You might also like
- Ndizeye 2018Document8 pagesNdizeye 2018Ajup SafarudinNo ratings yet
- Clinical Protection Handbook: for Healthcare Workers against COVID-19From EverandClinical Protection Handbook: for Healthcare Workers against COVID-19No ratings yet
- PPP Experience IndiaDocument37 pagesPPP Experience IndiaRajnish Ranjan PrasadNo ratings yet
- Clinical Decision Support System: Fundamentals and ApplicationsFrom EverandClinical Decision Support System: Fundamentals and ApplicationsNo ratings yet
- Application of Artificial Intelligence in Community-Based Primary Health Care - Systematic Scoping Review and Critical Appraisal - PMCDocument32 pagesApplication of Artificial Intelligence in Community-Based Primary Health Care - Systematic Scoping Review and Critical Appraisal - PMCPAULA REGINA TAVARES VIEIRANo ratings yet
- MedicinesDocument15 pagesMedicinesjuddy avottNo ratings yet
- Infection KontrolDocument48 pagesInfection Kontrolrini purwantiNo ratings yet
- Implementation of Smart Triage Combined With A QuaDocument21 pagesImplementation of Smart Triage Combined With A QuaadivwadhwaNo ratings yet
- Guide Lines in Surgical Quality ServiceDocument23 pagesGuide Lines in Surgical Quality ServiceAddis YeshitlaNo ratings yet
- Mukudu Et AlDocument10 pagesMukudu Et AlHillary MukuduNo ratings yet
- A Simple Remote Nutritional Screening Tool and PraDocument5 pagesA Simple Remote Nutritional Screening Tool and PraFERNANDA MAGDALENA BASTIAS GONZALEZNo ratings yet
- Jurnal Keselamatan PasienDocument9 pagesJurnal Keselamatan PasienJono ParmiNo ratings yet
- WHO CDS HIV 19.6 EngDocument20 pagesWHO CDS HIV 19.6 EngTauseef ShahidiNo ratings yet
- The Status Quo On Existing Routine Health InformatDocument15 pagesThe Status Quo On Existing Routine Health InformatJaweria KhanNo ratings yet
- Eliminating CAUTIDocument28 pagesEliminating CAUTIWardah Fauziah El SofwanNo ratings yet
- Y. AL HashmiDocument11 pagesY. AL HashmiAzam alausyNo ratings yet
- Oms Lista de Exames Essenciais 2018Document35 pagesOms Lista de Exames Essenciais 2018João LuccasNo ratings yet
- The Satisfactionof Patients On Maintenance Hemodialysis Concerning The Provided Nursing Care in Hemodialysis UnitsDocument11 pagesThe Satisfactionof Patients On Maintenance Hemodialysis Concerning The Provided Nursing Care in Hemodialysis Unitsbe a doctor for you Medical studentNo ratings yet
- Fpubh 10 879410Document7 pagesFpubh 10 879410Jaime Misael JalifeNo ratings yet
- SG Website ExampleDocument21 pagesSG Website ExampleishwaryaNo ratings yet
- GHC - TOR IMO COVID VaccinesDocument4 pagesGHC - TOR IMO COVID VaccinesDan JosephNo ratings yet
- National Urban Health MissionDocument30 pagesNational Urban Health MissiondeissuzaNo ratings yet
- Minimizing Population Health Loss in Times of Scarce Surgical Capacity During The Coronavirus Disease 2019 Crisis and Beyond: A Modeling StudyDocument10 pagesMinimizing Population Health Loss in Times of Scarce Surgical Capacity During The Coronavirus Disease 2019 Crisis and Beyond: A Modeling StudyAriani SukmadiwantiNo ratings yet
- Adherence of Physicians Practice Tonational Ministry of Health (Moh) Urgent Care Guideline in Eastern Region, Saudi ArabiaDocument9 pagesAdherence of Physicians Practice Tonational Ministry of Health (Moh) Urgent Care Guideline in Eastern Region, Saudi ArabiaIJAR JOURNALNo ratings yet
- Adherence of Physicians Practice Tonational Ministry of Health (Moh) Urgent Care Guideline in Eastern Region, Saudi ArabiaDocument9 pagesAdherence of Physicians Practice Tonational Ministry of Health (Moh) Urgent Care Guideline in Eastern Region, Saudi ArabiaIJAR JOURNALNo ratings yet
- Mentorship On Malaria Microscopy Diagnostic ServicDocument16 pagesMentorship On Malaria Microscopy Diagnostic Servicabiyot jemberNo ratings yet
- Egypt: Health Sector ReformDocument16 pagesEgypt: Health Sector Reformdevon2610No ratings yet
- Ket ProposalDocument37 pagesKet ProposalEneyew BirhanNo ratings yet
- WHO - MBHSS - Health System Strengthening PDFDocument110 pagesWHO - MBHSS - Health System Strengthening PDFRainer Danny Poluan MamahitNo ratings yet
- Slides For Hand Hygiene CoordinatorDocument138 pagesSlides For Hand Hygiene CoordinatorPaola Alcal� MatusNo ratings yet
- Toolkit Multisectoral Action Plan For Noncommunicable DiseasesDocument22 pagesToolkit Multisectoral Action Plan For Noncommunicable DiseasesabarmasNo ratings yet
- Indian Public Health Standard IIDocument19 pagesIndian Public Health Standard IIKailash NagarNo ratings yet
- Capstone ProjectDocument16 pagesCapstone Projectapi-549064749No ratings yet
- 411 1828 1 PB PDFDocument5 pages411 1828 1 PB PDFednihsNo ratings yet
- Consultorios Médicos en Farmacias PrivadasDocument12 pagesConsultorios Médicos en Farmacias PrivadasAristegui NoticiasNo ratings yet
- Principles Based Medical Informatics For Success NTDocument4 pagesPrinciples Based Medical Informatics For Success NTSvlader Reitef VanquisherNo ratings yet
- HAADStatisticsEng2013 PDFDocument91 pagesHAADStatisticsEng2013 PDFHitesh MotwaniiNo ratings yet
- First Meeting of National Technical Working Group For Private Sector EngagementDocument21 pagesFirst Meeting of National Technical Working Group For Private Sector EngagementDr. Radhay ShyamNo ratings yet
- AfricaProgramForOncho APOCDocument2 pagesAfricaProgramForOncho APOCAbdulkader TukaleNo ratings yet
- Factors Associated With The Ineffectiveness of Epidemiological Surveillance in The Health Districts of The South Cameroon RegionDocument9 pagesFactors Associated With The Ineffectiveness of Epidemiological Surveillance in The Health Districts of The South Cameroon RegionInternational Journal of Recent Innovations in Academic ResearchNo ratings yet
- Multicentre Analysis CancerDocument8 pagesMulticentre Analysis Cancersilvio da costa guerreiroNo ratings yet
- Cervical Cancer Strategy 2018Document59 pagesCervical Cancer Strategy 2018Faisal Mohammad AhamedNo ratings yet
- Colorectal BundlesDocument16 pagesColorectal BundlesDamie ChaulaNo ratings yet
- Article 1667458231Document9 pagesArticle 1667458231bharathNo ratings yet
- Comparative Health Technology Assessment of Robotic-AssistedDocument9 pagesComparative Health Technology Assessment of Robotic-AssistedDanica SavićNo ratings yet
- NSG 523 Module 10 Dissemination Grid For ProductDocument2 pagesNSG 523 Module 10 Dissemination Grid For Productapi-354069497No ratings yet
- Essential Components of Postnatal Care - A Systematic Literature Review and Development of Signal Functions To Guide Monitoring and EvaluationDocument16 pagesEssential Components of Postnatal Care - A Systematic Literature Review and Development of Signal Functions To Guide Monitoring and EvaluationvineelainjetyNo ratings yet
- Continence AuditDocument6 pagesContinence Auditi can always make u smile :DNo ratings yet
- Impact of Technology in Better Dispersal of HealthDocument4 pagesImpact of Technology in Better Dispersal of Healthvasthu broto ariyoNo ratings yet
- Characteristics of Case Management in Primary Care PDFDocument11 pagesCharacteristics of Case Management in Primary Care PDFCamila AlmeidaNo ratings yet
- Ijerph 18 08373 v2Document14 pagesIjerph 18 08373 v2Huy Trần ThiệnNo ratings yet
- Telemedicine, Teleophthalmology Programs in Action at Johns HopkinsDocument5 pagesTelemedicine, Teleophthalmology Programs in Action at Johns HopkinsJaime Albeiro Hurtado GomezNo ratings yet
- 873 3010 2 PBDocument5 pages873 3010 2 PBandreaNo ratings yet
- Capstone Project Final DraftDocument11 pagesCapstone Project Final Draftapi-540888060No ratings yet
- Standard Operating Procedures (Sops) For Palliative Care in German Comprehensive Cancer Centers - An Evaluation of The Implementation StatusDocument9 pagesStandard Operating Procedures (Sops) For Palliative Care in German Comprehensive Cancer Centers - An Evaluation of The Implementation StatusSujan KhanNo ratings yet
- Optimización Del Proceso de Atención de Pacientes en El Área de Oftalmología Del IHSSDocument10 pagesOptimización Del Proceso de Atención de Pacientes en El Área de Oftalmología Del IHSSkarina Sanchez ValverdeNo ratings yet
- Rhodes 2015Document9 pagesRhodes 2015Achmad Ageng SeloNo ratings yet
- Paper Su Case Study Medicina Lotti PontederaDocument2 pagesPaper Su Case Study Medicina Lotti PontederaronnyNo ratings yet
- Guide For Developing AWHSC Patient Safety Policy and Strategic PlanDocument17 pagesGuide For Developing AWHSC Patient Safety Policy and Strategic PlanAddis YeshitlaNo ratings yet
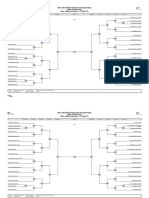
- (Day-1 Draw Sheet) Baku 2023 World Taekwondo ChampionshipsDocument4 pages(Day-1 Draw Sheet) Baku 2023 World Taekwondo ChampionshipsPhally UmNo ratings yet
- ESET Vs Bitdefender - 072314Document2 pagesESET Vs Bitdefender - 072314Phally UmNo ratings yet
- A Dec 400 Dental Equipment Brochure 85039300Document24 pagesA Dec 400 Dental Equipment Brochure 85039300Phally UmNo ratings yet
- User Manual For EasydentDocument239 pagesUser Manual For EasydentPhally UmNo ratings yet
- PROPOSED PUERTO PRINCESA HEALTH CENTER: Enhancing Tuberculosis Patient Detection and CareDocument7 pagesPROPOSED PUERTO PRINCESA HEALTH CENTER: Enhancing Tuberculosis Patient Detection and CareJaerald CruzNo ratings yet
- Johnson & Johnson Product Line, Product Mix, Marketing Mix & Branding - V ! $ T HHDocument11 pagesJohnson & Johnson Product Line, Product Mix, Marketing Mix & Branding - V ! $ T HHsharmavisthh82% (11)
- Patient Safety OfficerDocument173 pagesPatient Safety Officermsarojini100% (3)
- Basic Emergency Obstetric CareDocument4 pagesBasic Emergency Obstetric CareVirnaline VariasNo ratings yet
- 14-Rights of Drug AdministrationDocument4 pages14-Rights of Drug AdministrationFernandez, Florence Nicole100% (2)
- Community Dentistry ReviewerDocument2 pagesCommunity Dentistry ReviewerCzarina DavidNo ratings yet
- Case Study Report FinalDocument58 pagesCase Study Report Finalu6411362No ratings yet
- Test 1 NUR 151Document3 pagesTest 1 NUR 151davidvpnNo ratings yet
- Project Proposal On Youth Socio-Economic Development Centres in TanzaniaDocument15 pagesProject Proposal On Youth Socio-Economic Development Centres in TanzaniaMwagaVumbiNo ratings yet
- Artesunate Uses, Side Effects & WarningsDocument3 pagesArtesunate Uses, Side Effects & Warningstarun yadavNo ratings yet
- 4-Emotional Freedom Techniques (EFT) As A Practice For Supporting Chronic Disease Healthcare A Practitioners' PerspectiveDocument10 pages4-Emotional Freedom Techniques (EFT) As A Practice For Supporting Chronic Disease Healthcare A Practitioners' PerspectiveFria ZafriaNo ratings yet
- Ambuja Cement Foundation Visit ReportDocument5 pagesAmbuja Cement Foundation Visit ReportRavisinh ValaNo ratings yet
- Comparison Between Efficacy of Melatonin and Diazepam For Prevention of Recurrent Simple Febrile Seizures A RandomizedDocument19 pagesComparison Between Efficacy of Melatonin and Diazepam For Prevention of Recurrent Simple Febrile Seizures A RandomizedSMA N 1 TOROHNo ratings yet
- 11TH Nursing On The Move - Consolidating and Harnessing The Gains For Clinical ExcellenceDocument39 pages11TH Nursing On The Move - Consolidating and Harnessing The Gains For Clinical ExcellenceOlukayode DavidNo ratings yet
- Medical Equipment Business PlanDocument53 pagesMedical Equipment Business PlanJemimah Mejia100% (3)
- Fixed Orthodontic Retainers: A ReviewDocument5 pagesFixed Orthodontic Retainers: A ReviewhelmysiswantoNo ratings yet
- Ensuring A Patient's Right To Pastoral Care and Spiritual ServicesDocument6 pagesEnsuring A Patient's Right To Pastoral Care and Spiritual ServicesArwenn BeragoNo ratings yet
- College of St. John - Roxas: de La Salle SupervisedDocument3 pagesCollege of St. John - Roxas: de La Salle SupervisedLina Marie BesaNo ratings yet
- MOA - PhysicianDocument2 pagesMOA - PhysicianAngel Mae BaborNo ratings yet
- Ellex Glaucoma BrochureDocument12 pagesEllex Glaucoma BrochureHaag-Streit UK (HS-UK)No ratings yet
- Middle Range Theory Ellen D. Schulzt: Modeling and Role Modeling Katharine Kolcaba: Comfort TheoryDocument22 pagesMiddle Range Theory Ellen D. Schulzt: Modeling and Role Modeling Katharine Kolcaba: Comfort TheoryMerlinNo ratings yet
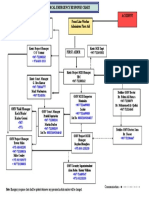
- Medical Emergency RESPONSE CHART - Doc - 1Document1 pageMedical Emergency RESPONSE CHART - Doc - 1Mohammed Ahmed NasherNo ratings yet
- 6343 (20) Ex Gaz-IIDocument23 pages6343 (20) Ex Gaz-IIHabib Ur Rehman BazmiNo ratings yet
- Mechanical Engineering and The Health SectorDocument4 pagesMechanical Engineering and The Health SectorKING ZADDYNo ratings yet
- Treatment and OutcomeDocument26 pagesTreatment and OutcomeChristine EnriquezNo ratings yet
- Lesson 1. Therapeutic Community IntroductionDocument2 pagesLesson 1. Therapeutic Community IntroductionBrielle Shai Cruz100% (1)
- NURSING PROCESS FundaDocument26 pagesNURSING PROCESS FundaDELA CRUZ, JENISSE LOUISSENo ratings yet
- Labor Room and DNC Chart BeghDocument3 pagesLabor Room and DNC Chart BeghTeanu Jose Gabrillo TamayoNo ratings yet
- SISTEM TRIAGE - Dr. Mirza, SP - An, FIPM, FIPPDocument34 pagesSISTEM TRIAGE - Dr. Mirza, SP - An, FIPM, FIPPlittle sunflowerfieldNo ratings yet
- Medication Error Reporting FormDocument2 pagesMedication Error Reporting Formahmad ganieNo ratings yet