You might also like
- CCRN Cert Review Neuro 2Document15 pagesCCRN Cert Review Neuro 2Giovanni MictilNo ratings yet
- Catapres (Clonidine)Document2 pagesCatapres (Clonidine)Adrianne BazoNo ratings yet
- Management of Lumbar Spinal Stenosis 2016Document13 pagesManagement of Lumbar Spinal Stenosis 2016Bruno HazlebyNo ratings yet
- Thoracic and Lumbar Pain and Stiffness - M. Suresh SchlangerDocument26 pagesThoracic and Lumbar Pain and Stiffness - M. Suresh Schlangerscason9No ratings yet
- AOSpine Masters Series Vol 8 Back Pain by Vialle, Luiz Roberto GomesDocument362 pagesAOSpine Masters Series Vol 8 Back Pain by Vialle, Luiz Roberto GomesCésar MierNo ratings yet
- Massage Therapy For Bruxism, TMJ SyndromeDocument39 pagesMassage Therapy For Bruxism, TMJ SyndromeAdam Kesher100% (1)
- Drug Study (Haloperidol)Document3 pagesDrug Study (Haloperidol)Mae Ann Bueno CastillonNo ratings yet
- Lumbar Strain: Dr. Lipy Bhat PT Faculty, Physiotherapy SrhuDocument38 pagesLumbar Strain: Dr. Lipy Bhat PT Faculty, Physiotherapy SrhuKapil LakhwaraNo ratings yet
- The Inner UnitDocument8 pagesThe Inner UnitAerialist Bhagavati100% (2)
- Antiviral Agents - 2022Document113 pagesAntiviral Agents - 2022Top VidsNo ratings yet
- Pulmonary EmbolismDocument27 pagesPulmonary EmbolismEfren Ezekiel AlbiosNo ratings yet
- Case Study AntenatalDocument19 pagesCase Study AntenatalRDi J100% (1)
- Isoflurane ThiopentalDocument13 pagesIsoflurane ThiopentalMr rawr100% (1)
- Medical Iyengar Yoga SequencesDocument141 pagesMedical Iyengar Yoga Sequencesscribewala100% (13)
- DRUG STUDY Exams Ms - LavarraDocument15 pagesDRUG STUDY Exams Ms - LavarraCharm Abyss la MorenaNo ratings yet
- CH 41 LBP - Braddom's Physical Medicine & RehabilitationDocument46 pagesCH 41 LBP - Braddom's Physical Medicine & RehabilitationPyrectic WilliamsNo ratings yet
- A Case Study On Parkinsons DiseaseDocument42 pagesA Case Study On Parkinsons DiseaseMark Tristan AsuncionNo ratings yet
- NimodipineDocument5 pagesNimodipineGwyn Rosales100% (1)
- Hipertensi-Krisis Dr. HendroDocument35 pagesHipertensi-Krisis Dr. Hendroyudhagp100% (1)
- Cyriax - Spine: by DR. Akshay A. Chougule (PT) Orthopaedic Manual TherapistDocument44 pagesCyriax - Spine: by DR. Akshay A. Chougule (PT) Orthopaedic Manual TherapistAishwarya Shah100% (1)
- Case Report Skizofrenia KatatonikDocument3 pagesCase Report Skizofrenia KatatonikIntan PratiwiNo ratings yet
- CL PsychDocument1 pageCL PsychasdfNo ratings yet
- Case Study ARF Fall 2020Document4 pagesCase Study ARF Fall 2020Hailey GiauqueNo ratings yet
- 33 Psych EmergenciesDocument3 pages33 Psych EmergenciesGAPL WijesekaraNo ratings yet
- DroperidolDocument1 pageDroperidolIvanne HisolerNo ratings yet
- Nursing Care Plan - Impaired DentitionDocument18 pagesNursing Care Plan - Impaired Dentitionken kiplimoNo ratings yet
- Citalopram ManiaDocument6 pagesCitalopram Maniagion.nandNo ratings yet
- Seizure Disorders: Abraham Berger, MD, F.A.C.E.P. Department of Emergency Medicine Beth Israel Medical Center, N.YDocument44 pagesSeizure Disorders: Abraham Berger, MD, F.A.C.E.P. Department of Emergency Medicine Beth Israel Medical Center, N.YTheop AyodeleNo ratings yet
- POC and Concepts Maps Week 12Document23 pagesPOC and Concepts Maps Week 12Michelle CollinsNo ratings yet
- Case StudyDocument14 pagesCase Studyapi-592376639No ratings yet
- Injections: 2.5mg/ml in CNS: Drowsiness,: DroperidolDocument3 pagesInjections: 2.5mg/ml in CNS: Drowsiness,: DroperidolthesarayoNo ratings yet
- (Per System Preferably) : AntihypertensiveDocument4 pages(Per System Preferably) : AntihypertensiveGwyn RosalesNo ratings yet
- PSYCHOTROPIC AGENTS - ActivityDocument13 pagesPSYCHOTROPIC AGENTS - ActivityANNA V. LARITANo ratings yet
- Drug StudyDocument4 pagesDrug StudyXio PauNo ratings yet
- Case StudyDocument19 pagesCase StudyChristine MccombsNo ratings yet
- Chief ComplaintDocument4 pagesChief ComplaintKram mrkNo ratings yet
- Grand Rounds SAHDocument32 pagesGrand Rounds SAHJohn Bryan GonzagaNo ratings yet
- Assignment - HypertensionDocument6 pagesAssignment - HypertensionAyessa Salazar100% (2)
- Kuliah Hipertensi KrisisDocument30 pagesKuliah Hipertensi KrisisArbusa86No ratings yet
- Case No. 6 Lost The PlotDocument7 pagesCase No. 6 Lost The PlotNermeen AlrajhiNo ratings yet
- Igd 13-1-2020Document25 pagesIgd 13-1-2020Jefri SusantoNo ratings yet
- Nms Topic DiscussionDocument2 pagesNms Topic Discussionapi-734449276No ratings yet
- NCP 2004Document6 pagesNCP 2004Kate WillisNo ratings yet
- Week 5 - Course TaskDocument7 pagesWeek 5 - Course TaskCher Allain BellosilloNo ratings yet
- Long Case 1Document16 pagesLong Case 1damion clarkeNo ratings yet
- Hipertensi Krisis: DR Widyastuti Puskesmas TanggulanginDocument29 pagesHipertensi Krisis: DR Widyastuti Puskesmas TanggulanginvitrieNo ratings yet
- Formatif NBSSDocument17 pagesFormatif NBSSCYNTHIA ARISTANo ratings yet
- MethyldopaDocument4 pagesMethyldopaMichael TokongNo ratings yet
- Neuroleptic Malignant Syndrome: Kathryn RosenblattDocument12 pagesNeuroleptic Malignant Syndrome: Kathryn RosenblattTroy FengNo ratings yet
- Convulsive Disorders: Presenters: Kabwe Chanda EliasDocument30 pagesConvulsive Disorders: Presenters: Kabwe Chanda EliasHomeground entertainmentNo ratings yet
- PSYCHIAdrugstudyDocument5 pagesPSYCHIAdrugstudyJss Rosete-De GuzmanNo ratings yet
- Hashim Daily Log 2Document10 pagesHashim Daily Log 2Hashim AlsammawiNo ratings yet
- Prevention and Management of Pain, AgitationDocument44 pagesPrevention and Management of Pain, AgitationSiriporn PongpattarapakNo ratings yet
- Anemia Concept Mapping. Group 1Document82 pagesAnemia Concept Mapping. Group 1Giselle EstoquiaNo ratings yet
- Pediatric Cardiology: Ruby Ann L. Punongbayan, MDDocument51 pagesPediatric Cardiology: Ruby Ann L. Punongbayan, MDsarguss14100% (3)
- Endocrinología Y Nutrición: Scientific LettersDocument2 pagesEndocrinología Y Nutrición: Scientific LettersMakmur SejatiNo ratings yet
- Ziprasidone Drug StudyDocument4 pagesZiprasidone Drug Studyshadow gonzalez100% (1)
- Multiple Episodes of NMS: Overlap With Malignant Catatonia: Case NotesDocument3 pagesMultiple Episodes of NMS: Overlap With Malignant Catatonia: Case NotesTurkey AlomraneyNo ratings yet
- The PatientDocument9 pagesThe PatientJan Crizza Dale R. FrancoNo ratings yet
- A Changed Alphabet and Neurological ChaosDocument31 pagesA Changed Alphabet and Neurological ChaosBisweswar OjhaNo ratings yet
- Toxicology PDFDocument44 pagesToxicology PDFhuong LNo ratings yet
- Slides-Dr Ahmed Mahmood Husain Azzaw OAB ManagementDocument17 pagesSlides-Dr Ahmed Mahmood Husain Azzaw OAB ManagementDylanSalamNo ratings yet
- Atypical Presentation of Neuroleptic Malignant Syndrome: A Diagnostic DilemmaDocument4 pagesAtypical Presentation of Neuroleptic Malignant Syndrome: A Diagnostic Dilemmagion.nandNo ratings yet
- Snake BiteDocument62 pagesSnake Bitelailatul husnaNo ratings yet
- Patient & Family EducationDocument3 pagesPatient & Family EducationJenjendeuk kimNo ratings yet
- NCM118 (Midterms) Activity 6: Case Analysis: Assessment Finding Physiologic Basis Nursing InterventionDocument2 pagesNCM118 (Midterms) Activity 6: Case Analysis: Assessment Finding Physiologic Basis Nursing InterventionKyla TuanNo ratings yet
- Reducing Med ErrorsDocument14 pagesReducing Med ErrorsTop VidsNo ratings yet
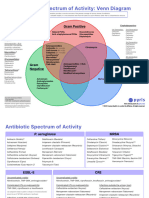
- Antibotics Venn DiagramDocument2 pagesAntibotics Venn DiagramTop VidsNo ratings yet
- Chapter 146: Antimicrobial Prophylaxis in Surgery SELF-ASSESSMENT QUESTIONSDocument3 pagesChapter 146: Antimicrobial Prophylaxis in Surgery SELF-ASSESSMENT QUESTIONSTop VidsNo ratings yet
- Chapter 139: Urinary Tract Infections Self-Assessment QuestionsDocument4 pagesChapter 139: Urinary Tract Infections Self-Assessment QuestionsTop VidsNo ratings yet
- Chapter 48 - Antifungal Agents - Preclass MaterialsDocument14 pagesChapter 48 - Antifungal Agents - Preclass MaterialsTop VidsNo ratings yet
- CH 141: Bone and Joint Infections Self-Assessment Question-AnswersDocument3 pagesCH 141: Bone and Joint Infections Self-Assessment Question-AnswersTop VidsNo ratings yet
- CH 142: Sepsis and Septic Shock ANSWERSDocument2 pagesCH 142: Sepsis and Septic Shock ANSWERSTop VidsNo ratings yet
- CH 136: GI Infections and Enterotoxigenic Poisonings SELF-ASSESSMENT QUESTIONSDocument4 pagesCH 136: GI Infections and Enterotoxigenic Poisonings SELF-ASSESSMENT QUESTIONSTop VidsNo ratings yet
- Karen Barker - Developing and Leading An Evidence Based Orthopaedic Physiotherapy ServiceDocument24 pagesKaren Barker - Developing and Leading An Evidence Based Orthopaedic Physiotherapy ServiceManisha KarnaniNo ratings yet
- 00011Document10 pages00011M Joaquin Robles OrtizNo ratings yet
- 14 Surgical Procedures Discectomy and HerniectomyDocument10 pages14 Surgical Procedures Discectomy and Herniectomydrkis200No ratings yet
- Mckenzie For LBP HNPDocument15 pagesMckenzie For LBP HNPRiri NandaNo ratings yet
- 2023 WAVWatch HandbookDocument24 pages2023 WAVWatch Handbookfelixcalderon562No ratings yet
- Physical Therapy For Low Back PainDocument6 pagesPhysical Therapy For Low Back PainCharles LimbuNo ratings yet
- The Oswestry Disability IndexDocument3 pagesThe Oswestry Disability IndexjuanNo ratings yet
- A Case Study of A 23 Year Old Woman With Ewing's SarcomaDocument2 pagesA Case Study of A 23 Year Old Woman With Ewing's SarcomaSoleil SierraNo ratings yet
- Low Back PainDocument12 pagesLow Back PainKARLOS ALVARO ACURIO ORTIZNo ratings yet
- Exercise in Cardiac RehabilitationDocument5 pagesExercise in Cardiac RehabilitationАлексNo ratings yet
- 7.PT Management of LBADocument11 pages7.PT Management of LBASapna ChaudharyNo ratings yet
- Nucleus Arthroplasty Volume IIDocument55 pagesNucleus Arthroplasty Volume IIHelifunoNo ratings yet
- Potts DiseaseDocument8 pagesPotts Diseaseaimeeros0% (2)
- AXIOM DRX9000 Ver 2 For UploadDocument14 pagesAXIOM DRX9000 Ver 2 For UploadNik Haniff HanafiNo ratings yet
- Empire BCBS 2017Document17 pagesEmpire BCBS 2017Bishara WilsonNo ratings yet
- Cons Study Summary QuiestionsDocument124 pagesCons Study Summary QuiestionsCons Miyu HimeNo ratings yet
- Neuropathic Pain: DR - Dr.Thomas Eko P. Sps (K) Bagian/Smf Neurologi FK Unud/ Rsup DenpasarDocument85 pagesNeuropathic Pain: DR - Dr.Thomas Eko P. Sps (K) Bagian/Smf Neurologi FK Unud/ Rsup DenpasarCox AbeeNo ratings yet
- Deyo 1992Document6 pagesDeyo 1992Wwwanand111No ratings yet
- Tan Ah Kau V The Government of Malaysia - (2Document17 pagesTan Ah Kau V The Government of Malaysia - (2Arvin ANo ratings yet
- Family Worried About Missing Woman: Welcome Home To CadillacDocument36 pagesFamily Worried About Missing Woman: Welcome Home To Cadillaccn_cadillacmiNo ratings yet
- Hip Vs SpineDocument12 pagesHip Vs Spinevaibhav gowdaNo ratings yet