You might also like
- FDARDocument33 pagesFDARRaquel M. Mendoza100% (7)
- Dental Vto MBTDocument10 pagesDental Vto MBTGabriela Castillo83% (6)
- Nursing InductionDocument114 pagesNursing InductionMichael Long92% (26)
- Charting and Documentation NotesDocument4 pagesCharting and Documentation NotesCyriel DicoNo ratings yet
- Assessment Needs Nursing Diagnos IS Goal/Obj Ective Intervention Rationale EvaluationDocument10 pagesAssessment Needs Nursing Diagnos IS Goal/Obj Ective Intervention Rationale EvaluationApol Pen67% (3)
- Eclampsia NCPDocument2 pagesEclampsia NCPIvan Liquiran Avenado100% (2)
- Focus ChartingDocument5 pagesFocus ChartingAnn GelNo ratings yet
- NURSING CARE PLAN For Nsg. Research Betty NeumannDocument9 pagesNURSING CARE PLAN For Nsg. Research Betty NeumannFlor SabaysabayNo ratings yet
- What Is FOCUS CHARTINGDocument38 pagesWhat Is FOCUS CHARTINGSwen Digdigan-Ege100% (2)
- Soap ChartingDocument31 pagesSoap ChartingterefagcanganNo ratings yet
- NCP Acute PainDocument3 pagesNCP Acute PainSatchiko Riko SakuraNo ratings yet
- Respiratory Care Review: An Intense Look at Respiratory Care Through Case StudiesFrom EverandRespiratory Care Review: An Intense Look at Respiratory Care Through Case StudiesNo ratings yet
- Complications of Major SurgeryDocument24 pagesComplications of Major SurgerySoyebo Alegría OluseyeNo ratings yet
- Lyrica Generic vs Brand Name GuideDocument3 pagesLyrica Generic vs Brand Name GuideRoseben Somido100% (1)
- Which It Is A Process Whereby Pancreatic Enzymes Destroy Its Own Tissue Leading ToDocument8 pagesWhich It Is A Process Whereby Pancreatic Enzymes Destroy Its Own Tissue Leading ToAriane-Gay Cristobal DuranNo ratings yet
- FDAR ChartingDocument50 pagesFDAR ChartingNathaniel PulidoNo ratings yet
- I PassDocument43 pagesI PassAnmol shresthaNo ratings yet
- Duty Activity: Lyceum of The Philippines University College of NursingDocument7 pagesDuty Activity: Lyceum of The Philippines University College of NursingCyrille Anne MongeNo ratings yet
- Focus Charting 2Document65 pagesFocus Charting 2Ella Caro100% (1)
- Fdar Charting - Imh-1Document34 pagesFdar Charting - Imh-1Rekkusu MakeinuNo ratings yet
- CS NCPDocument3 pagesCS NCPAllan VillanuevaNo ratings yet
- NCPDocument1 pageNCPAlynna ValbuenaNo ratings yet
- NCP FinalDocument18 pagesNCP FinalJessica Medina100% (1)
- Date/ Time Cues Need Nursing Diagnosis Patient Outcome Planning of Interventions Imple Ment Ation EvaluationDocument4 pagesDate/ Time Cues Need Nursing Diagnosis Patient Outcome Planning of Interventions Imple Ment Ation EvaluationVianah Eve EscobidoNo ratings yet
- Nursing ProcessDocument40 pagesNursing ProcessRishiel Dimple BalonesNo ratings yet
- Problem-Oriented Charting SOPIE FormatDocument27 pagesProblem-Oriented Charting SOPIE Formatkyuss2No ratings yet
- NCPDocument9 pagesNCPLeolene Grace BautistaNo ratings yet
- Assessment Nursing Diagnosis Planning Nursing Intervention Rationale Evaluation IndependentDocument4 pagesAssessment Nursing Diagnosis Planning Nursing Intervention Rationale Evaluation IndependentJoseph Rodney de LeonNo ratings yet
- Focus Charting 2Document69 pagesFocus Charting 2Ella Caro100% (2)
- Focus ChartingDocument4 pagesFocus ChartingTenIs ForMeNo ratings yet
- NCPDocument17 pagesNCPShayne Jessemae AlmarioNo ratings yet
- Nursing Care PlanDocument9 pagesNursing Care PlanjmichaelaNo ratings yet
- NCPDocument4 pagesNCPHannah LopezNo ratings yet
- And Release of Pancreatic Enzyme: Which It Is A Process Whereby Pancreatic Enzymes Destroy Its Own Tissue Leading ToDocument15 pagesAnd Release of Pancreatic Enzyme: Which It Is A Process Whereby Pancreatic Enzymes Destroy Its Own Tissue Leading ToAriane-Gay Cristobal DuranNo ratings yet
- FDARDocument41 pagesFDARJojo Justo100% (2)
- Case Study 2Document19 pagesCase Study 2Sumit Singh100% (1)
- Answer Script Part B Mental Health Mid170014Document6 pagesAnswer Script Part B Mental Health Mid170014knj210110318No ratings yet
- Measuring Intake and OutputDocument24 pagesMeasuring Intake and Outputmftaganas83% (6)
- AOA Survival Guide To The 2nd YearDocument18 pagesAOA Survival Guide To The 2nd Yearmediquest100% (1)
- Hospital Clinical Week Three AssignmentDocument4 pagesHospital Clinical Week Three Assignmentapi-721737905No ratings yet
- Maricotwse 6Document3 pagesMaricotwse 6api-316415750No ratings yet
- The SOAP Note FormatDocument8 pagesThe SOAP Note Formatimeldafitri100% (1)
- Focus ChartingDocument23 pagesFocus ChartingJaffy Espiritu100% (3)
- Enrichment Class On DocumentationDocument20 pagesEnrichment Class On Documentationronnelgalang.rgNo ratings yet
- Nursing Care Plan for Respiratory IssuesDocument10 pagesNursing Care Plan for Respiratory IssuesMykel Jake VasquezNo ratings yet
- FINAL OSSAM-ICU PrestudyDocument36 pagesFINAL OSSAM-ICU PrestudyHannah DuyagNo ratings yet
- CHARTING BASICS GUIDEDocument11 pagesCHARTING BASICS GUIDEfarahdlc100% (1)
- Nursing Management of CVA and NIDDMDocument12 pagesNursing Management of CVA and NIDDMKaloy KamaoNo ratings yet
- Wse Week5Document4 pagesWse Week5api-302336744No ratings yet
- Revised Medicine Admit OrdersDocument2 pagesRevised Medicine Admit OrdersJamie AsheNo ratings yet
- wk4 Weekly Self Eval KmiuraDocument3 pageswk4 Weekly Self Eval Kmiuraapi-295640482No ratings yet
- NCP 28Document9 pagesNCP 28Leanne Joie Lozano100% (1)
- Documentation ExamplesDocument5 pagesDocumentation ExamplesErika HarveryNo ratings yet
- Final NCPDocument5 pagesFinal NCPAce VirtusioNo ratings yet
- Managing Acute Renal PainDocument22 pagesManaging Acute Renal PainMaricris S. Sampang100% (1)
- Reflective Theories Writing AssignmentDocument7 pagesReflective Theories Writing Assignmentapi-582889983No ratings yet
- Scolio, Heart FailureDocument12 pagesScolio, Heart FailureArjay AvesNo ratings yet
- Nursing Care Plan: Date/ Time Assessment Nursing Diagnosis Planning Intervention Evaluatio NDocument2 pagesNursing Care Plan: Date/ Time Assessment Nursing Diagnosis Planning Intervention Evaluatio NnananaNo ratings yet
- Heart of the Field "Refresher & Nha Certification Quick Notes"From EverandHeart of the Field "Refresher & Nha Certification Quick Notes"No ratings yet
- Nursing Study Guide: Your Nursing Assistant To Do Well In SchoolFrom EverandNursing Study Guide: Your Nursing Assistant To Do Well In SchoolRating: 3 out of 5 stars3/5 (2)
- Nurse As A EducatorDocument11 pagesNurse As A EducatorAlyssa EspineliNo ratings yet
- Nurse ManagerDocument8 pagesNurse ManagerAlyssa EspineliNo ratings yet
- Nurse As A EducatorDocument11 pagesNurse As A EducatorAlyssa EspineliNo ratings yet
- Group 1 Subgroup 2 - NCS - GerdDocument121 pagesGroup 1 Subgroup 2 - NCS - GerdAlyssa EspineliNo ratings yet
- PSEQ1Document11 pagesPSEQ1Vane GANo ratings yet
- Differentiation of Pityriasis Rubra Pilaris From Plaque Psoriasis by DermosDocument4 pagesDifferentiation of Pityriasis Rubra Pilaris From Plaque Psoriasis by DermoscharoiteNo ratings yet
- Caesarean SectionDocument73 pagesCaesarean SectionBhattarai Shrinkhala100% (2)
- Fertility Patients Under COVID-19: Attitudes, Perceptions and Psychological ReactionsDocument10 pagesFertility Patients Under COVID-19: Attitudes, Perceptions and Psychological ReactionsMirjana14No ratings yet
- Eye Essentials Diabetes and The Eye PDFDocument2 pagesEye Essentials Diabetes and The Eye PDFMicheleNo ratings yet
- Intestinal Malrotation in Neonates With Nonbilious Emesis: Perinatal/Neonatal Case PresentationDocument3 pagesIntestinal Malrotation in Neonates With Nonbilious Emesis: Perinatal/Neonatal Case PresentationSaurav SultaniaNo ratings yet
- Amy 1Document26 pagesAmy 1cynthia amaraNo ratings yet
- Current Views On Treatment of Vertigo and Dizziness (JURDING)Document22 pagesCurrent Views On Treatment of Vertigo and Dizziness (JURDING)arifNo ratings yet
- Epistaxis Diagnosis & TreatmentDocument3 pagesEpistaxis Diagnosis & TreatmentDaisy Haryono0% (1)
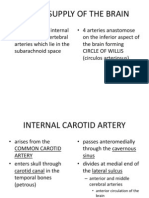
- Blood Supply of The BrainDocument11 pagesBlood Supply of The Brainneleh grayNo ratings yet
- Daftar Pustaka DaniDocument3 pagesDaftar Pustaka Danidokter linggauNo ratings yet
- Nexgen Legacy Lps Flex Knee BrochureDocument8 pagesNexgen Legacy Lps Flex Knee BrochureKamelBelkhirNo ratings yet
- Vet Repr UltrasDocument255 pagesVet Repr UltrasClaudia Alejandra Ramirez100% (1)
- Manual Periodontal Instrumentation Bailey1Document109 pagesManual Periodontal Instrumentation Bailey1velangniNo ratings yet
- Rizal Travel HistoryDocument4 pagesRizal Travel HistoryLeslie LinggodenNo ratings yet
- Organizing Neonatal CareDocument17 pagesOrganizing Neonatal CareManisha ThakurNo ratings yet
- Overview of Postpartum Hemorrhage - UpToDateDocument48 pagesOverview of Postpartum Hemorrhage - UpToDatewendy100% (1)
- $RQMTW24Document1 page$RQMTW24akxerox47No ratings yet
- Fracture FemurDocument28 pagesFracture FemurKulsoom ShahNo ratings yet
- Improving Breast Cancer Surgery Classification and Quadrant AtlasDocument17 pagesImproving Breast Cancer Surgery Classification and Quadrant Atlaskomlanihou_890233161No ratings yet
- Antibiotic Prophylaxis in Gastrointestinal System EndosDocument6 pagesAntibiotic Prophylaxis in Gastrointestinal System EndosAceNo ratings yet
- Thy 2015 0020 PDFDocument271 pagesThy 2015 0020 PDFMade RusmanaNo ratings yet
- Anesthesia Considerations for Microlaryngoscopy and Direct LaryngoscopyDocument6 pagesAnesthesia Considerations for Microlaryngoscopy and Direct LaryngoscopyRubén Darío HerediaNo ratings yet
- Regulasi CA, MG and PO4Document16 pagesRegulasi CA, MG and PO4siskaNo ratings yet
- 13 Districts Recognized Hospitals List PDFDocument86 pages13 Districts Recognized Hospitals List PDFseetha ramNo ratings yet
- Establishing An Anatomic Pathology Laboratory at Cleveland Clinic Abu DhabiDocument11 pagesEstablishing An Anatomic Pathology Laboratory at Cleveland Clinic Abu DhabiRafat ElshemiNo ratings yet
- Prosthodontics Book ListDocument3 pagesProsthodontics Book ListDentist Here100% (1)