You might also like
- Images For Surgeons: Abdominal Tuberculosis: An Easily Forgotten DiagnosisDocument2 pagesImages For Surgeons: Abdominal Tuberculosis: An Easily Forgotten DiagnosisRisti Khafidah100% (1)
- Teaching Case of The Month: Abdominal Tuberculosis: An Unusual Cause of Abdominal PainDocument4 pagesTeaching Case of The Month: Abdominal Tuberculosis: An Unusual Cause of Abdominal PainkingkinresmytaNo ratings yet
- Abdominal Tuberculosis Presenting As Ascites in An Older Indigenous Woman: A Case ReportDocument5 pagesAbdominal Tuberculosis Presenting As Ascites in An Older Indigenous Woman: A Case ReportauliaNo ratings yet
- CASE REPORT Colitis TuberculosisDocument3 pagesCASE REPORT Colitis TuberculosisIfan RizkyNo ratings yet
- Clinical Predictors of Ileocecal Tuberculosis: A Case SeriesDocument14 pagesClinical Predictors of Ileocecal Tuberculosis: A Case SeriesChristopher AsisNo ratings yet
- Intestinal Tuberculosis: A Diagnostic Challenge: Open Access Case DOI: 10.7759/cureus.13058Document4 pagesIntestinal Tuberculosis: A Diagnostic Challenge: Open Access Case DOI: 10.7759/cureus.13058ATIKA INDAH SARINo ratings yet
- IJRP 100931120222804 (1) - CompressedDocument7 pagesIJRP 100931120222804 (1) - CompressedKlinik Bpjs AthariNo ratings yet
- Case Report: TB Peritonitis Mistaken For Ovarian Carcinomatosis Based On An Elevated CA-125Document4 pagesCase Report: TB Peritonitis Mistaken For Ovarian Carcinomatosis Based On An Elevated CA-125pudjoNo ratings yet
- Peritoneal Tuberculosis: ReviewDocument5 pagesPeritoneal Tuberculosis: ReviewEvellyna MeilanyNo ratings yet
- Unusual Case of Tuberculous Pleural Effusion and Abdominal MassDocument4 pagesUnusual Case of Tuberculous Pleural Effusion and Abdominal MassRofi IrmanNo ratings yet
- Abdominal Tuberculosis in Nepal Medical College Teaching Hospital, KathmanduDocument4 pagesAbdominal Tuberculosis in Nepal Medical College Teaching Hospital, KathmanduSavitri Maharani BudimanNo ratings yet
- 1-S2.0-S1726490112000895-Main Baru - En.idDocument5 pages1-S2.0-S1726490112000895-Main Baru - En.idHenandwita Fadilla PravitasariNo ratings yet
- Case Report: Streptococcus AnginosusDocument4 pagesCase Report: Streptococcus AnginosusIesanu MaraNo ratings yet
- Case Report Peritonitis WordDocument4 pagesCase Report Peritonitis WordMufidatul UmmahNo ratings yet
- Endoscopia: Diagnostic Approach of Intestinal Tuberculosis: Case and Literature ReviewDocument4 pagesEndoscopia: Diagnostic Approach of Intestinal Tuberculosis: Case and Literature ReviewDumitru RadulescuNo ratings yet
- Residents' Clinic: 22-Year-Old Man With Abdominal Pain and RashDocument4 pagesResidents' Clinic: 22-Year-Old Man With Abdominal Pain and RashAkhtar AliNo ratings yet
- JGH 13174Document9 pagesJGH 13174samudraandiNo ratings yet
- Clinical, Imaging, and Endoscopic Profile of Patients With Abdominal TuberculosisDocument6 pagesClinical, Imaging, and Endoscopic Profile of Patients With Abdominal TuberculosisINDRINo ratings yet
- A Girl With Ulcerative Colitis in A Tertiary Care Hospital-A Case ReportDocument4 pagesA Girl With Ulcerative Colitis in A Tertiary Care Hospital-A Case ReportAbdullah KhanNo ratings yet
- A Girl With Ulcerative Colitis in A Tertiary Care Hospital-A Case ReportDocument4 pagesA Girl With Ulcerative Colitis in A Tertiary Care Hospital-A Case ReportWyn AgustinNo ratings yet
- MRSAcolitisGastroenterol Report2015Document4 pagesMRSAcolitisGastroenterol Report2015selandia nisrinaNo ratings yet
- Systematic Review: Tuberculous Peritonitis - Presenting Features, Diagnostic Strategies and TreatmentDocument16 pagesSystematic Review: Tuberculous Peritonitis - Presenting Features, Diagnostic Strategies and TreatmenthendraNo ratings yet
- Peritoneal Tuberculosis: A Review of Diagnosis and ManagementDocument5 pagesPeritoneal Tuberculosis: A Review of Diagnosis and ManagementHanny FadhilaNo ratings yet
- Hiding in The Water: Clinical Problem-SolvingDocument6 pagesHiding in The Water: Clinical Problem-SolvingtabareeNo ratings yet
- Abdominal Tuberculosis Diagnosis and TreatmentDocument4 pagesAbdominal Tuberculosis Diagnosis and TreatmentYousra AhmedNo ratings yet
- doi- 10.1111:j.1525-1438.2006.00209.x.Document6 pagesdoi- 10.1111:j.1525-1438.2006.00209.x.Sulaeman Andrianto SusiloNo ratings yet
- J500200164 - Hajarina Qahirah ADocument13 pagesJ500200164 - Hajarina Qahirah A164Hajarina Qahirah A -No ratings yet
- Hematochezia Case Report on Crohn's Disease in Young MaleDocument3 pagesHematochezia Case Report on Crohn's Disease in Young Maleseptian_tjayaNo ratings yet
- Jurnal TB AbdomenDocument4 pagesJurnal TB AbdomenbelaNo ratings yet
- 260-Article Text-875-1-10-20220728Document4 pages260-Article Text-875-1-10-20220728hasan andrianNo ratings yet
- Fast Facts: Complex Perianal Fistulas in Crohn's Disease: A multidisciplinary approach to a clinical challengeFrom EverandFast Facts: Complex Perianal Fistulas in Crohn's Disease: A multidisciplinary approach to a clinical challengeNo ratings yet
- Purbadi-Peritoneal tuberculosis mimicking advanced ovarian cancer case report- Laparoscopy as diagnostic modality-2021-International Journal of Surgery Case ReportsDocument4 pagesPurbadi-Peritoneal tuberculosis mimicking advanced ovarian cancer case report- Laparoscopy as diagnostic modality-2021-International Journal of Surgery Case ReportsSulaeman Andrianto SusiloNo ratings yet
- Drug Induced Hepatitis Pada Tuberkulosis Paru Dengan MultisiteDocument6 pagesDrug Induced Hepatitis Pada Tuberkulosis Paru Dengan MultisiteAyuNo ratings yet
- 16 3 2010 0350 0351 PDFDocument2 pages16 3 2010 0350 0351 PDFSandi ApriadiNo ratings yet
- Tuberculosis and Chronic Renal FailureDocument38 pagesTuberculosis and Chronic Renal FailureGopal ChawlaNo ratings yet
- Pancreatic Tuberculosis Diagnosis UpdateDocument24 pagesPancreatic Tuberculosis Diagnosis UpdatesamudraandiNo ratings yet
- Gi 2Document2 pagesGi 2Syifa' FauziyahNo ratings yet
- Primary Splenic Amyloidosis: A Case ReportDocument4 pagesPrimary Splenic Amyloidosis: A Case Reportfitra khoNo ratings yet
- Liver Disease: A Clinical CasebookFrom EverandLiver Disease: A Clinical CasebookStanley Martin CohenNo ratings yet
- Tuberculous Salpingitis: A Case Report: - 2013 Jun 7 (6) : 1186-1188. Published Online 2013 Jun 1. Doi: PMCID: PMC3708232Document5 pagesTuberculous Salpingitis: A Case Report: - 2013 Jun 7 (6) : 1186-1188. Published Online 2013 Jun 1. Doi: PMCID: PMC3708232Lucky PuspitasariNo ratings yet
- Pylephlebitis Incidentally Found On A Patient With Gastric CancerDocument3 pagesPylephlebitis Incidentally Found On A Patient With Gastric CancerTony NouhNo ratings yet
- International Journal of Surgery Case Reports: Adenocarcinoma in An Ano-Vaginal Fistula in Crohn's DiseaseDocument4 pagesInternational Journal of Surgery Case Reports: Adenocarcinoma in An Ano-Vaginal Fistula in Crohn's DiseaseTegoeh RizkiNo ratings yet
- Mediastinal Mass in A 25-Year-Old Man: Chest Imaging and Pathology For CliniciansDocument5 pagesMediastinal Mass in A 25-Year-Old Man: Chest Imaging and Pathology For CliniciansWahyu RianiNo ratings yet
- Ajol File Journals - 76 - Articles - 114038 - Submission - Proof - 114038 901 318286 1 10 20150309Document2 pagesAjol File Journals - 76 - Articles - 114038 - Submission - Proof - 114038 901 318286 1 10 20150309alysNo ratings yet
- Artigo 29Document5 pagesArtigo 29raudneimNo ratings yet
- Delay in Diagnosis of Extra-Pulmonary Tuberculosis by Its Rare Manifestations: A Case ReportDocument5 pagesDelay in Diagnosis of Extra-Pulmonary Tuberculosis by Its Rare Manifestations: A Case ReportSneeze LouderNo ratings yet
- Potts DiseaseDocument6 pagesPotts DiseaseJefferson ManasanNo ratings yet
- Management of Occult GI Bleeding: A Clinical GuideFrom EverandManagement of Occult GI Bleeding: A Clinical GuideMicheal TadrosNo ratings yet
- Case Report and Literature Review On Good's Syndrome, A Form of Acquired Immunodeficiency Associated With ThymomasDocument7 pagesCase Report and Literature Review On Good's Syndrome, A Form of Acquired Immunodeficiency Associated With ThymomasMudassar SattarNo ratings yet
- Severe Peritonitis Case Report Highlights Diagnosis and Treatment of Acute PancreatitisDocument2 pagesSevere Peritonitis Case Report Highlights Diagnosis and Treatment of Acute PancreatitisJune Faith HacheroNo ratings yet
- Acute Gastrointestinal Bleeding: Diagnosis and TreatmentFrom EverandAcute Gastrointestinal Bleeding: Diagnosis and TreatmentKaren E. KimNo ratings yet
- Case 167: MD Pediatrics PHD Ped Study Children Special NeedDocument49 pagesCase 167: MD Pediatrics PHD Ped Study Children Special NeedMona MostafaNo ratings yet
- Diseases of the Liver and Biliary TreeFrom EverandDiseases of the Liver and Biliary TreeAnnarosa FloreaniNo ratings yet
- Tuberculous Ileal Perforation in Post-Appendicectomy PeriOperative Period: A Diagnostic ChallengeDocument3 pagesTuberculous Ileal Perforation in Post-Appendicectomy PeriOperative Period: A Diagnostic ChallengeIOSRjournalNo ratings yet
- Case Report Hepato FinalDocument29 pagesCase Report Hepato FinalBangkit PutrawanNo ratings yet
- Toxic Megacolon Presentation FinalDocument33 pagesToxic Megacolon Presentation FinalHendra SetyawanNo ratings yet
- Hemochromatosis and HCCDocument4 pagesHemochromatosis and HCCMihaela MocanNo ratings yet
- emerg-3-168Document2 pagesemerg-3-168Randy SaputraNo ratings yet
- 1 s2.0 S2210261221009731 MainDocument4 pages1 s2.0 S2210261221009731 Maintarmohamed.muradNo ratings yet
- FAMILY PLANNING PERSONAL NOTESDocument4 pagesFAMILY PLANNING PERSONAL NOTESOB-GYNE DEPARTMENTNo ratings yet
- Scientific Review ProcessDocument16 pagesScientific Review ProcessOB-GYNE DEPARTMENTNo ratings yet
- MARCH 12 copyDocument7 pagesMARCH 12 copyOB-GYNE DEPARTMENTNo ratings yet
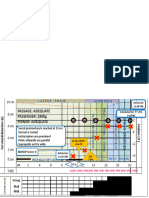
- PAETOGRAPH CS AUDITDocument2 pagesPAETOGRAPH CS AUDITOB-GYNE DEPARTMENTNo ratings yet
- NSD + PSDocument1 pageNSD + PSOB-GYNE DEPARTMENTNo ratings yet
- Hypogastric Pain Leads to Diagnosis of Potts DiseaseDocument11 pagesHypogastric Pain Leads to Diagnosis of Potts DiseaseOB-GYNE DEPARTMENTNo ratings yet
- Delivery RecordDocument2 pagesDelivery RecordOB-GYNE DEPARTMENTNo ratings yet
- Manual Extraction of The PlacentaDocument1 pageManual Extraction of The PlacentaOB-GYNE DEPARTMENTNo ratings yet
- Classical CS FinalDocument1 pageClassical CS FinalOB-GYNE DEPARTMENTNo ratings yet
- Umbilical Cord CareDocument3 pagesUmbilical Cord CareHui Li TehNo ratings yet
- Kingdom MycotaDocument33 pagesKingdom MycotaSariska MehraNo ratings yet
- Bennett2007 PDFDocument8 pagesBennett2007 PDFMirza RisqaNo ratings yet
- 210-241 UrinaryDocument34 pages210-241 UrinaryYaj Cruzada100% (1)
- Significance of Study-Denguesummer2012Document2 pagesSignificance of Study-Denguesummer2012Mark Remuel Cruz FinezNo ratings yet
- Clinical Manifestations and Diagnosis of Vitamin B12 and Folate Deficiency - UpToDateDocument63 pagesClinical Manifestations and Diagnosis of Vitamin B12 and Folate Deficiency - UpToDateHuỳnh Thị Khả DuyNo ratings yet
- Why SufferingDocument7 pagesWhy SufferingRandall Dean WestNo ratings yet
- Workshop1 1Document2 pagesWorkshop1 1Aple Mae Cudiamat Letranca-CastroNo ratings yet
- Dsm-Iii at The Cinema: Madness in The MoviesDocument12 pagesDsm-Iii at The Cinema: Madness in The MoviesLiridon1804No ratings yet
- Xi Cleft (Accumulation Point) : DiagnosisDocument4 pagesXi Cleft (Accumulation Point) : DiagnosisZareen FNo ratings yet
- The Diagnostic Criteria For Chronic EndometritisDocument7 pagesThe Diagnostic Criteria For Chronic EndometritisyuriescaidaNo ratings yet
- Diabetic Living - Summer 2016Document108 pagesDiabetic Living - Summer 2016Lohrasp Suraliwala100% (2)
- Neurorehabilitation in Neuro-Oncology 2019 E-BookDocument254 pagesNeurorehabilitation in Neuro-Oncology 2019 E-BookWoffe SoloNo ratings yet
- Train Your Brain Build A Framework For Clear ThinkingDocument235 pagesTrain Your Brain Build A Framework For Clear ThinkingyashyiNo ratings yet
- Psychological Trauma: Theory, Research, Practice, and PolicyDocument4 pagesPsychological Trauma: Theory, Research, Practice, and PolicyPerla MontellanoNo ratings yet
- Manaka TechniqueDocument5 pagesManaka TechniqueKoa Carlos CastroNo ratings yet
- 2ND Periodical Test in Science 6 With Tos KeyDocument9 pages2ND Periodical Test in Science 6 With Tos KeyJumaliza Francisco Paguirigan67% (3)
- Cambridge International AS & A Level: BIOLOGY 9700/21Document20 pagesCambridge International AS & A Level: BIOLOGY 9700/21jamalNo ratings yet
- Manual Breast Manual ExpressionDocument9 pagesManual Breast Manual ExpressionhoneykrizelNo ratings yet
- Legg Calve Perthes DiseaseDocument7 pagesLegg Calve Perthes DiseaseMatthew Rich Laguitao CortesNo ratings yet
- Frcophth 400 Sbas and CrqsDocument262 pagesFrcophth 400 Sbas and CrqsZaheer Ullah Soleh100% (1)
- Probiotics and Preterm Infants A Position Paper.26 ShareDocument17 pagesProbiotics and Preterm Infants A Position Paper.26 Shareendy tovarNo ratings yet
- Pharmacy Guidelines and Instructions For DAIDS Clinical Trials Networks March 2016Document41 pagesPharmacy Guidelines and Instructions For DAIDS Clinical Trials Networks March 2016GerifalteNo ratings yet
- BSN 1-1 Biochem Week 6Document2 pagesBSN 1-1 Biochem Week 6PAULINE KAYE QUITANNo ratings yet
- Ts 410 420 Product Instruction ManualDocument112 pagesTs 410 420 Product Instruction ManualRosario GonzalesNo ratings yet
- Asimetrii MandibulareDocument25 pagesAsimetrii MandibulareBranici OanaNo ratings yet
- Red Flags ArticleDocument4 pagesRed Flags ArticleINNOCENT KHULIWANo ratings yet
- 2020 Eagle Practical CardiologyDocument24 pages2020 Eagle Practical CardiologyaeliasgvNo ratings yet
- Single-Cell Map of Diverse Immune Phenotypes in The Breast Tumor MicroenvironmentDocument53 pagesSingle-Cell Map of Diverse Immune Phenotypes in The Breast Tumor MicroenvironmentRoger FigueiredoNo ratings yet
- Diapositivas Amoxicilina English Cipas 2Document7 pagesDiapositivas Amoxicilina English Cipas 2viviana1417No ratings yet