You might also like
- Proulx Et Al (Eds.) - The Wiley Handbook of What Works With Sexual Offenders. Contemporary Perspectives in Theory, Assessment, Treatment, (2020)Document530 pagesProulx Et Al (Eds.) - The Wiley Handbook of What Works With Sexual Offenders. Contemporary Perspectives in Theory, Assessment, Treatment, (2020)willl100% (1)
- Sample Paper 3 Answer PDFDocument58 pagesSample Paper 3 Answer PDFAhhh HahahaNo ratings yet
- Biomedical Medical Equipment Key Performance Indicators (Kpi /QPS)Document4 pagesBiomedical Medical Equipment Key Performance Indicators (Kpi /QPS)Natasha Bhasin100% (5)
- Ansi-Aami DF80-2003Document16 pagesAnsi-Aami DF80-2003lucasromano21No ratings yet
- Fault Diagnosis and Sustainable Control of Wind Turbines: Robust Data-Driven and Model-Based StrategiesFrom EverandFault Diagnosis and Sustainable Control of Wind Turbines: Robust Data-Driven and Model-Based StrategiesRating: 4 out of 5 stars4/5 (1)
- The People of The Materia Medica World: A Comparative Materia Medica Part-1Document5 pagesThe People of The Materia Medica World: A Comparative Materia Medica Part-1Paromita Dasgupta50% (2)
- ANSI AMM EC13-2002 - Frecuencia CardiacaDocument87 pagesANSI AMM EC13-2002 - Frecuencia CardiacaJHONJA1100% (2)
- Commissioning and Qualification ASTM ApproachDocument0 pagesCommissioning and Qualification ASTM Approachvenki_beeNo ratings yet
- Aami RD520408 PDFDocument53 pagesAami RD520408 PDFrossyNo ratings yet
- SOP For Procurement of Medical DevicesDocument2 pagesSOP For Procurement of Medical DevicesMuhammad Nisar33% (3)
- Homework 6Document19 pagesHomework 6Trần Phạm Minh ĐăngNo ratings yet
- Leyte Department of Education Personal Development DocumentDocument2 pagesLeyte Department of Education Personal Development DocumentMaricar Cesista NicartNo ratings yet
- How to Identify and Analyze Hospital RisksDocument12 pagesHow to Identify and Analyze Hospital Risksver_at_workNo ratings yet
- JCE 0b013e31829a2a45Document9 pagesJCE 0b013e31829a2a45jlopezhamdanNo ratings yet
- Medical Devices Inspection and Maintenance A Literature ReviewDocument11 pagesMedical Devices Inspection and Maintenance A Literature ReviewAya AhmedNo ratings yet
- Biomedical Hospital EquipmentDocument6 pagesBiomedical Hospital Equipmentee113051No ratings yet
- Planned Preventive MaintenanceDocument4 pagesPlanned Preventive MaintenanceMOHAMMAD AHMADNo ratings yet
- Ei Eqtplan UmDocument6 pagesEi Eqtplan UmHassanBelalNo ratings yet
- EU US PostMarket Surveillance Whitepaper PDFDocument7 pagesEU US PostMarket Surveillance Whitepaper PDFLakshmana Perumal RamarajNo ratings yet
- Standard For Equipment in Critical Care: The Intensive Care SocietyDocument15 pagesStandard For Equipment in Critical Care: The Intensive Care SocietyAhmed Sabaa ayounNo ratings yet
- Aami Ci86 2017Document179 pagesAami Ci86 2017tazerNo ratings yet
- Medical Equipment Management Plan: I PurposeDocument17 pagesMedical Equipment Management Plan: I PurposeSiham SayeedNo ratings yet
- Guideline - Medical Equipment ManagementDocument16 pagesGuideline - Medical Equipment ManagementdvhoangNo ratings yet
- Biomedical Equip PlanningDocument6 pagesBiomedical Equip PlanningOcwich FrancisNo ratings yet
- Critical Care Environment: BOX 2.1 Business Case: Sample HeadingsDocument8 pagesCritical Care Environment: BOX 2.1 Business Case: Sample HeadingsIqbal Yusuf AshariNo ratings yet
- Aami RD520408Document53 pagesAami RD520408dominic100% (1)
- Planning Medical Device Management SRS PlaningDocument11 pagesPlanning Medical Device Management SRS PlaningRajesh KumarNo ratings yet
- Medical Devices Inspection and Maintenance A Literature ReviewDocument10 pagesMedical Devices Inspection and Maintenance A Literature ReviewlchirinoscautinhoNo ratings yet
- Medical Equipment Management - Binseng WangDocument5 pagesMedical Equipment Management - Binseng WangIanca MoraesNo ratings yet
- II510412 PreviewDocument14 pagesII510412 PreviewMiguel Palma MuñozNo ratings yet
- Qre 1084Document14 pagesQre 1084Art RemoNo ratings yet
- AAMIDocument82 pagesAAMIadisurjadiw100% (1)
- Final ThesisDocument69 pagesFinal ThesisAswin WSNo ratings yet
- Of Active Medical Devices-Malaysia Standard MS 2058:2009 Syed Mustafa KamalDocument6 pagesOf Active Medical Devices-Malaysia Standard MS 2058:2009 Syed Mustafa KamalArif YamanNo ratings yet
- Preview Files ST650812 PreviewDocument15 pagesPreview Files ST650812 PreviewDiego Fernando OvalleNo ratings yet
- American Society of ExtraCorporeal Technology Standards and GuidelinesDocument22 pagesAmerican Society of ExtraCorporeal Technology Standards and GuidelinesErkanNo ratings yet
- State of The Art - Precautionary MaintenaceDocument12 pagesState of The Art - Precautionary MaintenacejavinavasNo ratings yet
- Clinical Literature Review Medical DevicesDocument5 pagesClinical Literature Review Medical Devicesea6p1e99100% (1)
- Solving Safety Implications in A Case Based Decision-Support System in MedicineDocument81 pagesSolving Safety Implications in A Case Based Decision-Support System in MedicineClo SerNo ratings yet
- The Role of Clinical Engineers in Reducing Medical Errors: Peer-Review PaperDocument3 pagesThe Role of Clinical Engineers in Reducing Medical Errors: Peer-Review PaperConny Rubio RiquelmeNo ratings yet
- Managing Medical Devices MHRADocument34 pagesManaging Medical Devices MHRALeyla BaşgülNo ratings yet
- Ims 415Document12 pagesIms 415abelnarwatduutNo ratings yet
- Medical Devicesequipment Management Compliance With The Medical MedicalDocument50 pagesMedical Devicesequipment Management Compliance With The Medical MedicalFayez Abu Al SaoudNo ratings yet
- Diagnosis, and TherapiesDocument6 pagesDiagnosis, and TherapiesHoney MacabuhayNo ratings yet
- Clinical Investigation UpdateDocument28 pagesClinical Investigation UpdateMarcBenetPozoNo ratings yet
- Medical Equipment Management PlanDocument4 pagesMedical Equipment Management PlanShallaine MarieNo ratings yet
- Sample Policies For A Clinical Engineering Department: AppendixaDocument15 pagesSample Policies For A Clinical Engineering Department: AppendixamohammedNo ratings yet
- Developing An In-House Computerized Maintenance Management System For HospitalsDocument9 pagesDeveloping An In-House Computerized Maintenance Management System For Hospitalsاديب جازمNo ratings yet
- Comp9 Unit7d Audio TranscriptDocument10 pagesComp9 Unit7d Audio TranscriptP D SpencerNo ratings yet
- BSI MD Usability Engineering Whitepaper UK enDocument13 pagesBSI MD Usability Engineering Whitepaper UK ensrdjan.djordjevic0603No ratings yet
- Efficient Equipment Management Software for HospitalsDocument6 pagesEfficient Equipment Management Software for HospitalshendranatjNo ratings yet
- Process Safety ManagementDocument28 pagesProcess Safety ManagementIndranil Hatua100% (13)
- Clinical Investigation Revised v2Document30 pagesClinical Investigation Revised v2FahadNo ratings yet
- Protocols and procedures for medical equipment managementDocument9 pagesProtocols and procedures for medical equipment managementAmir100% (1)
- 3rd Edition NABH Guidebook 2012 New PDFDocument258 pages3rd Edition NABH Guidebook 2012 New PDFraamki_99No ratings yet
- Ar Fieldsafety PolicyDocument5 pagesAr Fieldsafety Policyme.ddfNo ratings yet
- Instrument Processing, Work Flow and Sterility Assurance: 4 CE CreditsDocument12 pagesInstrument Processing, Work Flow and Sterility Assurance: 4 CE Creditsdruzair007No ratings yet
- Clinical InvestigationDocument2 pagesClinical InvestigationLejlaNo ratings yet
- NEWS CENTER Maine (NCM) Sent A List of Questions To The FDA and These Were Their ResponsesDocument2 pagesNEWS CENTER Maine (NCM) Sent A List of Questions To The FDA and These Were Their ResponsesNEWS CENTER MaineNo ratings yet
- An Integrative Literature Review On Accuracy in Anesthesia Information Management SystemsDocument8 pagesAn Integrative Literature Review On Accuracy in Anesthesia Information Management SystemseldcahvkgNo ratings yet
- SC14-07 01-02 Hospital Preventive Maintenance Memo-AttachDocument16 pagesSC14-07 01-02 Hospital Preventive Maintenance Memo-AttachRaydoon SadeqNo ratings yet
- NYU HOSPITALS CENTER MEDICAL EQUIPMENT MANAGEMENTDocument32 pagesNYU HOSPITALS CENTER MEDICAL EQUIPMENT MANAGEMENTHind Chehabeddine100% (2)
- Guidance For Industry Cybersecurity For Networked Medical Devices Containing Off-the-Shelf (OTS) SoftwareDocument7 pagesGuidance For Industry Cybersecurity For Networked Medical Devices Containing Off-the-Shelf (OTS) Softwarecsellers2642No ratings yet
- Care of PatientsDocument4 pagesCare of PatientsVicente TurasNo ratings yet
- Research16 Scholar PosterDocument1 pageResearch16 Scholar PosterKarthik Raj VNo ratings yet
- ECG Denoising and Compression Using A Modified Extended Kalman Filter StructureDocument9 pagesECG Denoising and Compression Using A Modified Extended Kalman Filter StructureKarthik Raj VNo ratings yet
- Filtering Noisy ECG Signals Using The Extended Kalman Filter Based On A Modified Dynamic ECG ModelDocument4 pagesFiltering Noisy ECG Signals Using The Extended Kalman Filter Based On A Modified Dynamic ECG ModelKarthik Raj VNo ratings yet
- Authors GuidelinesDocument3 pagesAuthors GuidelinesKarthik Raj VNo ratings yet
- De-Noising of Electrocardiogram (ECG) With Adaptive Filter Using MATLABDocument4 pagesDe-Noising of Electrocardiogram (ECG) With Adaptive Filter Using MATLABKarthik Raj VNo ratings yet
- ECG Noise Filtering Using Wavelets With Soft-Thres Holding MethodsDocument4 pagesECG Noise Filtering Using Wavelets With Soft-Thres Holding MethodsKarthik Raj VNo ratings yet
- Arm and Wrist Surface Potential Mapping For Wearable ECG Rhythm Recording Devices A PilotDocument9 pagesArm and Wrist Surface Potential Mapping For Wearable ECG Rhythm Recording Devices A PilotKarthik Raj VNo ratings yet
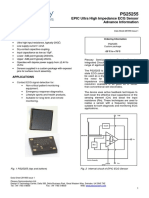
- EPIC Ultra High Impedance ECG Sensor Advance Information: FeaturesDocument7 pagesEPIC Ultra High Impedance ECG Sensor Advance Information: FeaturesKarthik Raj VNo ratings yet
- PS25255 256881Document7 pagesPS25255 256881Karthik Raj VNo ratings yet
- Development and Evaluation of One Arm Electrode BasedDocument4 pagesDevelopment and Evaluation of One Arm Electrode BasedKarthik Raj VNo ratings yet
- Feasiblity of Sngle Arm Ecg BiometricsDocument5 pagesFeasiblity of Sngle Arm Ecg BiometricsKarthik Raj VNo ratings yet
- A Low Latency Electrocardiographic QRS Activity RecoveryDocument10 pagesA Low Latency Electrocardiographic QRS Activity RecoveryKarthik Raj VNo ratings yet
- 4 - 4 - 27689 - 1647803002 - Advantage Training Kris GorriaranDocument1 page4 - 4 - 27689 - 1647803002 - Advantage Training Kris GorriaranKarthik Raj VNo ratings yet
- Patient Monitor FlukeDocument30 pagesPatient Monitor FlukeKarthik Raj VNo ratings yet
- Application Note: Patient Monitor Testing: Related Standards of ReferenceDocument2 pagesApplication Note: Patient Monitor Testing: Related Standards of ReferenceKarthik Raj VNo ratings yet
- E-Commerce and Enterprise SystemsDocument19 pagesE-Commerce and Enterprise SystemsMaria Angela B. GalvezNo ratings yet
- Behavioral Finance-An OverviewDocument46 pagesBehavioral Finance-An OverviewriyasacademicNo ratings yet
- Pc128us 2 Sebm018419 PDFDocument1,029 pagesPc128us 2 Sebm018419 PDFLuis Carlos Ramos100% (1)
- Padeye Deign.Document14 pagesPadeye Deign.Bolarinwa100% (3)
- Kinetic Study of Crystal Violet ReactionDocument10 pagesKinetic Study of Crystal Violet ReactionTaniya GuptaNo ratings yet
- Crime Trend CompletedDocument15 pagesCrime Trend CompletedLENARD LAGASINo ratings yet
- Quadcopter Math Model (Amazing)Document26 pagesQuadcopter Math Model (Amazing)Joseph Oberholtzer83% (6)
- Kumpulan Soal SynonymDocument10 pagesKumpulan Soal SynonymMuhammad Abi PrasetyoNo ratings yet
- Roman Epicurean'ism - Natural Law and HomosexualityDocument21 pagesRoman Epicurean'ism - Natural Law and HomosexualityPapa Giorgio100% (1)
- Employee Satisfaction Analysis and InterpretationDocument29 pagesEmployee Satisfaction Analysis and InterpretationkhayyumNo ratings yet
- Quotation # SO2021/1274870: Quotation Date: Expiration: SalespersonDocument1 pageQuotation # SO2021/1274870: Quotation Date: Expiration: SalespersonAbdul WadoodNo ratings yet
- Un Ejercicio para 2º BACHILLERATO. (An Exercise For Advanced Students.)Document4 pagesUn Ejercicio para 2º BACHILLERATO. (An Exercise For Advanced Students.)Herber HerberNo ratings yet
- Corporal Punishment Versus Capital PunishmentDocument8 pagesCorporal Punishment Versus Capital PunishmentWac GunarathnaNo ratings yet
- The Zwolftonspiel of Josef Matthias Hauer: John RDocument36 pagesThe Zwolftonspiel of Josef Matthias Hauer: John RMax Kühn100% (1)
- Report of Lost, Stolen, Damaged or Destroyed Property: Appendix 75Document3 pagesReport of Lost, Stolen, Damaged or Destroyed Property: Appendix 75Knoll Viado100% (1)
- Use of Imagery in Look Back in AngerDocument3 pagesUse of Imagery in Look Back in AngerArindam SenNo ratings yet
- Extended Paper 2 May 00Document12 pagesExtended Paper 2 May 00Mari Carmen Pérez GómezNo ratings yet
- Principles of Composition SimplifiedDocument20 pagesPrinciples of Composition Simplifiedjoseph arao-araoNo ratings yet
- Leading culturally diverse global teamsDocument20 pagesLeading culturally diverse global teamsEdrick SoegiantoNo ratings yet
- Reset Logon, Networking & PersonalizationDocument10 pagesReset Logon, Networking & PersonalizationDenis TomaNo ratings yet
- The Path To Dignity and Respect enDocument73 pagesThe Path To Dignity and Respect enStan BuddenNo ratings yet
- Concrete Creep PropertiesDocument49 pagesConcrete Creep PropertiesGurram VinayNo ratings yet
- NCP Case 1Document6 pagesNCP Case 1boomer SeargeNo ratings yet
- Chapter 12 - Deliver The Customer ExperienceDocument28 pagesChapter 12 - Deliver The Customer ExperienceKarina Gabriella SanchezNo ratings yet
- Pre Crane Lift ChecklistDocument1 pagePre Crane Lift Checklistg665013No ratings yet