You might also like
- 00130478-202105000-00006 Serial Neurologic Assessment in Pediatrics (SNAP) : A New Tool For Bedside Neurologic Assessment of Critically Ill ChildrenDocument13 pages00130478-202105000-00006 Serial Neurologic Assessment in Pediatrics (SNAP) : A New Tool For Bedside Neurologic Assessment of Critically Ill ChildrenYo MeNo ratings yet
- Nursing TheoriesDocument9 pagesNursing TheoriesMichelleneChenTadleNo ratings yet
- Cognitive Effects of Peg-IFNalpha/RBV Treatment in Hepatitis C PatientsDocument1 pageCognitive Effects of Peg-IFNalpha/RBV Treatment in Hepatitis C PatientstatypatryNo ratings yet
- Metabolic Abnormalities Reveal Chronic Fatigue Syndrome BiologyDocument9 pagesMetabolic Abnormalities Reveal Chronic Fatigue Syndrome BiologyM. A. GARCÍANo ratings yet
- MainDocument10 pagesMainBhandariNo ratings yet
- Brown 2016Document13 pagesBrown 2016wedawisnawaNo ratings yet
- Nunez Fernandez 2022 Validation of The Norma Latina NeurDocument15 pagesNunez Fernandez 2022 Validation of The Norma Latina NeurMelissa DiazNo ratings yet
- Advance Care Plan and Factors Related To Disease Progression in Patients With Spinocerebellar Ataxia Type 1: A Cross-Sectional Study in ThailandDocument6 pagesAdvance Care Plan and Factors Related To Disease Progression in Patients With Spinocerebellar Ataxia Type 1: A Cross-Sectional Study in ThailandJefe de Escuela PsicologiaNo ratings yet
- Franca 2020 AtaxiaDocument6 pagesFranca 2020 AtaxiainervavsNo ratings yet
- Bloque - 4 - DCB CriteriosDocument7 pagesBloque - 4 - DCB CriteriosMacarena RodriguezNo ratings yet
- Safety Tolerability and Efficacy of pbt2 in Huntingtons Disease 2015Document9 pagesSafety Tolerability and Efficacy of pbt2 in Huntingtons Disease 2015Eileen MoralesNo ratings yet
- 2012-European Journal of Neurology IMPRIMIR PAGINA 141Document368 pages2012-European Journal of Neurology IMPRIMIR PAGINA 141Francisco A. Villegas-LópezNo ratings yet
- 878 Saturday, 17 June 2017: Scientific AbstractsDocument1 page878 Saturday, 17 June 2017: Scientific AbstractsDavid Gimenez RomeroNo ratings yet
- Longterm Safety and Effectiveness of Lurasidone in Schizophrenia A 22month Openlabel Extension StudyDocument10 pagesLongterm Safety and Effectiveness of Lurasidone in Schizophrenia A 22month Openlabel Extension Studyromany hosnyNo ratings yet
- Comparing In-House and Glasgow Coma Scales for Non-Traumatic Altered StatesDocument16 pagesComparing In-House and Glasgow Coma Scales for Non-Traumatic Altered StatesMegha JainNo ratings yet
- Nutrients 14 03959Document15 pagesNutrients 14 03959CrisNo ratings yet
- Score Predictivo NMDA 2018Document10 pagesScore Predictivo NMDA 2018Pablo Sebastián SaezNo ratings yet
- 2-F-Fluoro-2-Deoxyglucose Positron Emission Tomography in DeliriumDocument12 pages2-F-Fluoro-2-Deoxyglucose Positron Emission Tomography in DeliriumIin Rodiatul Wardiah HarahapNo ratings yet
- Bilingualism As A Protection Against The Onset of Symptoms of DementiaDocument6 pagesBilingualism As A Protection Against The Onset of Symptoms of DementiaSonier KaeceipzNo ratings yet
- Validación en Mexico 2022Document8 pagesValidación en Mexico 2022juanpaNo ratings yet
- oooDocument10 pagesoooaner cristobal alonso alonsoNo ratings yet
- Ana 24309Document14 pagesAna 24309cah bagusNo ratings yet
- 2021 09 24 21264020v1 FullDocument25 pages2021 09 24 21264020v1 FullElfina NataliaNo ratings yet
- Jurnal 3Document6 pagesJurnal 3rifahNo ratings yet
- Journalof Natural RemediesDocument10 pagesJournalof Natural RemediesAndreia TorresNo ratings yet
- Abstrak GabungDocument3 pagesAbstrak GabunganastasiagmNo ratings yet
- 1 s2.0 S0890856714004079 MainDocument10 pages1 s2.0 S0890856714004079 MainPar DoNo ratings yet
- The Spanish Version of The Coma Recovery Scale-Revised: Events On A Correct TimelineDocument19 pagesThe Spanish Version of The Coma Recovery Scale-Revised: Events On A Correct TimelineGaby ChocobarNo ratings yet
- Botulinum Toxin A For Upper Limb SpasticityDocument3 pagesBotulinum Toxin A For Upper Limb SpasticityTerrence ChanNo ratings yet
- Validation of The Amyotrophic Lateral Sclerosis Assessment Questionnaire (ALSAQ-40) Scale in The Portuguese LanguageDocument4 pagesValidation of The Amyotrophic Lateral Sclerosis Assessment Questionnaire (ALSAQ-40) Scale in The Portuguese LanguageMCPF1No ratings yet
- Escala de Recuperación Del ComaDocument18 pagesEscala de Recuperación Del ComaFrancisco Aguilera GalloNo ratings yet
- Stem Cells Therapy in Cerebral Palsy: A Systematic ReviewDocument7 pagesStem Cells Therapy in Cerebral Palsy: A Systematic Reviewallyssa rahmadittaNo ratings yet
- 154-The Frequency and Aetiology of Repeated Kidney Injury Episodes Determine The Degree of Renal DamageDocument2 pages154-The Frequency and Aetiology of Repeated Kidney Injury Episodes Determine The Degree of Renal DamageCarlos Martinez SalgadoNo ratings yet
- Bartlett 2020Document9 pagesBartlett 2020Erick SolisNo ratings yet
- Subacute Sclerosing Panencephalitis A Clinical and Pathological Study - 101 108Document7 pagesSubacute Sclerosing Panencephalitis A Clinical and Pathological Study - 101 108Bhanu PratapNo ratings yet
- Glutathione Precursor N-Acetyl-cysteine Modulates EEG Synchronization in Schizophrenia PatientsDocument9 pagesGlutathione Precursor N-Acetyl-cysteine Modulates EEG Synchronization in Schizophrenia PatientsArturoNo ratings yet
- Practice Parameters: Assessment and Management of Patients in The Persistent Vegetative State (Summary Statement)Document7 pagesPractice Parameters: Assessment and Management of Patients in The Persistent Vegetative State (Summary Statement)mr.anggaardiantoNo ratings yet
- The Ketogenic Diet As A Non Pharmacological Treatment For HIV Associated Neurocognitive Disorder A Descriptive AnalysisDocument5 pagesThe Ketogenic Diet As A Non Pharmacological Treatment For HIV Associated Neurocognitive Disorder A Descriptive AnalysisPaul HartingNo ratings yet
- A Comprehensive Review of Adult EnuresisDocument13 pagesA Comprehensive Review of Adult EnuresisAli HusseinNo ratings yet
- Etanercept in Alzheimer Disease: A Randomized, Placebo-Controlled, Double-Blind, Phase 2 TrialDocument8 pagesEtanercept in Alzheimer Disease: A Randomized, Placebo-Controlled, Double-Blind, Phase 2 TrialGiuseppe AcanforaNo ratings yet
- A Brief Cognitive Assessment Tool For SchizophreniaDocument8 pagesA Brief Cognitive Assessment Tool For SchizophreniaRatriningdyah DewiNo ratings yet
- Acm 2014 5390 AbstractDocument2 pagesAcm 2014 5390 Abstractharshadpardeshi45No ratings yet
- Neurourology and Urodynamics - 2022 - Kwon - Continuous Administration of Mirabegron Has Advantages in Inhibition ofDocument9 pagesNeurourology and Urodynamics - 2022 - Kwon - Continuous Administration of Mirabegron Has Advantages in Inhibition ofkadioglu20No ratings yet
- Marigold Lutein and Zeaxanthin 1Document7 pagesMarigold Lutein and Zeaxanthin 1dmNo ratings yet
- Benefits of Cognitive-Motor Intervention in MCI and Mild To Moderate Alzheimer DiseaseDocument6 pagesBenefits of Cognitive-Motor Intervention in MCI and Mild To Moderate Alzheimer DiseaseLaura Alvarez AbenzaNo ratings yet
- 10.1007@s12311 020 01195 7Document10 pages10.1007@s12311 020 01195 7xiomara velasquezNo ratings yet
- 250 Successful Management of Ankylosing SpondylitiDocument1 page250 Successful Management of Ankylosing SpondylitiAananda Raaj V MNo ratings yet
- Analysis_of_the_effectiveness_of_the_intDocument1 pageAnalysis_of_the_effectiveness_of_the_intslyvesterNo ratings yet
- Results of Gamma Knife Anterior Capsulotomy For Refractory Obsessive-Compulsive Disorder: Results in A Series of 10 Consecutive PatientsDocument8 pagesResults of Gamma Knife Anterior Capsulotomy For Refractory Obsessive-Compulsive Disorder: Results in A Series of 10 Consecutive PatientsManuela Martín-Bejarano GarcíaNo ratings yet
- NLR Bells PalsyDocument4 pagesNLR Bells PalsyIskandar HasanNo ratings yet
- Deep Brain Stimulation PDFDocument11 pagesDeep Brain Stimulation PDFTeodora FeliciaNo ratings yet
- A-Comparative-Analysis-of-Nutritional-Assessment-UDocument7 pagesA-Comparative-Analysis-of-Nutritional-Assessment-Uranjani093No ratings yet
- Best Autism Treatment in ChennaiDocument32 pagesBest Autism Treatment in ChennaiNP KarthikeyenNo ratings yet
- Pico P1Document3 pagesPico P1Siti Ayu Nur'afifahNo ratings yet
- Nicotine Treatment of Mild Cognitive Impairment - PMCDocument15 pagesNicotine Treatment of Mild Cognitive Impairment - PMCDoug HaynesNo ratings yet
- Disfunción Ejecutiva en La Enfermedad de HuntingtonDocument7 pagesDisfunción Ejecutiva en La Enfermedad de HuntingtonKaren TolorzaNo ratings yet
- Cell Based Therapeutic Strategies For Treatment Of.6Document10 pagesCell Based Therapeutic Strategies For Treatment Of.6Tamara MuñozNo ratings yet
- Biomarkers Distinguish Between Sepsis-Associated Encephalopathy and DeliriumDocument5 pagesBiomarkers Distinguish Between Sepsis-Associated Encephalopathy and DeliriumCristiane TomasiNo ratings yet
- Advantage of Modified MRI Protocol For HDocument148 pagesAdvantage of Modified MRI Protocol For HasasakopNo ratings yet
- CLN 66 06 991 PDFDocument5 pagesCLN 66 06 991 PDFyenny handayani sihiteNo ratings yet
- Autism Spectrum Disorder: Bioregenerative Medicine With Stem Cell TherapyFrom EverandAutism Spectrum Disorder: Bioregenerative Medicine With Stem Cell TherapyNo ratings yet
- 2011 02 Huijben Spie Why Every Urea Plant Needs A Continuous NC Meter PDFDocument9 pages2011 02 Huijben Spie Why Every Urea Plant Needs A Continuous NC Meter PDFfawadintNo ratings yet
- Global Resort List by Country (38 charactersDocument51 pagesGlobal Resort List by Country (38 charactersMaulik ShahNo ratings yet
- Mechanical Design of Turine EginesDocument51 pagesMechanical Design of Turine EginessriniNo ratings yet
- Mathematical Structures of The UniverseDocument228 pagesMathematical Structures of The UniverseMaki MajomNo ratings yet
- El Anatsui - TransformationsDocument15 pagesEl Anatsui - TransformationsReece BriceNo ratings yet
- Air Sentry - Energy Statement App 3 Dessicant and Filters PDFDocument20 pagesAir Sentry - Energy Statement App 3 Dessicant and Filters PDFEsteban Fernando Meza IbacetaNo ratings yet
- Algebra 1 FINAL EXAM REVIEW 2Document2 pagesAlgebra 1 FINAL EXAM REVIEW 2Makala DarwoodNo ratings yet
- SilverDocument16 pagesSilversharma_shruti0% (1)
- Guía de Instalación y Programación: Sistema de Seguridad de 32 ZonasDocument68 pagesGuía de Instalación y Programación: Sistema de Seguridad de 32 ZonasfernanfivNo ratings yet
- Science: Pure Substances Vs MixturesDocument33 pagesScience: Pure Substances Vs MixturesElle Ma Rie100% (1)
- Stabil Drill Roller ReamersDocument2 pagesStabil Drill Roller ReamersIMEDHAMMOUDANo ratings yet
- What Is The Kingdom of GodDocument10 pagesWhat Is The Kingdom of GodSunil ChelladuraiNo ratings yet
- Essay Writing-PTEDocument13 pagesEssay Writing-PTEAnita GajjarNo ratings yet
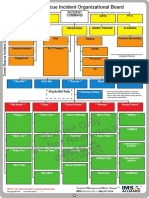
- Sample Only Do Not Reproduce: Trench Rescue Incident Organizational BoardDocument1 pageSample Only Do Not Reproduce: Trench Rescue Incident Organizational BoardLuis Diaz CerdanNo ratings yet
- White Lies - Core RulebookDocument136 pagesWhite Lies - Core RulebookThiago AlmeidaNo ratings yet
- LEEA-036 (B) - Academy ITS Practical Training Courses Jan - June 2020 Version 1 October 2019Document18 pagesLEEA-036 (B) - Academy ITS Practical Training Courses Jan - June 2020 Version 1 October 2019kaito kurabaNo ratings yet
- 60d068822a861e19f4179ec9 - 11. Consensus - Local Cerberus - CompressedDocument1 page60d068822a861e19f4179ec9 - 11. Consensus - Local Cerberus - Compressedhombre pocilgaNo ratings yet
- Example of Gcse Science CourseworkDocument7 pagesExample of Gcse Science Courseworkbcrbcw6a100% (2)
- 3rd Periodic Test in English4Document7 pages3rd Periodic Test in English4Santa Dela Cruz Naluz100% (1)
- Module 2 Chem 1Document25 pagesModule 2 Chem 1melissa cabreraNo ratings yet
- Audit Keselamatan Jalan Pada Jalan Yogyakarta-Purworejo KM 35-40, Kulon Progo, YogyakartaDocument10 pagesAudit Keselamatan Jalan Pada Jalan Yogyakarta-Purworejo KM 35-40, Kulon Progo, YogyakartaSawaluddin SawalNo ratings yet
- LUKAS Product Information-2Document2 pagesLUKAS Product Information-2Flavian ZfmNo ratings yet
- Jean NouvelDocument1 pageJean Nouvelc.sioson.540553No ratings yet
- Separation and Purification TechnologyDocument10 pagesSeparation and Purification TechnologyPedro Henrique MagachoNo ratings yet
- Magellans of The Sky - Prologue - Summer 2010Document12 pagesMagellans of The Sky - Prologue - Summer 2010Prologue MagazineNo ratings yet
- Instapdf - in Bangalore Tourist Places List 674Document31 pagesInstapdf - in Bangalore Tourist Places List 674R K PathamNo ratings yet
- Lab ReportDocument9 pagesLab ReportQi Yi TanNo ratings yet
- Design of Temporary Floating Road for Construction SiteDocument6 pagesDesign of Temporary Floating Road for Construction SiteAnonymous hRWwL7pZnCNo ratings yet
- 9th Mole Concept and Problems Based On PDFDocument2 pages9th Mole Concept and Problems Based On PDFMintu KhanNo ratings yet