You might also like
- Knee MobilebearingkneeDocument20 pagesKnee MobilebearingkneeJobin VargheseNo ratings yet
- FulltextDocument10 pagesFulltextDenis AlexandruNo ratings yet
- Total Knee Replacement Prosthesis AssignmentDocument33 pagesTotal Knee Replacement Prosthesis Assignmentdr neha gaggarNo ratings yet
- Bme 365 FinalDocument12 pagesBme 365 Finalapi-246126735No ratings yet
- Knee Joint ThesisDocument5 pagesKnee Joint Thesisamywashingtonpittsburgh100% (2)
- Conferences and Reviews Total Hip Arthroplasty: or An A ReconDocument7 pagesConferences and Reviews Total Hip Arthroplasty: or An A ReconSekar CitrasariNo ratings yet
- Total Knee Arthroplasty: Aspects On Improved Fixation in The Younger PatientDocument77 pagesTotal Knee Arthroplasty: Aspects On Improved Fixation in The Younger PatientAndreea TudorascuNo ratings yet
- Implant Selection in Revision Total Knee ArthroplastyDocument10 pagesImplant Selection in Revision Total Knee ArthroplastyAndrés KnubelNo ratings yet
- Bio EssayDocument5 pagesBio EssayWeston MooreNo ratings yet
- Acetabular Component PositioningDocument4 pagesAcetabular Component PositioningPurushotham NalamatiNo ratings yet
- Custom-Designed Orthopedic Implants Evaluated Using Finite Element Analysis of Patient-Specific Computed Tomography Data: Femoral-Component Case StudyDocument11 pagesCustom-Designed Orthopedic Implants Evaluated Using Finite Element Analysis of Patient-Specific Computed Tomography Data: Femoral-Component Case StudySAM IMNo ratings yet
- Cope Land Op TechDocument24 pagesCope Land Op Techsiddig7No ratings yet
- Chapter 1: IntroductionDocument15 pagesChapter 1: IntroductionsafowanNo ratings yet
- J Arth 2015 09 001Document7 pagesJ Arth 2015 09 001Carlos Mauricio Salazar BedollaNo ratings yet
- World's Largest Science, Technology & Medicine Open Access Book PublisherDocument15 pagesWorld's Largest Science, Technology & Medicine Open Access Book PublisherOrhan RamazanNo ratings yet
- Clinics in Sports MedicineDocument202 pagesClinics in Sports MedicineAndres Sanchez EscobedoNo ratings yet
- Crestal Bone Level Alterations in Implant Therapy: August 2011Document35 pagesCrestal Bone Level Alterations in Implant Therapy: August 2011Muhammad Shakeel KhawajaNo ratings yet
- Illustration of Implants in Total Knee ReplacementDocument5 pagesIllustration of Implants in Total Knee ReplacementInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Management of Bone Defects in Primary Knee Arthroplasty: A Case ReportDocument4 pagesManagement of Bone Defects in Primary Knee Arthroplasty: A Case ReportInternational Journal of Recent Innovations in Academic ResearchNo ratings yet
- Lovely Professional UniversityDocument4 pagesLovely Professional Universityshailesh_singh_19No ratings yet
- A Literature Based Comparison of Bone Augmentation.1Document6 pagesA Literature Based Comparison of Bone Augmentation.1drzana78No ratings yet
- Bone Level ImplantsDocument9 pagesBone Level Implantshp1903No ratings yet
- Selected Instructional Course Lectures: The American Academy of Orthopaedic SurgeonsDocument23 pagesSelected Instructional Course Lectures: The American Academy of Orthopaedic SurgeonsGERARDO TORRES RUIZNo ratings yet
- Short ImplantsFrom EverandShort ImplantsBoyd J. TomasettiNo ratings yet
- Microsoft Word - THR Preprint - Thr+PreprintDocument2 pagesMicrosoft Word - THR Preprint - Thr+PreprintNuno GueiralNo ratings yet
- Sto Indus Knee 2Document59 pagesSto Indus Knee 2Purushothama Rao NalamatiNo ratings yet
- The New Bone Level Implants - Clinical Rationale For The Development and Current Indications For Daily Practice by BuserDocument9 pagesThe New Bone Level Implants - Clinical Rationale For The Development and Current Indications For Daily Practice by BuserChristian OkaforNo ratings yet
- Patient-Specific Bone Implants Using Subtractive Rapid PrototypingDocument12 pagesPatient-Specific Bone Implants Using Subtractive Rapid PrototypingsreeshpsNo ratings yet
- Xenograf Versus AllograftDocument14 pagesXenograf Versus AllograftLab NanobiomaterialesNo ratings yet
- ConstreñidosDocument10 pagesConstreñidosCelest ReyesNo ratings yet
- Araoye IB - Use of Intramedullary Carbon Fiber Nail in Hindfoot Fusion A SmallDocument6 pagesAraoye IB - Use of Intramedullary Carbon Fiber Nail in Hindfoot Fusion A SmallHariom ShuklaNo ratings yet
- Guidelines For Treatment Planning of Mandibular Implant OverdentureDocument6 pagesGuidelines For Treatment Planning of Mandibular Implant OverdentureLia DietrichNo ratings yet
- How To Read A Postoperative Knee Replacement RadiographDocument9 pagesHow To Read A Postoperative Knee Replacement RadiographNegru TeodorNo ratings yet
- InMotion - The Knee Disarticulation - It's Better When It's Better and It's Not When It's NotDocument11 pagesInMotion - The Knee Disarticulation - It's Better When It's Better and It's Not When It's NotSucipto HartonoNo ratings yet
- Marginal Bone Loss and Immediate DentureDocument14 pagesMarginal Bone Loss and Immediate DentureSupriya ShuklaNo ratings yet
- Bipolar Hemiarthroplasty ThesisDocument5 pagesBipolar Hemiarthroplasty Thesisgjhs6kja100% (1)
- Plagiarized First 1reportDocument39 pagesPlagiarized First 1reportAbdul RabbaniNo ratings yet
- 1-s2.0-S0011853223001143-CopyDocument8 pages1-s2.0-S0011853223001143-CopychannadrasmaNo ratings yet
- Paper M Time 2012Document5 pagesPaper M Time 2012Elizandro SordiNo ratings yet
- Anterior Cruciate Ligament Reconstruction: A Practical Surgical GuideFrom EverandAnterior Cruciate Ligament Reconstruction: A Practical Surgical GuideNo ratings yet
- Research Paper On Total Knee ReplacementDocument4 pagesResearch Paper On Total Knee Replacementtitamyg1p1j2100% (1)
- Osteogenesis InglesDocument4 pagesOsteogenesis InglesJulio TorresNo ratings yet
- Total Knee Replacement Part I: Radiographic Evaluation: Felix S. Chew, MD, and Catherine C. Roberts, MDDocument6 pagesTotal Knee Replacement Part I: Radiographic Evaluation: Felix S. Chew, MD, and Catherine C. Roberts, MDGERARDO TORRES RUIZ100% (1)
- (Literally "Re-Forming of Joint") : ArthroplastyDocument93 pages(Literally "Re-Forming of Joint") : ArthroplastykotraeNo ratings yet
- Splints BracesDocument18 pagesSplints BracesvaishnaviNo ratings yet
- 1 s2.0 S1991790219308700 MainDocument6 pages1 s2.0 S1991790219308700 MainRonin ZxxNo ratings yet
- The Platform Switching Concept-A Myth or Fact: A Literature ReviewDocument5 pagesThe Platform Switching Concept-A Myth or Fact: A Literature ReviewChifa MusrataNo ratings yet
- Surgical Challenges in Complex Primary Total Hip ADocument9 pagesSurgical Challenges in Complex Primary Total Hip Aehabede6445No ratings yet
- The Effects of Total Ankle Replacement On Ankle J - 2017 - Journal of Sport andDocument6 pagesThe Effects of Total Ankle Replacement On Ankle J - 2017 - Journal of Sport andSisi WeeraNo ratings yet
- Uwrit Annotated Biblio-3Document5 pagesUwrit Annotated Biblio-3api-315967417No ratings yet
- Orthodontically Driven Corticotomy: Tissue Engineering to Enhance Orthodontic and Multidisciplinary TreatmentFrom EverandOrthodontically Driven Corticotomy: Tissue Engineering to Enhance Orthodontic and Multidisciplinary TreatmentFederico BrugnamiNo ratings yet
- J Jds 2019 12 003Document6 pagesJ Jds 2019 12 003aDITYA GUJARENo ratings yet
- A Bio-Inspired Condylar Knee Joint For Leg Amputees and For Knee ImplantsDocument13 pagesA Bio-Inspired Condylar Knee Joint For Leg Amputees and For Knee ImplantsNada GhammemNo ratings yet
- Evolution of Anchors For Cuff Burkhart Arthroscopy 2013Document7 pagesEvolution of Anchors For Cuff Burkhart Arthroscopy 2013harpreet singhNo ratings yet
- Wallace, Maxillary Sinus AugmentationDocument16 pagesWallace, Maxillary Sinus AugmentationChin-lungHsiehNo ratings yet
- Growth Relativity Theory PDFDocument20 pagesGrowth Relativity Theory PDFMonojit DuttaNo ratings yet
- Chirurgia Piciorului ºi GlezneiDocument28 pagesChirurgia Piciorului ºi GlezneiAngela PascarNo ratings yet
- Optimized Trapezoidal Shaped Hip Implant For Total Hip Arthroplasty Using Finite Element AnalysisDocument15 pagesOptimized Trapezoidal Shaped Hip Implant For Total Hip Arthroplasty Using Finite Element AnalysisSergio PluchinskyNo ratings yet
- Oxford Unicompartmental Knee Replacement Literature ReviewDocument4 pagesOxford Unicompartmental Knee Replacement Literature Reviewz0pilazes0m3No ratings yet
- Guidelines For Treatment Planning of Mandibular Implant Overdenture PDFDocument6 pagesGuidelines For Treatment Planning of Mandibular Implant Overdenture PDFjoephinNo ratings yet
- EBM CasesDocument1 pageEBM CasesdnaritaNo ratings yet
- St. John, Isaac Newton and Prediction of MedicanesDocument6 pagesSt. John, Isaac Newton and Prediction of MedicanesMarthaNo ratings yet
- Astm - C338Document3 pagesAstm - C338KuNtii Devi VerdejofNo ratings yet
- Din Ling, 'Miss Sophia's Diary'Document2 pagesDin Ling, 'Miss Sophia's Diary'StudenteNo ratings yet
- Explore Rupnagar's Historical and Religious Sites in 2 DaysTITLEDocument37 pagesExplore Rupnagar's Historical and Religious Sites in 2 DaysTITLEAkshayKumarNo ratings yet
- Applied Mechanics - 341-345 NSQF IrdtDocument4 pagesApplied Mechanics - 341-345 NSQF IrdtTushar KiranNo ratings yet
- Rasa Theory and Its Application in TranslationDocument36 pagesRasa Theory and Its Application in TranslationKamal JajoriyaNo ratings yet
- Notes in Readings in Philippine History: Act of Proclamation of Independence of The Filipino PeopleDocument4 pagesNotes in Readings in Philippine History: Act of Proclamation of Independence of The Filipino PeopleAiris Ramos AgillonNo ratings yet
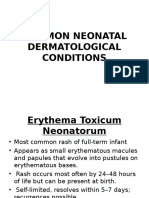
- Common Neonatal Dermatological ConditionsDocument27 pagesCommon Neonatal Dermatological ConditionsArslan SiddiquiNo ratings yet
- ALD PatriciaLockwood TheCommunalMindDocument16 pagesALD PatriciaLockwood TheCommunalMindtillhopstockNo ratings yet
- RacismDocument23 pagesRacismRaj KrishnaNo ratings yet
- 9696 Geography Example Candidate Responses 2011 WEBDocument313 pages9696 Geography Example Candidate Responses 2011 WEBAsma Merchant67% (3)
- Punjab govt grants EOL to doctors for postgraduate trainingDocument2 pagesPunjab govt grants EOL to doctors for postgraduate trainingMasroor HassanNo ratings yet
- Civics OrginalDocument17 pagesCivics OrginalNeb coolNo ratings yet
- Ethics Final ModuleDocument27 pagesEthics Final ModuleEdmond TagubaNo ratings yet
- Amity School of Communication: BA (J&MC), Semester-1 Basics of Print Media Neha BhagatDocument10 pagesAmity School of Communication: BA (J&MC), Semester-1 Basics of Print Media Neha BhagatYash TiwariNo ratings yet
- Audit of Receivables Pre-Assessment: Acctg35Document3 pagesAudit of Receivables Pre-Assessment: Acctg35Jeane Mae BooNo ratings yet
- English K 2 Multi Age Year A Unit 1Document46 pagesEnglish K 2 Multi Age Year A Unit 1celine celineNo ratings yet
- 10 Legacy A1 Unit KeyDocument12 pages10 Legacy A1 Unit KeyHristoMilushevNo ratings yet
- The Tracking Shot in Kapo Serge Daney Senses of CinemaDocument22 pagesThe Tracking Shot in Kapo Serge Daney Senses of CinemaMarcos GonzálezNo ratings yet
- Architecture Statement of PurposeDocument4 pagesArchitecture Statement of PurposeAZAR HOSNo ratings yet
- Journal of Cleaner Production: Fabíola Negreiros de Oliveira, Adriana Leiras, Paula CerynoDocument15 pagesJournal of Cleaner Production: Fabíola Negreiros de Oliveira, Adriana Leiras, Paula CerynohbNo ratings yet
- Individual Project Instructions - 5aDocument1 pageIndividual Project Instructions - 5aIkhram JohariNo ratings yet
- Experimental and Numerical Investigation of Rotating Bladed Disk Forced Response Using Under-Platform Friction DampersDocument11 pagesExperimental and Numerical Investigation of Rotating Bladed Disk Forced Response Using Under-Platform Friction DamperssenthilNo ratings yet
- Mastery-Test-Math-10-Quarter-3 Week 5-6Document1 pageMastery-Test-Math-10-Quarter-3 Week 5-6Sheila Mauricio GarciaNo ratings yet
- 3 Affect Regulation, Mentalization, and The Development of The Self (Peter Fonagy, Gyorgy Gergely, Elliot L. Jurist Etc.) - 211-259Document49 pages3 Affect Regulation, Mentalization, and The Development of The Self (Peter Fonagy, Gyorgy Gergely, Elliot L. Jurist Etc.) - 211-259Sergio Andres Rico AvendanoNo ratings yet
- The Use of MuseScore (A Music Transcribing Computer Software) As A Tool in Enhancing The Knowledge and Skills of Non-Music Major Teachers of Tayabas West Central School - IDocument13 pagesThe Use of MuseScore (A Music Transcribing Computer Software) As A Tool in Enhancing The Knowledge and Skills of Non-Music Major Teachers of Tayabas West Central School - IRyan Chester ManzanaresNo ratings yet
- Brown v. Board of EducationDocument1 pageBrown v. Board of EducationSam TaborNo ratings yet
- Free-Range Chicken Farming PDFDocument138 pagesFree-Range Chicken Farming PDFDennis MacedoNo ratings yet
- Niccolò MachiavelliDocument3 pagesNiccolò MachiavelliAm YuniqueNo ratings yet