You might also like
- Filipino Construction Terms in ArchitectureDocument2 pagesFilipino Construction Terms in ArchitectureMarj Oblinada100% (3)
- Pharmaceutical Quality ManagementDocument4 pagesPharmaceutical Quality ManagementlindaNo ratings yet
- GMP in Pharmaceutical Industry: Global cGMP & Regulatory ExpectationsFrom EverandGMP in Pharmaceutical Industry: Global cGMP & Regulatory ExpectationsRating: 5 out of 5 stars5/5 (2)
- EXP Well Intervention 20p A4 ProofDocument20 pagesEXP Well Intervention 20p A4 ProofMohamed Kamal100% (2)
- Pharmaceutical Quality Management System (QMS) Questions and AnswersFrom EverandPharmaceutical Quality Management System (QMS) Questions and AnswersNo ratings yet
- GMP ManualDocument303 pagesGMP ManualShrinivas TamaskarNo ratings yet
- CDER's Quality Management Maturity Program: Fda/Cder/Opq/OqsDocument26 pagesCDER's Quality Management Maturity Program: Fda/Cder/Opq/OqsAmbadas RautNo ratings yet
- FDA's New Rating SystemDocument7 pagesFDA's New Rating SystemmuratNo ratings yet
- GMPDocument3 pagesGMPdamien.zoni.travailNo ratings yet
- Pharmaceutical Quality Management SystemDocument13 pagesPharmaceutical Quality Management SystemShailesh Gupta100% (1)
- Change Management: Common Failures and A Checklist For ImprovementDocument5 pagesChange Management: Common Failures and A Checklist For ImprovementPerry BurtonNo ratings yet
- The Pharmaceutical Guide To The Perfect Quality Assurance PlanDocument17 pagesThe Pharmaceutical Guide To The Perfect Quality Assurance PlansamontoyaNo ratings yet
- Assignment of QCMDocument14 pagesAssignment of QCMAnoosha FarooquiNo ratings yet
- A PDFDocument13 pagesA PDFMunir ShmaitNo ratings yet
- Presentation GMP and CGMP ConsiderationsDocument42 pagesPresentation GMP and CGMP ConsiderationsMimi SlifiNo ratings yet
- State of Total Quality Management in Pharmaceutical Industry Literature ReviewDocument4 pagesState of Total Quality Management in Pharmaceutical Industry Literature ReviewwoeatlrifNo ratings yet
- QBT To QBDDocument7 pagesQBT To QBDshelfinararaNo ratings yet
- Process ValidationDocument5 pagesProcess ValidationNarongchai PongpanNo ratings yet
- Benchmarking The Quality Practices of Global Pharmaceutical Manufacturing To Advance Supply Chain ResilienceDocument11 pagesBenchmarking The Quality Practices of Global Pharmaceutical Manufacturing To Advance Supply Chain Resilienceoanateodorachirac1995No ratings yet
- Quality by Desig1Document10 pagesQuality by Desig1Asti Destilia SafrudinNo ratings yet
- Process ValidationDocument30 pagesProcess ValidationIrfan A. Ahanger100% (2)
- Aksu 2019 Chapter 2Document23 pagesAksu 2019 Chapter 2Angel GarciaNo ratings yet
- Elemnts QBDDocument9 pagesElemnts QBDalexNo ratings yet
- Quality by Design (QBD) : A New Concept For Development of Quality PharmaceuticalsDocument7 pagesQuality by Design (QBD) : A New Concept For Development of Quality PharmaceuticalsVitalis MbuyaNo ratings yet
- From QBT To QBD 1Document3 pagesFrom QBT To QBD 1JuspidayantiNo ratings yet
- Usfda CGMP PDFDocument49 pagesUsfda CGMP PDFHARI HARA RAO GUJJARNo ratings yet
- Process Analytical Technology: A ReviewDocument23 pagesProcess Analytical Technology: A ReviewAbbas Syed100% (2)
- Implementation of QBD AQbD Approach in Pharmaceutical Formulation and Analytical Method Development A Comprehensive Research Review Ijariie18342 PDFDocument32 pagesImplementation of QBD AQbD Approach in Pharmaceutical Formulation and Analytical Method Development A Comprehensive Research Review Ijariie18342 PDFrbmoureNo ratings yet
- Contamination - Control - in - and - Out - of - The - Cleanroom - Full - ArticleDocument3 pagesContamination - Control - in - and - Out - of - The - Cleanroom - Full - ArticlesigalrusNo ratings yet
- GXP Compliance in Pharmaceutical Industry PDFDocument6 pagesGXP Compliance in Pharmaceutical Industry PDFGyana SahooNo ratings yet
- Quality by Design Approaches For Topical Dermatological Dosage FormsDocument19 pagesQuality by Design Approaches For Topical Dermatological Dosage FormsDoinița UrsuNo ratings yet
- QMS in Medical Device ProjectsDocument3 pagesQMS in Medical Device Projectsjicet67288No ratings yet
- Why Are Cgmps So Important?Document13 pagesWhy Are Cgmps So Important?Adeliza MortallaNo ratings yet
- QMS For APIs Integrating Iso 9001 2005Document73 pagesQMS For APIs Integrating Iso 9001 2005kartpgit1987No ratings yet
- QD FabDocument3 pagesQD Fabfabianosir321No ratings yet
- Weekly Current Affairs 8-Jan-2024 To 14-Jan-2024Document25 pagesWeekly Current Affairs 8-Jan-2024 To 14-Jan-2024Vandana VermaNo ratings yet
- Jun 2017 CPD QMSDocument49 pagesJun 2017 CPD QMSSelvaraj SimiyonNo ratings yet
- Avoiding Errors With The Batch Release ProcessDocument11 pagesAvoiding Errors With The Batch Release ProcessAnthony CollierNo ratings yet
- 56-63, Tesma0807, IJEASTDocument8 pages56-63, Tesma0807, IJEASTlahrach.yasmine1No ratings yet
- Understanding Pharmaceutical QBD PDFDocument13 pagesUnderstanding Pharmaceutical QBD PDFcabeto124211No ratings yet
- A Quantitative Approach For PharmaceuticDocument8 pagesA Quantitative Approach For PharmaceuticHalil İbrahim ÖzdemirNo ratings yet
- Good Manufacturing Practices (GMP)Document5 pagesGood Manufacturing Practices (GMP)sai vaibhavNo ratings yet
- Quality by Design (QBD) A Comprehensive Understanding of ImplementationDocument7 pagesQuality by Design (QBD) A Comprehensive Understanding of Implementationiabureid7460No ratings yet
- Quality by Design (QBD) - Principles Underlying Concepts and RegDocument17 pagesQuality by Design (QBD) - Principles Underlying Concepts and RegVinay PatelNo ratings yet
- Quality by Design: Review ArticleDocument13 pagesQuality by Design: Review ArticleIjupbs IjupbsNo ratings yet
- Journal of Drug Discovery and Therapeutics 1 (6) 2013, 47-55Document9 pagesJournal of Drug Discovery and Therapeutics 1 (6) 2013, 47-55k.p.No ratings yet
- Total Quality Management in Pharmaceuticals PDFDocument11 pagesTotal Quality Management in Pharmaceuticals PDFNarongchai PongpanNo ratings yet
- Moving From Quality Control To Quality AssuranceDocument5 pagesMoving From Quality Control To Quality AssuranceMohamed ZhranNo ratings yet
- GMPANDc GMPCONSIDERATIONSDocument42 pagesGMPANDc GMPCONSIDERATIONSbalrajjadonNo ratings yet
- Good Manufacturing Practice in The Pharmaceutical Industry: Done By: Ali Mahmoud Jasim Supervised: Prof. Talal A. AburjaiDocument46 pagesGood Manufacturing Practice in The Pharmaceutical Industry: Done By: Ali Mahmoud Jasim Supervised: Prof. Talal A. AburjaitesteNo ratings yet
- IVT SDCC pgs6Document42 pagesIVT SDCC pgs6sabrinaNo ratings yet
- UNIMMA-Rendhika Krisna WibowoDocument1 pageUNIMMA-Rendhika Krisna WibowoRendhikaNo ratings yet
- Asps 03 0376Document5 pagesAsps 03 0376surafelNo ratings yet
- The Self-Inspections (Internal Audits) Process As A Part of The Pharmaceutical Quality System: Formation of A Risk-Based Approach To Internal Audits PlanningDocument13 pagesThe Self-Inspections (Internal Audits) Process As A Part of The Pharmaceutical Quality System: Formation of A Risk-Based Approach To Internal Audits PlanningSabrina JonesNo ratings yet
- Future-Proofing Pharmaceutical Analytical Method Development With An AQbD ApproachDocument6 pagesFuture-Proofing Pharmaceutical Analytical Method Development With An AQbD ApproachrbmoureNo ratings yet
- The FDA and Worldwide Current Good Manufacturing Practices and Quality System Requirements Guidebook for Finished PharmaceuticalsFrom EverandThe FDA and Worldwide Current Good Manufacturing Practices and Quality System Requirements Guidebook for Finished PharmaceuticalsNo ratings yet
- ECA Modern EU and FDA ValidationDocument4 pagesECA Modern EU and FDA ValidationAziz Aditya WigunaNo ratings yet
- GMP and Regulations: Good Manufacturing PracticeDocument10 pagesGMP and Regulations: Good Manufacturing PracticeCelia Caroline Neves Faria de SousaNo ratings yet
- Quality by Design (QBD) Approach in Pharmaceuticals: Status, Challenges and Next StepsDocument8 pagesQuality by Design (QBD) Approach in Pharmaceuticals: Status, Challenges and Next StepsnabilahNo ratings yet
- Pharmaceutics 13 00919 v2Document45 pagesPharmaceutics 13 00919 v24n4n4sNo ratings yet
- Development Knowledge QBDDocument6 pagesDevelopment Knowledge QBDNarendrakumarNo ratings yet
- Grammar Quiz: Whatever / Whenever / WhoeverDocument2 pagesGrammar Quiz: Whatever / Whenever / WhoeverGrover Quispe MamaniNo ratings yet
- EF's Booking Conditions: What's Included On Your TourDocument6 pagesEF's Booking Conditions: What's Included On Your Tournmoultrie200No ratings yet
- Financial Times Magazine - April 2017Document45 pagesFinancial Times Magazine - April 2017jwestmisterNo ratings yet
- Dirichlet PrincipleDocument30 pagesDirichlet PrincipleNguyễn Ngân HàNo ratings yet
- Learning DefinitionDocument2 pagesLearning DefinitionRaden Nurilma HidayatullahNo ratings yet
- Daily English Lesson Plan For Year 5 (20 September 2011)Document2 pagesDaily English Lesson Plan For Year 5 (20 September 2011)V Rozanna Matthew0% (1)
- A Conceptual Framework On Implementing Additive ManufacturingDocument15 pagesA Conceptual Framework On Implementing Additive ManufacturingAnonymous 5AmJ13mLkNo ratings yet
- A Holdsworth Guitar AstronaDocument4 pagesA Holdsworth Guitar Astronaprimus290% (10)
- Attention Important Information: Vehicles For The Visteon Satellite Kits 4068597 (Generic) & 4068598 (MUX/DVD)Document73 pagesAttention Important Information: Vehicles For The Visteon Satellite Kits 4068597 (Generic) & 4068598 (MUX/DVD)Fermin AbadíaNo ratings yet
- Faculty Member, Himachal Institute of Life Sciences: Ashok KumarDocument12 pagesFaculty Member, Himachal Institute of Life Sciences: Ashok KumarasokumrNo ratings yet
- Cover LetterDocument2 pagesCover LetterBilal AslamNo ratings yet
- Edited Final MekdiDocument61 pagesEdited Final MekdiBetelhiem WoldemedhinNo ratings yet
- DNA Repair - On The Pathways To Fixing DNA Damage and ErrorsDocument392 pagesDNA Repair - On The Pathways To Fixing DNA Damage and ErrorsStefan ŽivanovićNo ratings yet
- P.E Sba Kalayma GrittenDocument21 pagesP.E Sba Kalayma Grittenselina fraser100% (2)
- Limiting Factors On Population DensityDocument2 pagesLimiting Factors On Population DensityLaarni Faye Sarmiento100% (1)
- SBD-E-Commerce and Internet MarketingDocument12 pagesSBD-E-Commerce and Internet MarketingjacvillarbaNo ratings yet
- Prefix Suffix Root List ChartDocument6 pagesPrefix Suffix Root List Chartangelajohnson1983No ratings yet
- Al Ghubaiba Bus Station - Abu Dhabi, Central Bus Station Õ ÕÛ C R'@C @ (Ê Óå Ï - Õ C R'? @ (Document4 pagesAl Ghubaiba Bus Station - Abu Dhabi, Central Bus Station Õ ÕÛ C R'@C @ (Ê Óå Ï - Õ C R'? @ (Dubai Q&ANo ratings yet
- Pittsfield Public Schools New Code of Conduct, Character and SupportDocument65 pagesPittsfield Public Schools New Code of Conduct, Character and SupportThe Berkshire EagleNo ratings yet
- Assignment 1 OsDocument3 pagesAssignment 1 OsAbdul Wajid HanjrahNo ratings yet
- Blue Jay Private LimitedDocument2 pagesBlue Jay Private LimitedanuNo ratings yet
- 2004 Electrical Schematics: P42/L57 ChassisDocument52 pages2004 Electrical Schematics: P42/L57 ChassisMTK2016No ratings yet
- Cover Page For ESP 9Document6 pagesCover Page For ESP 9Ghost hackerNo ratings yet
- Case GrammarDocument5 pagesCase GrammarBel SterlingNo ratings yet
- Olfactory Receptors Are Not Unique To The NoseDocument1 pageOlfactory Receptors Are Not Unique To The NoseMicheleFontanaNo ratings yet
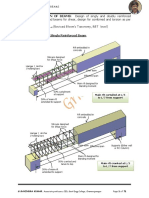
- Beams, Design of Flanged Beams For Shear, Design For Combined and Torsion As Per IS - 456. 10 Hours L and L (Revised Bloom's Taxonomy, RBT Level)Document71 pagesBeams, Design of Flanged Beams For Shear, Design For Combined and Torsion As Per IS - 456. 10 Hours L and L (Revised Bloom's Taxonomy, RBT Level)Viji NpNo ratings yet
- Present Simple and Continuous Question Time PDFDocument2 pagesPresent Simple and Continuous Question Time PDFКаріна ЗейканNo ratings yet
- Manunggul-Cave EditedDocument14 pagesManunggul-Cave EditedCoco MartinNo ratings yet