You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5814)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1092)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (845)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (590)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (897)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (540)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (348)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (822)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (401)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- Anatomical Study of Jiu Jitsu Joint LocksDocument111 pagesAnatomical Study of Jiu Jitsu Joint LocksOuvertureFacile100% (6)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Anomaly Scan ReportDocument26 pagesAnomaly Scan ReportMichael Idowu100% (1)
- Neurology, Thalassemia & Endocrine Examination AllamDocument91 pagesNeurology, Thalassemia & Endocrine Examination AllamHigh Class Education (H.C.Education)No ratings yet
- Icd 10 UgdDocument6 pagesIcd 10 UgdTiara WidyastutiNo ratings yet
- 2.bones of Trunk & LimbsDocument19 pages2.bones of Trunk & LimbsRioNo ratings yet
- CHAPTER 57 Anatomy and Surgical Access of The MediastinumDocument6 pagesCHAPTER 57 Anatomy and Surgical Access of The MediastinumAbeNo ratings yet
- Manual Handling Learner GuideDocument16 pagesManual Handling Learner Guidebmwm31996bmwNo ratings yet
- Nucleus Arthroplasty Volume IIDocument55 pagesNucleus Arthroplasty Volume IIHelifunoNo ratings yet
- 504 Essential WordsDocument42 pages504 Essential WordsMatt Drew100% (13)
- CBD Spinal Infection: by Neoh Zhong NingDocument26 pagesCBD Spinal Infection: by Neoh Zhong NingJoni NeohNo ratings yet
- Cervical Spine DisorderDocument9 pagesCervical Spine DisorderANDRE MANo ratings yet
- Anatomy - Vertebral ColumnDocument5 pagesAnatomy - Vertebral ColumnArmelda Elda MuhollariNo ratings yet
- Herniated Nucleus Pulposus (Report) - 2Document27 pagesHerniated Nucleus Pulposus (Report) - 2Angelu Gabrielle CastroNo ratings yet
- Human Anatomy & Physiology: Spinal Cord, Spinal Nerves and Somatic ReflexesDocument41 pagesHuman Anatomy & Physiology: Spinal Cord, Spinal Nerves and Somatic ReflexesSyarif MaulanaNo ratings yet
- Lab Assignment Week # 2Document28 pagesLab Assignment Week # 2azizzatiNo ratings yet
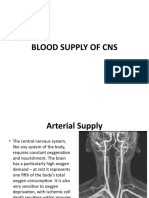
- NEUROANATOMY Lecture # 07 (BLOOD SUPPLY OF CNS)Document26 pagesNEUROANATOMY Lecture # 07 (BLOOD SUPPLY OF CNS)MISS. COMNo ratings yet
- Lesson Five 4 - 5837179529600176303Document9 pagesLesson Five 4 - 5837179529600176303julien KoudouNo ratings yet
- Structure and Function of The Musculoskeletal SystemDocument31 pagesStructure and Function of The Musculoskeletal SystemSaminathan KayarohanamNo ratings yet
- CSEC - Form 4 Human and Social Biology NotesDocument4 pagesCSEC - Form 4 Human and Social Biology NotesLeon Abel80% (5)
- Grade 4 Book My Science Health and Physical EducationDocument161 pagesGrade 4 Book My Science Health and Physical Educationmani_regmi3054No ratings yet
- Animals Science .Document24 pagesAnimals Science .Alkhair SangcopanNo ratings yet
- Healing Yoga For Neck and Shoulder PainDocument110 pagesHealing Yoga For Neck and Shoulder Painjamalaasr94% (17)
- Anatomy WordDocument86 pagesAnatomy WordYana-Marisa EdwardsNo ratings yet
- Herniated DiscsDocument28 pagesHerniated DiscsEndah A. Rahmadhani SugiartoNo ratings yet
- Introduction To General Pathology VPM 152: Web ReviewDocument41 pagesIntroduction To General Pathology VPM 152: Web ReviewRenien Khim BahayaNo ratings yet
- Chapter 5 The Skeletal SystemDocument139 pagesChapter 5 The Skeletal SystemCharlz ZipaganNo ratings yet
- How To Diagnose LBP RevisiDocument65 pagesHow To Diagnose LBP RevisiDedy SavradinataNo ratings yet
- Basic Clinical Manipulation PDFDocument227 pagesBasic Clinical Manipulation PDFMorosan Budau Olga100% (16)
- Scheme of Work Science Stage 4Document38 pagesScheme of Work Science Stage 4nesrineayad93No ratings yet