You might also like
- Best Practice Guidelines Physiotherapy EIPIC 2Document66 pagesBest Practice Guidelines Physiotherapy EIPIC 2Ankur ShahNo ratings yet
- Deresky Tif 03Document21 pagesDeresky Tif 03UNF2012100% (8)
- Argumentative EssayDocument6 pagesArgumentative Essayapi-28603785175% (4)
- Nursing CatalogDocument27 pagesNursing Catalogrrockel100% (1)
- Iapt Bame PPG 2019 PDFDocument52 pagesIapt Bame PPG 2019 PDFKarolina KaliszNo ratings yet
- Artificial Intelligence in Healthcare: Unlocking its PotentialFrom EverandArtificial Intelligence in Healthcare: Unlocking its PotentialNo ratings yet
- The Riddle ScaleDocument3 pagesThe Riddle ScaleArsene LupinNo ratings yet
- Yoshino - The Epistemic Contract of Bisexual ErasureDocument110 pagesYoshino - The Epistemic Contract of Bisexual ErasureMathieu TrachmanNo ratings yet
- CSEC English SBADocument20 pagesCSEC English SBArenay campbell0% (2)
- Nursing and Euthanasia: A Narrative Review of The Nursing Ethics LiteratureDocument16 pagesNursing and Euthanasia: A Narrative Review of The Nursing Ethics LiteratureFirda ApriyantiNo ratings yet
- Understanding Why Patients Request EuthanasiaDocument11 pagesUnderstanding Why Patients Request EuthanasiaSara Juliana Rosero MedinaNo ratings yet
- A Review of The Australian Healthcare System: A Policy PerspectiveDocument14 pagesA Review of The Australian Healthcare System: A Policy PerspectiveNisa FitriyaniNo ratings yet
- Abd Hamid 2017Document5 pagesAbd Hamid 2017M'ir Usai'lNo ratings yet
- Perin Et Al 2023 Clinical Ethics Committee in An Oncological Research Hospital Two Years ReportDocument15 pagesPerin Et Al 2023 Clinical Ethics Committee in An Oncological Research Hospital Two Years ReportFatimahNo ratings yet
- Specialist Palliative Care Services For Older People in Primary Care: A Systematic Review Using Narrative SynthesisDocument17 pagesSpecialist Palliative Care Services For Older People in Primary Care: A Systematic Review Using Narrative SynthesisKavinkumar SaravananNo ratings yet
- SAGEOpenMedicine-2016-Mbemba-etal 13 05 16 PDFDocument9 pagesSAGEOpenMedicine-2016-Mbemba-etal 13 05 16 PDFmlllNo ratings yet
- 1144 AuthorArticle 205 1 10 20210930Document6 pages1144 AuthorArticle 205 1 10 20210930joyelisadhty0906No ratings yet
- Health Regulation of Dietary SupplementsDocument22 pagesHealth Regulation of Dietary SupplementsApróné Török IbolyaNo ratings yet
- Actitud Ante La MuerteDocument8 pagesActitud Ante La Muertealberto cabelloNo ratings yet
- ECONOMICS MAIN NOTE 08-Jun-2021 15-29-38Document9 pagesECONOMICS MAIN NOTE 08-Jun-2021 15-29-38Richard OrisakweNo ratings yet
- Patient Education and CounselingDocument9 pagesPatient Education and Counselingdev darma karinggaNo ratings yet
- Cash 2021Document20 pagesCash 2021mariee_25No ratings yet
- Social Care Research: What's On The WebDocument2 pagesSocial Care Research: What's On The WebAjideniNo ratings yet
- Divan 2015 PASS AdaptationprocessDocument9 pagesDivan 2015 PASS AdaptationprocessErick David Barrios BastardoNo ratings yet
- Craig Et Al. - 2017 - Natural Experiments An Overview of Methods, ApproDocument21 pagesCraig Et Al. - 2017 - Natural Experiments An Overview of Methods, ApproEnrique Zamora VivancoNo ratings yet
- Jurnal Inter2Document15 pagesJurnal Inter2Mhd FirdausNo ratings yet
- IT-supported Integrated Care Pathways For Diabetes: A Compilation and Review of Good PracticesDocument15 pagesIT-supported Integrated Care Pathways For Diabetes: A Compilation and Review of Good PracticesKenny BellodasNo ratings yet
- Listen, Care, and Going Extra Mile: Guiding Principles For Physicians and Teachers in Health-Care ProfessionDocument6 pagesListen, Care, and Going Extra Mile: Guiding Principles For Physicians and Teachers in Health-Care ProfessionMarialee PlanNo ratings yet
- Nursing, Advocacy and Public Policy: Shane Matthew Scott and P Anne ScottDocument11 pagesNursing, Advocacy and Public Policy: Shane Matthew Scott and P Anne Scottlorelyn cabreraNo ratings yet
- Acceptability and Comprehensiveness of Cagayan State University Vision, Mission, College Goals and Bachelor of Public Administration Program ObjectivesDocument9 pagesAcceptability and Comprehensiveness of Cagayan State University Vision, Mission, College Goals and Bachelor of Public Administration Program Objectivesdomenick sadamaNo ratings yet
- S-LCA Methodological SheetsDocument152 pagesS-LCA Methodological SheetsCatallina arerizaNo ratings yet
- Sustainability SJRDocument18 pagesSustainability SJRNórida Pájaro GómezNo ratings yet
- Design of Knowledge Management System For Diabetic Complication DiseasesDocument7 pagesDesign of Knowledge Management System For Diabetic Complication DiseasesKutale TukuraNo ratings yet
- Transitionskillsforrecovery PDFDocument220 pagesTransitionskillsforrecovery PDFRudy KolderNo ratings yet
- 2018 CalderDocument13 pages2018 CalderIsabelle LunaNo ratings yet
- Macpherson Hart Heaver Artsforresilience JSWDocument21 pagesMacpherson Hart Heaver Artsforresilience JSWDEWI SHINTYA PRATIWINo ratings yet
- Adult Learning Theories in Context - A Quick Guide For Healthcare Professional EducatorsDocument10 pagesAdult Learning Theories in Context - A Quick Guide For Healthcare Professional EducatorsjharpatNo ratings yet
- EcoSattva Project BriefDocument8 pagesEcoSattva Project BriefMansi DwivediNo ratings yet
- Dibalik ComprehensiveDocument16 pagesDibalik ComprehensiveWardah HanifahNo ratings yet
- Time To Act Mature - Gearing Ehealth Evaluations Towards Technology Readiness LevelsDocument5 pagesTime To Act Mature - Gearing Ehealth Evaluations Towards Technology Readiness LevelsMaría Alejandra Silva PedrazaNo ratings yet
- Revisions To The Code of Ethics For The Nutrition&Document4 pagesRevisions To The Code of Ethics For The Nutrition&carolina prietoNo ratings yet
- C P A G F A Q (Faq) F P P MDocument2 pagesC P A G F A Q (Faq) F P P MDewanggaWahyuPrajaNo ratings yet
- Hebert 2008 PDFDocument15 pagesHebert 2008 PDFAndrew GilbertNo ratings yet
- The Essential Conditions Needed (EN)Document16 pagesThe Essential Conditions Needed (EN)WILLIAM GRANJA ANGULONo ratings yet
- Developing and Enhancing Adherence To A Telehealth ABA Parent Training Curriculum For Caregivers of Children With AutismDocument17 pagesDeveloping and Enhancing Adherence To A Telehealth ABA Parent Training Curriculum For Caregivers of Children With AutismThiago Brito MunizNo ratings yet
- Anpc 6 140Document3 pagesAnpc 6 140Dessy EkaNo ratings yet
- Practitioners' Perceptions of The Picture Exchange Communication System ForDocument8 pagesPractitioners' Perceptions of The Picture Exchange Communication System ForMuhammad Shehr YarNo ratings yet
- Szekelyetal.2024 Theefficacyofpsychoeducationtoimprovepersonalskillsandwell Beingamonghealth Careprofessionalsreturningtoclinicalpractice Apilotpre Poststudy3Document14 pagesSzekelyetal.2024 Theefficacyofpsychoeducationtoimprovepersonalskillsandwell Beingamonghealth Careprofessionalsreturningtoclinicalpractice Apilotpre Poststudy3dragonmasterleyNo ratings yet
- International Journal of Nursing StudiesDocument8 pagesInternational Journal of Nursing StudiesJos CanalesNo ratings yet
- Corkum, Et Al. (2015) Web-Based Intervention For Teachers of Elementary Students With ADHDDocument14 pagesCorkum, Et Al. (2015) Web-Based Intervention For Teachers of Elementary Students With ADHDjuanNo ratings yet
- Occupational Therapy INTERVENCTIONS IN PRIMARY CAREDocument6 pagesOccupational Therapy INTERVENCTIONS IN PRIMARY CAREIRENE ORTIZ LOPEZNo ratings yet
- The Nursing Centre As A Collaborative Approach To Integrate Community Health Service and Nursing Education in IndonesiaDocument3 pagesThe Nursing Centre As A Collaborative Approach To Integrate Community Health Service and Nursing Education in IndonesiaTentry Fuji PurwantiNo ratings yet
- The 8 Steps + FINAL Compressed FileDocument41 pagesThe 8 Steps + FINAL Compressed FileMuhammad AzliNo ratings yet
- Final ChapterwcompleteRRL.1 2Document34 pagesFinal ChapterwcompleteRRL.1 2Jeah AcostaNo ratings yet
- The Lancet Regional Health - Western Pacific: Research PaperDocument13 pagesThe Lancet Regional Health - Western Pacific: Research PaperdyahyuNo ratings yet
- Clinical Ethical Practice and Associated Factors in Healthcare Facilities in Ethiopia: A Cross-Sectional StudyDocument12 pagesClinical Ethical Practice and Associated Factors in Healthcare Facilities in Ethiopia: A Cross-Sectional Studymulugeta abateNo ratings yet
- Care Practices of Specialized Outpatient Pediatric Palliative Care Teams in Collaboration WithDocument9 pagesCare Practices of Specialized Outpatient Pediatric Palliative Care Teams in Collaboration WithMădălina MarincaşNo ratings yet
- Social Audit Performance of Cooperatives in NortheDocument14 pagesSocial Audit Performance of Cooperatives in Northecacadcadaan14No ratings yet
- Strategies For The Implementation of Palliative Care Education and Organizational Interventions in Long-Term Care FacilitiesDocument13 pagesStrategies For The Implementation of Palliative Care Education and Organizational Interventions in Long-Term Care FacilitiescharmyshkuNo ratings yet
- Lean Management in The Emergency Department: June 2018Document14 pagesLean Management in The Emergency Department: June 2018fajr muzzammilNo ratings yet
- Journal ReadingDocument14 pagesJournal Readingncc dharmaisNo ratings yet
- Development and Management of Networks of Care at The End of Life (The REDCUIDA Intervention) : Protocol For A Nonrandomized Controlled TrialDocument9 pagesDevelopment and Management of Networks of Care at The End of Life (The REDCUIDA Intervention) : Protocol For A Nonrandomized Controlled TrialDaniela Rojas MejiaNo ratings yet
- Recruitment of Caregivers Into Health Services ResDocument10 pagesRecruitment of Caregivers Into Health Services ResMónica Encantado GaboleiroNo ratings yet
- Santé Mentale Au Québec: Mary Ann TestDocument30 pagesSanté Mentale Au Québec: Mary Ann TestJejdkdNo ratings yet
- SAGE - Nurses Experiences of Ethical REVIEWDocument15 pagesSAGE - Nurses Experiences of Ethical REVIEWStee Al-FradianteeNo ratings yet
- Public Receptivity Towards LGBT in Recent Times Malaysia LGBT PerspectivesDocument14 pagesPublic Receptivity Towards LGBT in Recent Times Malaysia LGBT PerspectivesElexthéo JoseNo ratings yet
- REILLYMakingthe Invisible VisibleDocument12 pagesREILLYMakingthe Invisible VisibleElexthéo JoseNo ratings yet
- Reality of Gender Discrimination On WorkplaceDocument9 pagesReality of Gender Discrimination On WorkplaceElexthéo JoseNo ratings yet
- Gender Discrimination: August 2021Document13 pagesGender Discrimination: August 2021Elexthéo JoseNo ratings yet
- PDKDiss 2010 ArticleDocument7 pagesPDKDiss 2010 ArticleElexthéo JoseNo ratings yet
- Assessing The Effects of A Real-Life Contact InterDocument18 pagesAssessing The Effects of A Real-Life Contact InterElexthéo JoseNo ratings yet
- Article Castro Margate FinalDocument23 pagesArticle Castro Margate FinalElexthéo JoseNo ratings yet
- 3 Fdef 5Document11 pages3 Fdef 5Elexthéo JoseNo ratings yet
- Grade 4 6 Edukasyong Pantahanan at PangkabuhayanDocument54 pagesGrade 4 6 Edukasyong Pantahanan at Pangkabuhayanmary graceNo ratings yet
- 2021 Ladd Grace ThesisDocument66 pages2021 Ladd Grace ThesisElexthéo JoseNo ratings yet
- 2020 Gender Sensitive UniversityDocument210 pages2020 Gender Sensitive UniversityElexthéo JoseNo ratings yet
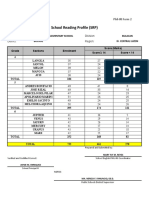
- School Reading Profile (SRP) : School: Division: District: RegionDocument2 pagesSchool Reading Profile (SRP) : School: Division: District: RegionElexthéo JoseNo ratings yet
- Nder Sensitizationatworkplace Impacton Deviant Workplace Behaviorsin Information Technologysectorin IndiaDocument11 pagesNder Sensitizationatworkplace Impacton Deviant Workplace Behaviorsin Information Technologysectorin IndiaElexthéo JoseNo ratings yet
- 4 - Sses - Masigasig First Jennilyn H. Aquino - ManahanDocument6 pages4 - Sses - Masigasig First Jennilyn H. Aquino - ManahanElexthéo JoseNo ratings yet
- GEYLUVDocument2 pagesGEYLUVZoeben Kent S. CarboneraNo ratings yet
- UTSDocument2 pagesUTSMikaela LozanoNo ratings yet
- Gender and Society: Bohol Island State University College of Business, Arts and SciencesDocument10 pagesGender and Society: Bohol Island State University College of Business, Arts and SciencesMaria GraciasNo ratings yet
- Transgender GuideDocument22 pagesTransgender GuideAlexandre Gonçalves50% (2)
- AnswersDocument1 pageAnswersapi-397698820No ratings yet
- Design PhilosophyDocument3 pagesDesign Philosophygene2693No ratings yet
- Erotic Art Prostitution Sex London 3 Of26 PDFDocument2 pagesErotic Art Prostitution Sex London 3 Of26 PDFJoeNo ratings yet
- Homosexuality in Church Society Charting The IssuesDocument131 pagesHomosexuality in Church Society Charting The IssuesWenJun LeowNo ratings yet
- Sexuality Development in Childhood: September 2020Document56 pagesSexuality Development in Childhood: September 2020Dr. EAZYNo ratings yet
- Sykes, Transsexual and Transgender Policies in SportDocument11 pagesSykes, Transsexual and Transgender Policies in SportDavidDuránNo ratings yet
- NCCI Gender and Sexuality PresentationDocument9 pagesNCCI Gender and Sexuality PresentationPompi BanerjeeNo ratings yet
- LGBT and The Law - Protecting The Rights of Minorities in Nigeria PDFDocument84 pagesLGBT and The Law - Protecting The Rights of Minorities in Nigeria PDFNnanna MbaNo ratings yet
- Homosexuality. It Can Be Found Among Every Class of People Just Like Other Sexual Behaviors As AdulteryDocument5 pagesHomosexuality. It Can Be Found Among Every Class of People Just Like Other Sexual Behaviors As AdulteryDhalia SisonNo ratings yet
- Mara Et Al. - 2020 - Strategies For Coping With LGBT Discrimination atDocument16 pagesMara Et Al. - 2020 - Strategies For Coping With LGBT Discrimination atRMADVNo ratings yet
- Ang Ladlad LGBT Party v. COMELECDocument2 pagesAng Ladlad LGBT Party v. COMELECJImlan Sahipa IsmaelNo ratings yet
- Bisexual Movements: by Brett Genny BeemynDocument4 pagesBisexual Movements: by Brett Genny BeemynJerico RiveraNo ratings yet
- Sogie 101 7-7-15Document26 pagesSogie 101 7-7-15Murphy Red100% (1)
- UC1 CBLM Observing Gender Sensitivty in The WorkplaceDocument68 pagesUC1 CBLM Observing Gender Sensitivty in The WorkplaceErethro CytesNo ratings yet
- Thesis Proposal FormDocument5 pagesThesis Proposal FormJohn Rey De la PeñaNo ratings yet
- Sanchez Hucles Davis 2010Document11 pagesSanchez Hucles Davis 2010api-286221742No ratings yet
- Interpersonal Justice and DevianceDocument52 pagesInterpersonal Justice and DevianceMohammad Sohail RashidNo ratings yet
- Uts-Reviewwer MidtermDocument6 pagesUts-Reviewwer MidtermElvira MirajulNo ratings yet
- Canagarajah 2006 TESOL at 40 - What Are The IssuesDocument264 pagesCanagarajah 2006 TESOL at 40 - What Are The IssuesJasonKclNo ratings yet
- Pro-Kontra Terhadap Pandangan Mengenai LGBT Berdasarkan Perspektif HAM, Agama, Dan Hukum Di IndonesiaDocument22 pagesPro-Kontra Terhadap Pandangan Mengenai LGBT Berdasarkan Perspektif HAM, Agama, Dan Hukum Di IndonesiaLaela HimmahNo ratings yet
- Exposing The Myth ofDocument7 pagesExposing The Myth ofnowayborngay0% (1)