- Budesonide (Drug Study)Document3 pagesBudesonide (Drug Study)Franz.thenurse6888No ratings yet
- Drugs For CoughDocument18 pagesDrugs For CoughAbraham BanjoNo ratings yet
- b7 PPT, AntihistaminesDocument56 pagesb7 PPT, AntihistaminesKeziah GillNo ratings yet
- Key Drug Information: AlbuterolDocument1 pageKey Drug Information: Albuterolamaliea234No ratings yet
- BudesonideDocument4 pagesBudesonideapi-3797941No ratings yet
- Antitusif Dan Nasal DecongestantDocument32 pagesAntitusif Dan Nasal DecongestantPutri PrimandiniNo ratings yet
- Colds 2020Document72 pagesColds 2020Noor SiddiquiNo ratings yet
- Common Cases in Ambulatory Care Clinic For Lu6Document106 pagesCommon Cases in Ambulatory Care Clinic For Lu6Joy SantosNo ratings yet
- 2nd Generation AntihistamineDocument4 pages2nd Generation AntihistamineJohn Christopher LucesNo ratings yet
- BKP L1-L4 CH419-2024Document99 pagesBKP L1-L4 CH419-2024randomvideos0011No ratings yet
- Baby healthcare essentials guideDocument62 pagesBaby healthcare essentials guiderohitNo ratings yet
- NLM MedicatingDocument11 pagesNLM MedicatingQuimberly ModequilloNo ratings yet
- Serotonin (5-HT3) Antagonist: Ondansetron SucralfateDocument6 pagesSerotonin (5-HT3) Antagonist: Ondansetron SucralfateLola LeNo ratings yet
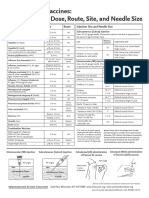
- Administering Vaccines: Dose, Route, Site and Needle Size GuideDocument1 pageAdministering Vaccines: Dose, Route, Site and Needle Size GuideKate Lucernas MayugaNo ratings yet
- Glucocorticoid Induced Adrenal Insufficiency Prete2021Document20 pagesGlucocorticoid Induced Adrenal Insufficiency Prete2021Marcos OrtizNo ratings yet
- Glenmark DataDocument3 pagesGlenmark DataPushpendra DixitNo ratings yet
- Antipsychotic Drugs: Eduviere A.TDocument19 pagesAntipsychotic Drugs: Eduviere A.TOmaraye JoshuaNo ratings yet
- Module 3 NSTP1 FinalDocument7 pagesModule 3 NSTP1 FinalFrank PintoNo ratings yet
- Analgesicos/Antitermicos: Jarabe 125mg/5mlDocument6 pagesAnalgesicos/Antitermicos: Jarabe 125mg/5mlMaria Belen AguilarNo ratings yet
- Anti-Hypertensive Agents: Beverlee R. Gamiao-Torida MDDocument14 pagesAnti-Hypertensive Agents: Beverlee R. Gamiao-Torida MDBeb Raquel GamiaoNo ratings yet
- Adderall Research PaperDocument6 pagesAdderall Research Paperapi-316769369100% (3)
- TetracyclinesChloramphenicolMechanismsUsesEffectsDocument29 pagesTetracyclinesChloramphenicolMechanismsUsesEffectsArun DavesarNo ratings yet
- Drug Discovery Complete NotesDocument5 pagesDrug Discovery Complete NotesSadiqa ForensicNo ratings yet
- Antidotes and Their UsesDocument3 pagesAntidotes and Their UsesAbdul SalamNo ratings yet
- Clinical Pharma ExamDocument4 pagesClinical Pharma Examnancy voraNo ratings yet
- LidocaineDocument3 pagesLidocaineNovella MannuelaNo ratings yet
- Anti FUNGAL Drugs PDFDocument70 pagesAnti FUNGAL Drugs PDFHester Marie SimpiaNo ratings yet
- EP LatestDocument83 pagesEP LatestramaiaNo ratings yet
- Hypnotics SedDocument13 pagesHypnotics SedSamantha ReyesNo ratings yet
- Drug Study: PART 1: To Be Completed Prior To Clinical ExperienceDocument5 pagesDrug Study: PART 1: To Be Completed Prior To Clinical ExperienceFrozanSNo ratings yet
- Final Management of Allergic RhinitisDocument80 pagesFinal Management of Allergic RhinitisgimamrNo ratings yet
- Top 200 Drugs To MemorizeDocument6 pagesTop 200 Drugs To MemorizeJuan Fran HernandezNo ratings yet
- 11 Medicine Inventory Nov 2015Document17 pages11 Medicine Inventory Nov 2015BadboyNo ratings yet
- Prozac and PaxilDocument6 pagesProzac and PaxilSmritiNo ratings yet
- Penyesuaian Dosis Regimen Pada Pasien Dengan Gangguan Fungsi GinjalDocument19 pagesPenyesuaian Dosis Regimen Pada Pasien Dengan Gangguan Fungsi GinjalChamidRiyadiNo ratings yet
- NarcoticsDocument6 pagesNarcoticsanaeshkl100% (1)
- PainDocument90 pagesPainmikErlh100% (4)
- Assignment 3Document5 pagesAssignment 3Samantha PargadNo ratings yet
- Dispensadores Bigfarma1Document5 pagesDispensadores Bigfarma1Milagros AliffNo ratings yet
- ReviewerDocument20 pagesReviewerKC PalattaoNo ratings yet
- Libro Quimica Opcion Quimica Medica PDFDocument102 pagesLibro Quimica Opcion Quimica Medica PDFJose A Suarez RNo ratings yet
- Routes of Drug AdministrationDocument107 pagesRoutes of Drug AdministrationChrislyn Sanlao100% (4)