You might also like
- Effects of Facemask Treatment Anchored With Miniplates After Alternate Rapid Maxillary Expansions and Constrictions A Pilot StudyDocument8 pagesEffects of Facemask Treatment Anchored With Miniplates After Alternate Rapid Maxillary Expansions and Constrictions A Pilot StudyMariana SantosNo ratings yet
- Dentofacial Effects of Two Facemask Therapies For Maxillary Protraction Miniscrew Implants Versus Rapid Maxillary ExpandersDocument9 pagesDentofacial Effects of Two Facemask Therapies For Maxillary Protraction Miniscrew Implants Versus Rapid Maxillary ExpandersMariana SantosNo ratings yet
- Correction of Late Adolescent Skeletal Class III Using The Alt-RAMEC Protocol and Skeletal AnchorageDocument11 pagesCorrection of Late Adolescent Skeletal Class III Using The Alt-RAMEC Protocol and Skeletal AnchoragePorchiddioNo ratings yet
- 1 s2.0 S2666430522000036 MainDocument12 pages1 s2.0 S2666430522000036 MainDANTE DELEGUERYNo ratings yet
- Kaya 2011Document8 pagesKaya 2011ortodoncia 2022No ratings yet
- Benedict Wimes, Mascara FacialDocument8 pagesBenedict Wimes, Mascara FacialjamilistccNo ratings yet
- Rapid Maxillary Expansion Compared To Surgery For Assistance in Maxillary Face Mask ProtractionDocument8 pagesRapid Maxillary Expansion Compared To Surgery For Assistance in Maxillary Face Mask ProtractionMariana SantosNo ratings yet
- Three-Dimensional Evaluation of Hybrid Expander Appliances: A Pilot StudyDocument6 pagesThree-Dimensional Evaluation of Hybrid Expander Appliances: A Pilot Studydruzair007No ratings yet
- 2176 9451 Dpjo 24 05 52Document8 pages2176 9451 Dpjo 24 05 52Crisu CrisuuNo ratings yet
- New Treatment Modality For Maxillary Hypoplasia in Cleft PatientsDocument9 pagesNew Treatment Modality For Maxillary Hypoplasia in Cleft PatientsKaranPadhaNo ratings yet
- Comparison of Root Resorption After Bone-Borne and Tooth-Borne Rapid Maxillary Expansion Evaluated With The Use of MicrotomographyDocument9 pagesComparison of Root Resorption After Bone-Borne and Tooth-Borne Rapid Maxillary Expansion Evaluated With The Use of MicrotomographyMonojit DuttaNo ratings yet
- Yildirim2019 PDFDocument9 pagesYildirim2019 PDFMonojit DuttaNo ratings yet
- Sarah Salah PaperDocument14 pagesSarah Salah PaperdentistsurorNo ratings yet
- Effectiveness of Maxillary Protraction Using A Hybrid Hyrax-Facemask Combination: A Controlled Clinical StudyDocument7 pagesEffectiveness of Maxillary Protraction Using A Hybrid Hyrax-Facemask Combination: A Controlled Clinical StudyKarin UchimaNo ratings yet
- Roll Man 2013Document6 pagesRoll Man 2013SergioNo ratings yet
- 2010-Three Dimensional Analysis of Maxillary Protraction WithDocument22 pages2010-Three Dimensional Analysis of Maxillary Protraction WithMariana SantosNo ratings yet
- ExpansãoDocument4 pagesExpansãoMiguel OcanhaNo ratings yet
- Schropp Et Al (2005) Immediate Vs Delayed IJOMIDocument9 pagesSchropp Et Al (2005) Immediate Vs Delayed IJOMIAlla MushkeyNo ratings yet
- Schropp Et Al (2005) Immediate Vs Delayed IJOMI PDFDocument9 pagesSchropp Et Al (2005) Immediate Vs Delayed IJOMI PDFAlla MushkeyNo ratings yet
- ALTRAMECARTICULODocument12 pagesALTRAMECARTICULOAlejandra NietoNo ratings yet
- Angle Orthod. 2012 82 5 846-52Document7 pagesAngle Orthod. 2012 82 5 846-52brookortontiaNo ratings yet
- JCDP 22 1135Document9 pagesJCDP 22 1135Thang Nguyen TienNo ratings yet
- International Journal of Surgery Case Reports: Kanistika Jha, Manoj AdhikariDocument4 pagesInternational Journal of Surgery Case Reports: Kanistika Jha, Manoj AdhikariYeraldin EspañaNo ratings yet
- Tejido Conectivo Implantes Inmediatos y Provisionales 2Document9 pagesTejido Conectivo Implantes Inmediatos y Provisionales 2James Alexander Toruño GordonNo ratings yet
- 2000 J C. H S W A: Udson Ickey Cientific Riting WardDocument6 pages2000 J C. H S W A: Udson Ickey Cientific Riting WardPremshith CpNo ratings yet
- Ajodo 3Document10 pagesAjodo 3ayisNo ratings yet
- Angle Orthod. 2016 86 5 746-52Document7 pagesAngle Orthod. 2016 86 5 746-52brookortontiaNo ratings yet
- Surgically Assisted Rapid Maxillary Expansion Combined With MaxillaryDocument21 pagesSurgically Assisted Rapid Maxillary Expansion Combined With MaxillaryKumar NiwalikarNo ratings yet
- 7 Articulo Bone-Anchored Maxillary Protraction in A Patient With Complete Cleft Lip and Palate: A Case ReportDocument8 pages7 Articulo Bone-Anchored Maxillary Protraction in A Patient With Complete Cleft Lip and Palate: A Case ReportErika NuñezNo ratings yet
- Dentofacial Effects of Modified Alt-RAMEC Protocol Combined With The Facial Mask For Treatment of Preadolescent Caucasian Class III PatientsDocument7 pagesDentofacial Effects of Modified Alt-RAMEC Protocol Combined With The Facial Mask For Treatment of Preadolescent Caucasian Class III PatientsMariana SantosNo ratings yet
- Assessment of Changes in The Nasal Airway After Nonsurgical Miniscrew-Assisted Rapid Maxillary Expansion in Young Adults.Document8 pagesAssessment of Changes in The Nasal Airway After Nonsurgical Miniscrew-Assisted Rapid Maxillary Expansion in Young Adults.Natan GussNo ratings yet
- Maxillary Expansion AppliancesDocument8 pagesMaxillary Expansion Appliancesmotivation munkeyNo ratings yet
- 2020 Article 265Document7 pages2020 Article 265Fabian BarretoNo ratings yet
- Three-Dimensional Soft Tissue Evaluation After Rapid Maxillary Expansion and Mandibular Midline Distraction OsteogenesisDocument7 pagesThree-Dimensional Soft Tissue Evaluation After Rapid Maxillary Expansion and Mandibular Midline Distraction OsteogenesisayisNo ratings yet
- Ajodo 1Document7 pagesAjodo 1ayis100% (1)
- Comparison of Two Protocols For Maxillary Protraction: Bone Anchors Versus Face Mask With Rapid Maxillary ExpansionDocument8 pagesComparison of Two Protocols For Maxillary Protraction: Bone Anchors Versus Face Mask With Rapid Maxillary ExpansionBeatriz ChilenoNo ratings yet
- Borgia Gonzalo, Ravecca Tabaré, Fumero Miriam, Pebé PabloDocument13 pagesBorgia Gonzalo, Ravecca Tabaré, Fumero Miriam, Pebé PabloJaime Angel Ortiz DiazNo ratings yet
- Bong 2011 PDFDocument14 pagesBong 2011 PDFkarenchavezalvanNo ratings yet
- Nonsurgical Correction of A Class III Malocclusion in An Adult by Miniscrew-Assisted Mandibular Dentition DistalizationDocument11 pagesNonsurgical Correction of A Class III Malocclusion in An Adult by Miniscrew-Assisted Mandibular Dentition DistalizationNeycer Catpo NuncevayNo ratings yet
- Journal of Surgery and Insights: Transpalatal Distraction As A Method of Maxillary Expansion: A Case ReportDocument4 pagesJournal of Surgery and Insights: Transpalatal Distraction As A Method of Maxillary Expansion: A Case ReportjabbarNo ratings yet
- 2011-Orthopedic Treatment of Class III Malocclusion With Rapid Maxillary Expansion Combined With A Face Mask A Cephalometric Assessment of Craniofacial Growth PatternsDocument7 pages2011-Orthopedic Treatment of Class III Malocclusion With Rapid Maxillary Expansion Combined With A Face Mask A Cephalometric Assessment of Craniofacial Growth PatternsMariana SantosNo ratings yet
- Scientific Dental Journal: Lower Facial Height and Soft Tissue Changes in Bimaxillary Protrusion CasesDocument7 pagesScientific Dental Journal: Lower Facial Height and Soft Tissue Changes in Bimaxillary Protrusion Casesyuni madjidNo ratings yet
- APOSTrendsOrthod 2016 6 4 228 186439 PDFDocument5 pagesAPOSTrendsOrthod 2016 6 4 228 186439 PDFDr sneha HoshingNo ratings yet
- Abbé - EstlanderDocument4 pagesAbbé - EstlanderKoretta Esmeral AtehortúaNo ratings yet
- Angle Orthod. 2015 85 2 284-91Document8 pagesAngle Orthod. 2015 85 2 284-91brookortontiaNo ratings yet
- Treatment Effects After Maxillary Expansion Using Tooth-Borne Vs Tissue-Borne Miniscrew-Assisted Rapid Palatal Expansion ApplianceDocument9 pagesTreatment Effects After Maxillary Expansion Using Tooth-Borne Vs Tissue-Borne Miniscrew-Assisted Rapid Palatal Expansion ApplianceRolando Huaman BravoNo ratings yet
- Lanza 2017Document7 pagesLanza 2017Promocoes PromoNo ratings yet
- Articol PMFDocument6 pagesArticol PMFclaudia lupuNo ratings yet
- Australian Dental Journal: Craniofacial DisordersDocument11 pagesAustralian Dental Journal: Craniofacial DisordersMantili TasrifNo ratings yet
- 2021 Does The Timing of 1-Stage Palatoplasty With Radical Muscle Dissection Effect Long-Term Midface Growth A Single-Center Retrospective AnalysisDocument7 pages2021 Does The Timing of 1-Stage Palatoplasty With Radical Muscle Dissection Effect Long-Term Midface Growth A Single-Center Retrospective AnalysisDimitris RodriguezNo ratings yet
- Alt Ramec - Estructuras DentalesDocument8 pagesAlt Ramec - Estructuras DentalesAna Clara ClaveroNo ratings yet
- Miniscrew-Assisted Rapid Palatal Expansion For Managing Arch Perimeter in An Adult PatientDocument12 pagesMiniscrew-Assisted Rapid Palatal Expansion For Managing Arch Perimeter in An Adult PatientAkash AmbhoreNo ratings yet
- Brandt2013 MDocument4 pagesBrandt2013 MAnkita GuravNo ratings yet
- Maxillary ExpansionDocument8 pagesMaxillary ExpansionJoji IsacNo ratings yet
- Mohammed 2019Document29 pagesMohammed 2019RafailiaNo ratings yet
- Case Report Treatment of An Adult Skeletal Class III Patient With Surgically Assisted Rapid Palatal Expansion and FacemaskDocument7 pagesCase Report Treatment of An Adult Skeletal Class III Patient With Surgically Assisted Rapid Palatal Expansion and FacemaskMirza GlusacNo ratings yet
- Mini-Implant Assisted Rapid Palatal Expansion: New PerspectivesDocument18 pagesMini-Implant Assisted Rapid Palatal Expansion: New PerspectivesKhyati GuptaNo ratings yet
- Maxillary Arch Distalization Using Interradicular Miniscrews and The Lever-Arm ApplianceDocument8 pagesMaxillary Arch Distalization Using Interradicular Miniscrews and The Lever-Arm ApplianceJuan Carlos CárcamoNo ratings yet
- Rapid Maxillary Expansion. Is It Better in The Mixed or in The Permanent Dentition?Document8 pagesRapid Maxillary Expansion. Is It Better in The Mixed or in The Permanent Dentition?Gustavo AnteparraNo ratings yet
- Coating With Zelodronic AcidDocument30 pagesCoating With Zelodronic AcidZaid DewachiNo ratings yet
- NCBIDocument13 pagesNCBIZaid DewachiNo ratings yet
- Study of Erosive Alterations in Dental Enamel Exposed To Medicinal SyrupsDocument3 pagesStudy of Erosive Alterations in Dental Enamel Exposed To Medicinal SyrupsZaid DewachiNo ratings yet
- Non-Surgical Treatment of Class III With Multiloop Edgewise Arch-Wire (MEAW) TherapyDocument22 pagesNon-Surgical Treatment of Class III With Multiloop Edgewise Arch-Wire (MEAW) TherapyZaid DewachiNo ratings yet
- Kjod 48 236Document9 pagesKjod 48 236Zaid DewachiNo ratings yet
- Tjo-29-2-4-91 Very ImportantDocument7 pagesTjo-29-2-4-91 Very ImportantZaid DewachiNo ratings yet
- Luki Gummetal W Ortodoncji 0Document16 pagesLuki Gummetal W Ortodoncji 0Zhiao Liu100% (1)
- Comparative Reliability Assessment of Tooth VolumeDocument12 pagesComparative Reliability Assessment of Tooth VolumeZaid DewachiNo ratings yet
- Straight Wire PIODocument16 pagesStraight Wire PIOZaid DewachiNo ratings yet
- Nackaerts 2014Document10 pagesNackaerts 2014Zaid DewachiNo ratings yet
- Cui ToothNet Automatic Tooth Instance Segmentation and Identification From Cone Beam CVPR 2019 PaperDocument10 pagesCui ToothNet Automatic Tooth Instance Segmentation and Identification From Cone Beam CVPR 2019 PaperZaid DewachiNo ratings yet
- Accuracy of in Vitro Mandibular Volumetric Measurements From CBCT of Different Voxel Sizes With Different Segmentation Threshold SettingsDocument7 pagesAccuracy of in Vitro Mandibular Volumetric Measurements From CBCT of Different Voxel Sizes With Different Segmentation Threshold SettingsZaid DewachiNo ratings yet
- Discuss 3Document7 pagesDiscuss 3Zaid DewachiNo ratings yet
- Ne 2Document7 pagesNe 2Zaid DewachiNo ratings yet
- Enoxaparin - Safe Prescribing - Check It Out 1Document3 pagesEnoxaparin - Safe Prescribing - Check It Out 1Zaid DewachiNo ratings yet
- Drishti Software Installation ManualDocument12 pagesDrishti Software Installation ManualZaid DewachiNo ratings yet
- Relationship Between Midpalatal Suture MaturationDocument6 pagesRelationship Between Midpalatal Suture MaturationZaid DewachiNo ratings yet
- Ne 3Document8 pagesNe 3Zaid DewachiNo ratings yet
- StemcellreviewinorthoDocument13 pagesStemcellreviewinorthoZaid DewachiNo ratings yet
- Skeletal and Dental Considerations in OrthodonticDocument11 pagesSkeletal and Dental Considerations in OrthodonticZaid DewachiNo ratings yet
- Laser Doopler Perfusi̇on İmagerDocument4 pagesLaser Doopler Perfusi̇on İmagerAli ÖzdemirNo ratings yet
- Ofertas Buen Fin SulkaDocument76 pagesOfertas Buen Fin SulkaCarlos QuirozNo ratings yet
- Physical Fitness CertificateDocument1 pagePhysical Fitness CertificateKavisa Ghosh85% (20)
- First Aid ChecklistDocument1 pageFirst Aid ChecklistGopal Choudhary0% (1)
- Ventstar Helix Heated Pi 9102433 enDocument8 pagesVentstar Helix Heated Pi 9102433 enDikka AzizNo ratings yet
- Accredited Colleges of Veterinary Medicine: Section 12.11Document5 pagesAccredited Colleges of Veterinary Medicine: Section 12.11ਰੋਹਿਤ ਬਾਵਾNo ratings yet
- Niva HSL Mediclaim Ghi Gpa Ss v3Document2 pagesNiva HSL Mediclaim Ghi Gpa Ss v3bradburywillsNo ratings yet
- Phar Assignment MR Sim V1.22Document3 pagesPhar Assignment MR Sim V1.22Kristoff Cardenas-RamosNo ratings yet
- CCH210604I83 Recibidas 2021 11 FacturasDocument42 pagesCCH210604I83 Recibidas 2021 11 FacturasAlexis Julian FloresNo ratings yet
- Hemophilia Powerpoint-Kuliah FKIK UNTANDocument33 pagesHemophilia Powerpoint-Kuliah FKIK UNTANAgung TriatmojoNo ratings yet
- Herbs, Laboratories, and RevolDocument15 pagesHerbs, Laboratories, and Revolhung tsung jenNo ratings yet
- DrugDocument90 pagesDrugamalia noviyantiNo ratings yet
- Bumil Anemia KekDocument7 pagesBumil Anemia KekRita WahyuningsihNo ratings yet
- Filehost - Professional English in Use MedicineDocument262 pagesFilehost - Professional English in Use MedicineCosmin Berechet0% (2)
- Taking-Patient-History-British-English-StudentDocument8 pagesTaking-Patient-History-British-English-Studentdr.huongnguyen.geneticsNo ratings yet
- Model Kemitraan Puskesmas-Praktisi Swasta Dalam Penanggulangan Tuberkulosis Paru Di Kecamatan Kalasan, Kabupaten Sleman, Provinsi DiyDocument9 pagesModel Kemitraan Puskesmas-Praktisi Swasta Dalam Penanggulangan Tuberkulosis Paru Di Kecamatan Kalasan, Kabupaten Sleman, Provinsi DiyDesvolim DesoNo ratings yet
- Brosur Pelayanan LaboratoriumDocument1 pageBrosur Pelayanan LaboratoriumChristian OktavianoNo ratings yet
- New Instructor Application: MEDIC FIRST AID International, IncDocument2 pagesNew Instructor Application: MEDIC FIRST AID International, IncjhoniNo ratings yet
- Đề Thi Tuyển Sinh Vào Lớp 10 Chuyên Anh – Trường THPT Chuyên NGUYỄN DU – Năm Học 2015-2016 – LonggleDocument8 pagesĐề Thi Tuyển Sinh Vào Lớp 10 Chuyên Anh – Trường THPT Chuyên NGUYỄN DU – Năm Học 2015-2016 – LongglerolandvietnamNo ratings yet
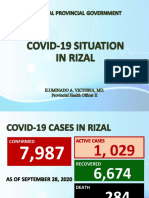
- Covid19 Situation in RizalDocument23 pagesCovid19 Situation in RizalToni Quitalig GamezNo ratings yet
- List of Hospitals Under Bombay Nursing Home Act - Patoda BlockDocument1 pageList of Hospitals Under Bombay Nursing Home Act - Patoda BlockCampaign MediaNo ratings yet
- Dissecting The Opioid Heroin Epidemic To Discover Its Ugly RootsDocument7 pagesDissecting The Opioid Heroin Epidemic To Discover Its Ugly RootsThavamNo ratings yet
- ახალშობილის მოვლაDocument28 pagesახალშობილის მოვლაNino KochuashviliNo ratings yet
- Asia TestDocument7 pagesAsia TestAsheNo ratings yet
- Stent Pricing: S. NO. Stent Discription Cost To Patient CompanyDocument1 pageStent Pricing: S. NO. Stent Discription Cost To Patient CompanyMohammad Ali ImranNo ratings yet
- Periodesasi Judo Herlina GitaDocument6 pagesPeriodesasi Judo Herlina GitaAhmad Al'FredoNo ratings yet
- Madya Visha & MadatyayaDocument33 pagesMadya Visha & Madatyayaraghabendrasahu1998No ratings yet
- Endovive: Enteral Access DevicesDocument16 pagesEndovive: Enteral Access Devicesmarcilene vitorianoNo ratings yet
- Job Application FormDocument3 pagesJob Application Formnrynaybae.iiNo ratings yet
- Menpinmw NCPDocument1 pageMenpinmw NCPLevin MenpinNo ratings yet