You might also like
- Ayushman BharatDocument28 pagesAyushman Bharatahffjda0% (1)
- AYushman Bharat AnalysisDocument12 pagesAYushman Bharat Analysisravi767457507No ratings yet
- The Indian Health Care System: A Complex Public-Private MixDocument9 pagesThe Indian Health Care System: A Complex Public-Private MixAaron Michelle DuvaliNo ratings yet
- Health Infrastructure in IndiaDocument34 pagesHealth Infrastructure in IndiamithraaNo ratings yet
- DATA ANALYSIS ManiDocument17 pagesDATA ANALYSIS ManiSyed AquibNo ratings yet
- Healthcare in IndiaDocument40 pagesHealthcare in Indiamanisha paikaray100% (1)
- Impact of Pradhan Mantri Jan Arogya Yojnaa On Indian EconomyDocument41 pagesImpact of Pradhan Mantri Jan Arogya Yojnaa On Indian EconomyyashNo ratings yet
- Ealth Nsurance IN Ndia: R M - 05PH2010Document6 pagesEalth Nsurance IN Ndia: R M - 05PH2010api-26832469No ratings yet
- A Comprehensive Analysis of Ayushman BharatDocument12 pagesA Comprehensive Analysis of Ayushman BharatMahika Gandhi100% (1)
- The Modicare Project CL PDPDocument5 pagesThe Modicare Project CL PDPDanish S MehtaNo ratings yet
- FICCI EY Report Healthcare ReportDocument72 pagesFICCI EY Report Healthcare Reportsh_niravNo ratings yet
- DES Final EssayDocument11 pagesDES Final EssaySumedha SaxenaNo ratings yet
- Health Insurance Coverage in India Insights for National Health Protection SchemeDocument21 pagesHealth Insurance Coverage in India Insights for National Health Protection Schemegarg.manav8No ratings yet
- Health Insurance Coverage in India Insights For National Health Protection SchemeDocument21 pagesHealth Insurance Coverage in India Insights For National Health Protection SchemeNeelaj MaityNo ratings yet
- Report On The High Healthcare Costs in IndiaDocument3 pagesReport On The High Healthcare Costs in IndiaSydkoNo ratings yet
- Rashtriya Swasthya Bima Yojana: Pioneering Public-Private Partnership in Health InsuranceDocument20 pagesRashtriya Swasthya Bima Yojana: Pioneering Public-Private Partnership in Health InsuranceSahaNo ratings yet
- India: Current State of HealthcareDocument15 pagesIndia: Current State of HealthcareYadav MannuNo ratings yet
- The Role of The Private Sector in Achieving Universal Healthcare in IndiaDocument7 pagesThe Role of The Private Sector in Achieving Universal Healthcare in IndiaEmerging Markets Health NetworkNo ratings yet
- Health Law ProjectDocument22 pagesHealth Law ProjectVarun MittalNo ratings yet
- Articles From General Knowledge Today: Rashtriya Swasthya Bima YojanaDocument2 pagesArticles From General Knowledge Today: Rashtriya Swasthya Bima YojanaSachinSharmaNo ratings yet
- HealthcareDocument10 pagesHealthcareTanish DhandNo ratings yet
- Equity in Hospital Services Utilisation in India PDFDocument7 pagesEquity in Hospital Services Utilisation in India PDFaditya_2kNo ratings yet
- Policy Brief on Ayushman Bharat's Impact and ShortcomingsDocument15 pagesPolicy Brief on Ayushman Bharat's Impact and ShortcomingsSujal TakNo ratings yet
- Challenge For UhcDocument3 pagesChallenge For UhcSatyanarayan MeenaNo ratings yet
- Healthcare in IndiaDocument91 pagesHealthcare in IndiaThanusha ThanushaNo ratings yet
- Man Environment Interaction of Naz BasinDocument28 pagesMan Environment Interaction of Naz BasinTp TpNo ratings yet
- 1 Ravi KiarnDocument14 pages1 Ravi KiarnMohammed Ahad UddinNo ratings yet
- Literature Review of Quality of Healthcare Services in IndiaDocument27 pagesLiterature Review of Quality of Healthcare Services in IndiaMunnangi NagendrareddyNo ratings yet
- Ayushman Bharat Yojana A Memorable Health InitiatiDocument2 pagesAyushman Bharat Yojana A Memorable Health InitiatiPiyush ChaturvediNo ratings yet
- Thailand's Three Main Health Insurance SchemesDocument42 pagesThailand's Three Main Health Insurance SchemesChampaka Prasad RanaNo ratings yet
- Prospects and issues in marketing health insurance in IndiaDocument7 pagesProspects and issues in marketing health insurance in IndiaManoj PareekNo ratings yet
- The Focus of Healthcare Is Increasingly Getting Skewed Towards TheDocument4 pagesThe Focus of Healthcare Is Increasingly Getting Skewed Towards TheNitish KumarNo ratings yet
- Vineeth Project NewDocument40 pagesVineeth Project NewFavas MuhammedNo ratings yet
- Ayushman BharatDocument3 pagesAyushman BharatSimran SpalNo ratings yet
- Chapter - 1 Nature, Scope, Objectives and Methodology of ResearchDocument18 pagesChapter - 1 Nature, Scope, Objectives and Methodology of ResearchJobin BabuNo ratings yet
- Chapter - 1 Nature, Scope, Objectives and Methodology of ResearchDocument18 pagesChapter - 1 Nature, Scope, Objectives and Methodology of ResearchMohammad MudasirNo ratings yet
- Chapter - 1 Nature, Scope, Objectives and Methodology of ResearchDocument18 pagesChapter - 1 Nature, Scope, Objectives and Methodology of ResearchJobin BabuNo ratings yet
- Chapter - 1 Nature, Scope, Objectives and Methodology of ResearchDocument18 pagesChapter - 1 Nature, Scope, Objectives and Methodology of ResearchJobin BabuNo ratings yet
- Comparative Study of Public and Private Health Services in Mumbai RegionDocument18 pagesComparative Study of Public and Private Health Services in Mumbai RegionJobin BabuNo ratings yet
- India HealthcareDocument16 pagesIndia HealthcareNeeraj SethiNo ratings yet
- ChisDocument34 pagesChisAnagha MaryNo ratings yet
- A Comparative Study On Patient Satisfaction Among Public and Private Hospitals in City of Pune, MaharashtraDocument8 pagesA Comparative Study On Patient Satisfaction Among Public and Private Hospitals in City of Pune, MaharashtraSaurav BhowmikNo ratings yet
- GCSR Nagaland - GTU ReportDocument10 pagesGCSR Nagaland - GTU ReportSatish J. MakwanaNo ratings yet
- Health Insurance in IndiaDocument93 pagesHealth Insurance in IndiaSaurabh NagwekarNo ratings yet
- wg11 HeasysDocument44 pageswg11 Heasysasdf789456123No ratings yet
- Healthcare in IndiaDocument2 pagesHealthcare in IndiaBrok GamingNo ratings yet
- Social Health Insurance in India Current ScenarioDocument22 pagesSocial Health Insurance in India Current ScenarioRohit MalviyaNo ratings yet
- Healthcare in IndiaDocument2 pagesHealthcare in IndiaKNishujiNo ratings yet
- Fixing India's Healthcare System - Carnegie Endowment For International PeaceDocument3 pagesFixing India's Healthcare System - Carnegie Endowment For International PeaceMohammad UzairNo ratings yet
- Health Care Status in IndiaDocument46 pagesHealth Care Status in Indialucky prajapatiNo ratings yet
- CIA 3 Health EconomicsDocument14 pagesCIA 3 Health EconomicsSujal TakNo ratings yet
- National Health Policy, 2017: Revealing Public Health ChicaneryDocument12 pagesNational Health Policy, 2017: Revealing Public Health ChicaneryRohan RegiNo ratings yet
- Ayushman Bharat Scheme Provides Healthcare CoverageDocument11 pagesAyushman Bharat Scheme Provides Healthcare CoverageAbhijit MundaleNo ratings yet
- Introduction To Healthcare System of IndiaDocument22 pagesIntroduction To Healthcare System of Indiakratika GaurNo ratings yet
- "It Is Health That Is Real Wealth and Not Pieces of Gold and Silver" Mahatma GandhiDocument8 pages"It Is Health That Is Real Wealth and Not Pieces of Gold and Silver" Mahatma GandhishivamNo ratings yet
- Evidence Based Field Work ReportDocument16 pagesEvidence Based Field Work ReportSuraj MauryaNo ratings yet
- Health Insurance in IndiaDocument11 pagesHealth Insurance in IndiaUpender DhullNo ratings yet
- Khyber Pakhtunkhwa Health Sector Review: Hospital CareFrom EverandKhyber Pakhtunkhwa Health Sector Review: Hospital CareNo ratings yet
- A Plan for a Single-Payer Health Care System: The Best Health Care in the WorldFrom EverandA Plan for a Single-Payer Health Care System: The Best Health Care in the WorldNo ratings yet
- HEALTHCARE SERVICE QUALITY AND PATIENT SATISFACTION IN OMANI PUBLIC HOSPITALS THROUGHOUT COVID-19 ERA: AN EMPIRICAL INVESTIGATIONFrom EverandHEALTHCARE SERVICE QUALITY AND PATIENT SATISFACTION IN OMANI PUBLIC HOSPITALS THROUGHOUT COVID-19 ERA: AN EMPIRICAL INVESTIGATIONNo ratings yet
- Name: Sport: Movement PrepDocument24 pagesName: Sport: Movement PrepS HNo ratings yet
- Predicting Natural Hazards PowerPointDocument29 pagesPredicting Natural Hazards PowerPointZarlene SierraNo ratings yet
- Sarah Fahy CV College PDFDocument4 pagesSarah Fahy CV College PDFapi-487352339No ratings yet
- Refrigeration and Air Conditioning Laboratory: Lab Session 3 Absorption Refrigeration Demonstrator 816 ObjectivesDocument10 pagesRefrigeration and Air Conditioning Laboratory: Lab Session 3 Absorption Refrigeration Demonstrator 816 Objectivesjhon milliNo ratings yet
- Broiled Salisbury SteaksDocument29 pagesBroiled Salisbury SteaksCei mendozaNo ratings yet
- M80 Oil Pump ManualDocument24 pagesM80 Oil Pump ManualElliot SmithNo ratings yet
- MYK Grout Card 2Document2 pagesMYK Grout Card 2Abdul Raheem SyedNo ratings yet
- Heat Transfer Surfaces Guide PDFDocument8 pagesHeat Transfer Surfaces Guide PDFJohan ConradieNo ratings yet
- NanocatalysisDocument9 pagesNanocatalysisNouran ElbadawiNo ratings yet
- BInggrisDocument19 pagesBInggrisanwar318No ratings yet
- 0210 Pop Labels BSDocument1 page0210 Pop Labels BSThe London Free PressNo ratings yet
- NSEA Solved Paper 2015Document30 pagesNSEA Solved Paper 2015vv12345670% (1)
- Introducion To Load Cells UtilcellDocument22 pagesIntroducion To Load Cells UtilcellRifi MohamedNo ratings yet
- Recommended Abma & Asme Boiler Water Limits Drum Operating Pressure (Psig) SteamDocument9 pagesRecommended Abma & Asme Boiler Water Limits Drum Operating Pressure (Psig) Steammaoc4vnNo ratings yet
- 2009 IECC Residential Code Requirements Apr 14 Draft InspectorsDocument4 pages2009 IECC Residential Code Requirements Apr 14 Draft Inspectorsbcap-oceanNo ratings yet
- Duconmix CRP 400Document2 pagesDuconmix CRP 400FounTech612No ratings yet
- Uganda National Urban ProfileDocument74 pagesUganda National Urban ProfileUnited Nations Human Settlements Programme (UN-HABITAT)No ratings yet
- RS9923 - Grade 12 Compulsory Subjects - Test Specification Chart and Model Questions - FinalDocument32 pagesRS9923 - Grade 12 Compulsory Subjects - Test Specification Chart and Model Questions - FinalPrince JaiswalNo ratings yet
- Sedimentation Tank Design NptelDocument7 pagesSedimentation Tank Design NptelNayan HalderNo ratings yet
- Animal Names in English and Telugu - 20170912 - 182216545Document17 pagesAnimal Names in English and Telugu - 20170912 - 182216545karimulla goraNo ratings yet
- Dyna Lift Flyer 500 FL 000010 enDocument20 pagesDyna Lift Flyer 500 FL 000010 enErdinc SenmanNo ratings yet
- Help to Buy ISA GuideDocument4 pagesHelp to Buy ISA GuidefsdesdsNo ratings yet
- Curriculum DesignDocument20 pagesCurriculum DesignRose Glaire Alaine TabraNo ratings yet
- Nikon Nivo C Series Instruction ManualDocument65 pagesNikon Nivo C Series Instruction ManualBambang Deriyanto100% (1)
- Argumentative EssayDocument5 pagesArgumentative Essayapi-538443988No ratings yet
- Work Immersion PortfolioDocument15 pagesWork Immersion PortfolioKaye Irish RosauroNo ratings yet
- Duarte Et Al - Resin CementsDocument28 pagesDuarte Et Al - Resin Cementsjfrascarolo100% (4)
- Hyperfunctional Voice DisordersDocument11 pagesHyperfunctional Voice DisordersJam PNo ratings yet
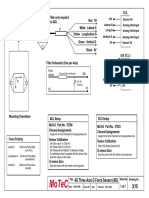
- Filter and wiring schematic for 3-axis ADL G-force sensorDocument1 pageFilter and wiring schematic for 3-axis ADL G-force sensorJuan Ramón Pérez LorenzoNo ratings yet
- CS Risk and Crisis Management FinalDocument62 pagesCS Risk and Crisis Management FinaldangermanNo ratings yet