You might also like
- PANCE Pearls Master 2013Document19 pagesPANCE Pearls Master 2013Haley Shields100% (7)
- Microbiology 2Document53 pagesMicrobiology 2pikachuNo ratings yet
- Pediatrics 2003 Cunningham 436 40Document7 pagesPediatrics 2003 Cunningham 436 40Putu Agus GrantikaNo ratings yet
- Hearing Screening Pediatrics 2009Document14 pagesHearing Screening Pediatrics 2009Francisco ValleNo ratings yet
- Early Identification of Hearing Loss in HighDocument4 pagesEarly Identification of Hearing Loss in HighKakaNo ratings yet
- Asthma Risk in Children Born After Infertility TreatmentDocument9 pagesAsthma Risk in Children Born After Infertility TreatmentKinjal ShahNo ratings yet
- 2016 franciaDocument6 pages2016 franciaRomi Sepúlveda SaldiviaNo ratings yet
- PSSJN - Volume 1 - Issue 2 - Pages 265-280Document16 pagesPSSJN - Volume 1 - Issue 2 - Pages 265-280Praveen YadavNo ratings yet
- Paediatric Dysphagia: How I Inform My Decisions (1) - Penetrating QuestionsDocument3 pagesPaediatric Dysphagia: How I Inform My Decisions (1) - Penetrating QuestionsSpeech & Language Therapy in PracticeNo ratings yet
- Aynalem 2020@journal - Pone.0235544Document14 pagesAynalem 2020@journal - Pone.0235544Huệ MinhNo ratings yet
- Deaf Mute PaperDocument11 pagesDeaf Mute PaperneviNo ratings yet
- Pone 0230978Document20 pagesPone 0230978Sanket TelangNo ratings yet
- International Journal of Pediatric Otorhinolaryngology: Mark W. Steehler, Matthew K. Steehler, Earl H. HarleyDocument5 pagesInternational Journal of Pediatric Otorhinolaryngology: Mark W. Steehler, Matthew K. Steehler, Earl H. HarleyJohan Sebastian Perea PalaciosNo ratings yet
- Prevalence of Asthma in Australian ChildrenDocument4 pagesPrevalence of Asthma in Australian Childrenoktha_pohanNo ratings yet
- Prevalence of The Cleft Lip and Palate Among Newborn Babies in Sulaimani Obstetrics and Gynecological HospitalDocument3 pagesPrevalence of The Cleft Lip and Palate Among Newborn Babies in Sulaimani Obstetrics and Gynecological HospitalIOSRjournalNo ratings yet
- Clinical Guidelines - OMEDocument24 pagesClinical Guidelines - OMEGaurav MedikeriNo ratings yet
- Chronic Effects of Pediatric Ear Infections On Postural StabilityDocument6 pagesChronic Effects of Pediatric Ear Infections On Postural StabilityFajar SutrisnaNo ratings yet
- UntitledDocument2 pagesUntitledIRA ODETTE GATUSNo ratings yet
- Evidence-Based Systematic Review: Effects of Oral Motor Interventions On Feeding and Swallowing in Preterm InfantsDocument20 pagesEvidence-Based Systematic Review: Effects of Oral Motor Interventions On Feeding and Swallowing in Preterm InfantsKrystyna AquinoNo ratings yet
- Effect of Aspiration On The Lungs in Children: A Comparison Using Chest Computed Tomography FindingsDocument7 pagesEffect of Aspiration On The Lungs in Children: A Comparison Using Chest Computed Tomography FindingsYuliaAntolisNo ratings yet
- Ome 2004Document20 pagesOme 2004Novy Sylvia WardanaNo ratings yet
- Prevalence of Birth Asphyxia and Associated Factors Among Neonates Delivered in Dilchora Referral Hospital in Dire Dawa Eastern Et 2090 7214 1000279 PDFDocument7 pagesPrevalence of Birth Asphyxia and Associated Factors Among Neonates Delivered in Dilchora Referral Hospital in Dire Dawa Eastern Et 2090 7214 1000279 PDFrikarikaNo ratings yet
- Quality of Nursing Care Provided For PreDocument16 pagesQuality of Nursing Care Provided For PreAmmar Mustafa Mahadi AlzeinNo ratings yet
- The Neonatal Intubation Causes Defects in PrimaryDocument9 pagesThe Neonatal Intubation Causes Defects in PrimaryfatimahNo ratings yet
- Bab IDocument5 pagesBab IWahyu Eka WidiantyNo ratings yet
- Down Syndrome and Feeding ProblemsDocument8 pagesDown Syndrome and Feeding Problemsfelix08121992No ratings yet
- Andersson 2018Document7 pagesAndersson 2018FernandaPïlapañaNo ratings yet
- Association Between Exclusive Breastfeeding and The Risk of Tonsilitis in Children Under Five in Demak, Central JavaDocument6 pagesAssociation Between Exclusive Breastfeeding and The Risk of Tonsilitis in Children Under Five in Demak, Central Javainggrid28 syaputriNo ratings yet
- Otitis Media With Effusion - GuidelineDocument41 pagesOtitis Media With Effusion - GuidelineAurel OctavianNo ratings yet
- Training Adults and Children with ASD to be Compliant with Dental AssessmentsDocument10 pagesTraining Adults and Children with ASD to be Compliant with Dental AssessmentsSpecial CareNo ratings yet
- Ceo 2018 01781Document7 pagesCeo 2018 01781Fuad hadyanNo ratings yet
- 118876-Article Text-328375-1-10-20150701Document9 pages118876-Article Text-328375-1-10-20150701Ahmad MuhammadNo ratings yet
- Otolaryngology Head and Neck Surgery 2016 Rosenfeld S1 S41Document41 pagesOtolaryngology Head and Neck Surgery 2016 Rosenfeld S1 S41Novy Sylvia Wardana100% (1)
- Otitis Media in Infants - Is It Related To Improper Breast Feeding Techniques?Document5 pagesOtitis Media in Infants - Is It Related To Improper Breast Feeding Techniques?Najla ShuaibNo ratings yet
- PIIS1098301518322721Document7 pagesPIIS1098301518322721Francelia Quiñonez RuvalcabaNo ratings yet
- Written Assignment 1Document5 pagesWritten Assignment 1api-401934380No ratings yet
- CONSIDERACIONES CLIN EN PEDIATRICOS EN LA EV CLINICA VS EVALUACION INSTURMENTAL DE LA DEGLUCIONDocument8 pagesCONSIDERACIONES CLIN EN PEDIATRICOS EN LA EV CLINICA VS EVALUACION INSTURMENTAL DE LA DEGLUCIONAngélica GarcíaNo ratings yet
- 1 s2.0 S0021755719305947 MainDocument7 pages1 s2.0 S0021755719305947 MainCatarina IglesiasNo ratings yet
- Sample Chapter TwoDocument2 pagesSample Chapter TwoMohamed Ali Abdi MahadalleNo ratings yet
- Clinical Study: Newborn Hearing Screening and Early Diagnostic in The NICUDocument11 pagesClinical Study: Newborn Hearing Screening and Early Diagnostic in The NICUannisanangNo ratings yet
- 2020 - LSHSS 20 00089Document13 pages2020 - LSHSS 20 00089Meva'a RogerNo ratings yet
- 9 JurnalDocument83 pages9 JurnalWanda AndiniNo ratings yet
- Clinical Practice Guideline Update for Otitis Media with EffusionDocument87 pagesClinical Practice Guideline Update for Otitis Media with EffusionMonicaDyaneTahaparyNo ratings yet
- MainDocument6 pagesMainDiana Catalina Avila BareñoNo ratings yet
- An Update On The Perioperative Management of Children With Upper Respiratory InfectionsDocument18 pagesAn Update On The Perioperative Management of Children With Upper Respiratory InfectionsAditya ManjunathNo ratings yet
- Understanding Childhood Asthma and The Development of The Respiratory TractDocument12 pagesUnderstanding Childhood Asthma and The Development of The Respiratory TractluchoNo ratings yet
- Neonatal ResuscitationDocument14 pagesNeonatal ResuscitationedwinNo ratings yet
- Benefits of Frenulotomy in Infants With AnkyloglossiaDocument4 pagesBenefits of Frenulotomy in Infants With Ankyloglossiaadrian bouzasNo ratings yet
- Risk Factors For Otitis Media in Rural, Preschool South Indian ChildrenDocument20 pagesRisk Factors For Otitis Media in Rural, Preschool South Indian ChildrengoolnuulNo ratings yet
- Features of Unilateral Hearing Loss Detected by Newborn Hearing ScreeningDocument9 pagesFeatures of Unilateral Hearing Loss Detected by Newborn Hearing Screening21 TMHNo ratings yet
- Presentación y Manejo de Infecciones Orofaciales en NiñosDocument10 pagesPresentación y Manejo de Infecciones Orofaciales en NiñosFelipe SuárezNo ratings yet
- Pacifier Use in Children: A Review of Recent LiteratureDocument10 pagesPacifier Use in Children: A Review of Recent LiteratureCindy Uswatun KhasanahNo ratings yet
- Risk Factors for Failed Neonatal Hearing Screening and Their Relationship to Screening OutcomesDocument6 pagesRisk Factors for Failed Neonatal Hearing Screening and Their Relationship to Screening OutcomesRendra SyaniNo ratings yet
- PYMS Is A Reliable Malnutrition Screening ToolsDocument8 pagesPYMS Is A Reliable Malnutrition Screening ToolsRika LedyNo ratings yet
- Feeding ArvedsonDocument10 pagesFeeding ArvedsonPablo Oyarzún Dubó100% (1)
- Rovers Study ArticleDocument4 pagesRovers Study ArticleHongMingNo ratings yet
- Bmri2021 5550267Document13 pagesBmri2021 5550267Shahid ShaikhNo ratings yet
- Facial Pattern and Hyoid Bone Changes in Children with Sleep ApneaDocument4 pagesFacial Pattern and Hyoid Bone Changes in Children with Sleep ApneaCEBDOF BRASILNo ratings yet
- Otolaryngol - Head Neck Surg - 2016 - Rosenfeld - Clinical Practice Guideline Otitis Media With Effusion UpdateDocument41 pagesOtolaryngol - Head Neck Surg - 2016 - Rosenfeld - Clinical Practice Guideline Otitis Media With Effusion UpdateFatih AbdullahNo ratings yet
- 02 Review PDFDocument10 pages02 Review PDFDanan LaksetyaNo ratings yet
- American Academy of Family Physicians: Clinical Practice Guideline: Otitis Media With EffusionDocument64 pagesAmerican Academy of Family Physicians: Clinical Practice Guideline: Otitis Media With EffusionIndigo ViolettaNo ratings yet
- Sleep Disorders in Pediatric Dentistry: Clinical Guide on Diagnosis and ManagementFrom EverandSleep Disorders in Pediatric Dentistry: Clinical Guide on Diagnosis and ManagementEdmund LiemNo ratings yet
- Examining Interventions and Effectiveness of Outpatient Pediatric Feeding TherapyDocument1 pageExamining Interventions and Effectiveness of Outpatient Pediatric Feeding TherapyLauraNo ratings yet
- Development of An Assessment For Ideational Praxis: Teresa A. May-Benson, Sharon A. CermakDocument6 pagesDevelopment of An Assessment For Ideational Praxis: Teresa A. May-Benson, Sharon A. CermakNina SalinasNo ratings yet
- Dyspraxia's Impact on Play Skills in AutismDocument6 pagesDyspraxia's Impact on Play Skills in AutismLauraNo ratings yet
- Sensory Profile ToddlerDocument5 pagesSensory Profile ToddlerLauraNo ratings yet
- Evaluation of MealSense A Sensory Integration-Based Feeding Support Program For ParentsDocument7 pagesEvaluation of MealSense A Sensory Integration-Based Feeding Support Program For ParentsLauraNo ratings yet
- Effective Treatment For Pediatric Feeding Difficulties Multimodal Approach Compared To Sensory Integration InterventionDocument1 pageEffective Treatment For Pediatric Feeding Difficulties Multimodal Approach Compared To Sensory Integration InterventionLauraNo ratings yet
- Dietary Intake Outcomes of Feeding Interventions For Children With Autism Spectrum Disorder (ASD)Document1 pageDietary Intake Outcomes of Feeding Interventions For Children With Autism Spectrum Disorder (ASD)LauraNo ratings yet
- Reexamining Feeding Through RelationshipsDocument7 pagesReexamining Feeding Through RelationshipsLauraNo ratings yet
- Organizing Alerting Calming Activities For Kids FINALDocument5 pagesOrganizing Alerting Calming Activities For Kids FINALLauraNo ratings yet
- FineMotorChallenge MinutetoWinIt Activities PacketDocument11 pagesFineMotorChallenge MinutetoWinIt Activities PacketLauraNo ratings yet
- Early Feeding Behaviors in Preterm Infants and Their Relationships To NeurobehaviorDocument1 pageEarly Feeding Behaviors in Preterm Infants and Their Relationships To NeurobehaviorLauraNo ratings yet
- Prewriting SkillsDocument10 pagesPrewriting SkillsLauraNo ratings yet
- Effectiveness of Outpatient OT Interventions To Improve Motor Skills For Children With SomatodyspraxiaDocument1 pageEffectiveness of Outpatient OT Interventions To Improve Motor Skills For Children With SomatodyspraxiaLauraNo ratings yet
- Latino-American Mothers' Perspectives On Feeding Their Young Children A Qualitative StudyDocument11 pagesLatino-American Mothers' Perspectives On Feeding Their Young Children A Qualitative StudyLauraNo ratings yet
- Mixed-Methods Analysis of Parent Stress and Feeding Experiences For Children With ASDDocument1 pageMixed-Methods Analysis of Parent Stress and Feeding Experiences For Children With ASDLauraNo ratings yet
- Pilot Study To Measure Deficits in Proprioception in Children With SomatodyspraxiaDocument10 pagesPilot Study To Measure Deficits in Proprioception in Children With SomatodyspraxiaLauraNo ratings yet
- Effect of Classroom Modification On Attention and Engagement of Students With Autism or DyspraxiaDocument9 pagesEffect of Classroom Modification On Attention and Engagement of Students With Autism or DyspraxiaLauraNo ratings yet
- May-Benson CermakDocument7 pagesMay-Benson CermakLauraNo ratings yet
- Parent Education Class For Children With Feeding DifficultiesDocument1 pageParent Education Class For Children With Feeding DifficultiesLauraNo ratings yet
- The Relationship Between Visual-Perceptual Motor Abilities and Clumsiness in Children With and Without Learning DisabilitiesDocument5 pagesThe Relationship Between Visual-Perceptual Motor Abilities and Clumsiness in Children With and Without Learning DisabilitiesLauraNo ratings yet
- The Relationship Between Narrative Language Skills and Ideational Praxis in ChildrenDocument3 pagesThe Relationship Between Narrative Language Skills and Ideational Praxis in ChildrenLauraNo ratings yet
- EASI Praxis Tests Age Trends and Internal ConsistencyDocument7 pagesEASI Praxis Tests Age Trends and Internal ConsistencyLauraNo ratings yet
- Validity of The Occupational Performance Scale of The Sensory Processing Three Dimensions MeasureDocument10 pagesValidity of The Occupational Performance Scale of The Sensory Processing Three Dimensions MeasureLauraNo ratings yet
- Deficits in Proprioception Measured in Children With SomatodyspraxiaDocument2 pagesDeficits in Proprioception Measured in Children With SomatodyspraxiaLauraNo ratings yet
- Differentiating Types of Apraxia in Children with Learning DisabilitiesDocument8 pagesDifferentiating Types of Apraxia in Children with Learning DisabilitiesLauraNo ratings yet
- Sensory Integration Patterns and Social Participation in Children With AutismDocument8 pagesSensory Integration Patterns and Social Participation in Children With AutismLauraNo ratings yet
- NCP and Drug StudyDocument11 pagesNCP and Drug StudyTonio PagaoNo ratings yet
- DDR PrimeDocument4 pagesDDR PrimeNona AlyNo ratings yet
- Pedia Set B PRNDocument9 pagesPedia Set B PRNEdgar RebuyasNo ratings yet
- Case Study Cap 2016Document31 pagesCase Study Cap 2016NadeshikoNo ratings yet
- 7es Science Lesson Plan ExampleDocument9 pages7es Science Lesson Plan ExampleKing GarciaNo ratings yet
- NANDA Page 658Document5 pagesNANDA Page 658Ashley Gaton Alindogan100% (1)
- Geeky Medics DocumentationDocument3 pagesGeeky Medics DocumentationGus LionsNo ratings yet
- Mock Occupational English Test Speaking PneumoniaDocument1 pageMock Occupational English Test Speaking PneumoniamavisNo ratings yet
- MK Paeds BazookaDocument118 pagesMK Paeds BazookaChipasha Bwalya100% (1)
- Ards Case StudyDocument1 pageArds Case StudyLyons MacNo ratings yet
- Interstitial Lung DiseaseDocument26 pagesInterstitial Lung DiseaseEnimia ShyNo ratings yet
- Nclex Questions - Medical Surgical NursingDocument15 pagesNclex Questions - Medical Surgical NursingRegine Gozo100% (1)
- CHN FinalsDocument43 pagesCHN FinalsNHICOLE YAO PORCESONo ratings yet
- Qi Presentation VapDocument19 pagesQi Presentation Vapapi-383799988No ratings yet
- I. National Objectives For Health 2005 - 2010 Department of HealthDocument7 pagesI. National Objectives For Health 2005 - 2010 Department of Healthjonalyn badeNo ratings yet
- Diagnosa IcdDocument13 pagesDiagnosa IcdAnnisa Putri AbisekaNo ratings yet
- Random FactsDocument338 pagesRandom Factscyram81100% (1)
- Penatalaksanaan Petugas Terpapar COVID-19Document30 pagesPenatalaksanaan Petugas Terpapar COVID-19Taupick ArsyNo ratings yet
- Download A First Look At Communication Theory 11Th Edition Em Griffin full chapterDocument67 pagesDownload A First Look At Communication Theory 11Th Edition Em Griffin full chaptermary.martin668100% (6)
- Case Study Pneumonia PediaDocument13 pagesCase Study Pneumonia PediaAinurul FatehahNo ratings yet
- Makalah Big SputumDocument12 pagesMakalah Big SputumCherlina ika Firana puteriNo ratings yet
- NLE RDocument51 pagesNLE RmariaNo ratings yet
- A Case Study Pneumonia 2329 6879 1000242 PDFDocument4 pagesA Case Study Pneumonia 2329 6879 1000242 PDFAsma Yudhi EfendiNo ratings yet
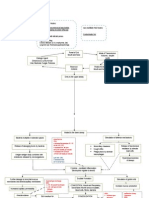
- Pneumonia PathodiagramDocument3 pagesPneumonia PathodiagramLester AbadNo ratings yet
- Drug StudyDocument12 pagesDrug Studyjoaqiun100% (1)
- 1 Revise MRCPDocument2 pages1 Revise MRCPDocSam048No ratings yet
- Impact of Medical Care Including Use of Anti Infec - 2020 - International JournDocument9 pagesImpact of Medical Care Including Use of Anti Infec - 2020 - International Journragod2No ratings yet
- Pneumonia (Fix)Document64 pagesPneumonia (Fix)Kornelis AribowoNo ratings yet