You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5796)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Fall2022PHAR128 AnalChem1CH0Student ALLDocument87 pagesFall2022PHAR128 AnalChem1CH0Student ALLErsin TukenmezNo ratings yet
- Fact Sheet For Potential UPB Exchange Students - 2021-22Document3 pagesFact Sheet For Potential UPB Exchange Students - 2021-22Ersin TukenmezNo ratings yet
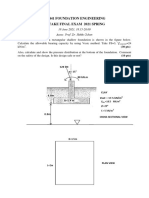
- Ce 441 Foundation Engineering Retake Final Exam 2021 SpringDocument2 pagesCe 441 Foundation Engineering Retake Final Exam 2021 SpringErsin TukenmezNo ratings yet
- ACFrOgD8mx1aj1NlKb5479so 1JW7zuyY rDfTA-F1b4xL-ijXcw9dz lrQ45xO6Z9867rqhFFkFtiBxdv9rd PnG4aFz7wpQ6TjpRyMGjnRDuIxt-gI avIe41pTKXKe-AYLrs Kx4fnBvLKc2SDocument41 pagesACFrOgD8mx1aj1NlKb5479so 1JW7zuyY rDfTA-F1b4xL-ijXcw9dz lrQ45xO6Z9867rqhFFkFtiBxdv9rd PnG4aFz7wpQ6TjpRyMGjnRDuIxt-gI avIe41pTKXKe-AYLrs Kx4fnBvLKc2SErsin TukenmezNo ratings yet
- Principles of Economics: Global EditionDocument31 pagesPrinciples of Economics: Global EditionErsin TukenmezNo ratings yet
- Principles of Economics: Global EditionDocument38 pagesPrinciples of Economics: Global EditionErsin TukenmezNo ratings yet
- Principles of Economics: Global EditionDocument34 pagesPrinciples of Economics: Global EditionErsin TukenmezNo ratings yet
- Principles of Economics: Global EditionDocument45 pagesPrinciples of Economics: Global EditionErsin TukenmezNo ratings yet
- Principles of Economics: Global EditionDocument43 pagesPrinciples of Economics: Global EditionErsin TukenmezNo ratings yet
- Principles of Economics: Global EditionDocument40 pagesPrinciples of Economics: Global EditionErsin TukenmezNo ratings yet
- Principles of Economics: Global EditionDocument28 pagesPrinciples of Economics: Global EditionErsin TukenmezNo ratings yet
- Principles of Economics: Global EditionDocument41 pagesPrinciples of Economics: Global EditionErsin TukenmezNo ratings yet
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (589)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (400)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (345)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1091)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (121)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- Ramirez Final Rca PaperDocument5 pagesRamirez Final Rca Paperapi-351096424No ratings yet
- Standard Methods For Apis Mellifera Pest and Pathogen Research IntroductionDocument4 pagesStandard Methods For Apis Mellifera Pest and Pathogen Research IntroductionKátia Peres GramachoNo ratings yet
- Karen Clarke - BSDH PresentationDocument28 pagesKaren Clarke - BSDH PresentationWaheed UllahNo ratings yet
- Hindustan TimesMumbai18!04!202069678Document12 pagesHindustan TimesMumbai18!04!202069678Kristic AngelNo ratings yet
- Current Status and Risk Factors of Canine ParvovirusDocument7 pagesCurrent Status and Risk Factors of Canine Parvovirustomas whaterzonNo ratings yet
- Clinical Presentation, Diagnosis, and Initial Evaluation of Diabetes Mellitus in Adults - UpToDateDocument21 pagesClinical Presentation, Diagnosis, and Initial Evaluation of Diabetes Mellitus in Adults - UpToDatePriscillaNo ratings yet
- Antibiotic Guidelines For BONE AND JOINT INFECTIONSDocument3 pagesAntibiotic Guidelines For BONE AND JOINT INFECTIONSKhurram NadeemNo ratings yet
- Case Study For PneumoniaDocument11 pagesCase Study For PneumoniaGabbii Cinco100% (1)
- np4 TestDocument8 pagesnp4 TestMargie BalunesNo ratings yet
- Abses ParafaringDocument10 pagesAbses ParafaringfayzaNo ratings yet
- Auntminnie SignsDocument56 pagesAuntminnie SignsHey ReelNo ratings yet
- Catalogue Biosynex 2022 Export June Final PrintDocument52 pagesCatalogue Biosynex 2022 Export June Final PrintThiago GalloNo ratings yet
- Rapid Assessment of Viral Hepatitis Testing and Quality AssuranceDocument18 pagesRapid Assessment of Viral Hepatitis Testing and Quality AssuranceCHELSIE KAITLYN DE GUZMANNo ratings yet
- Nosocomial Infection. BPTDocument44 pagesNosocomial Infection. BPTAanchal GuptaNo ratings yet
- Alberti 2004Document14 pagesAlberti 2004Messias FilhoNo ratings yet
- Mechanisms of Diabetic ComplicatioDocument52 pagesMechanisms of Diabetic ComplicatioRaffaharianggaraNo ratings yet
- Jamaica Times October 2014Document28 pagesJamaica Times October 2014Jamaica Times Newspaper100% (1)
- Ms Word Notes - Template (May 2022)Document4 pagesMs Word Notes - Template (May 2022)Jaycee Anne AregloNo ratings yet
- NQVH The Hall Technique ManualDocument19 pagesNQVH The Hall Technique Manualpriti adsulNo ratings yet
- Case Study PsychDocument49 pagesCase Study PsychMonique Reyes100% (1)
- Colibacillosis in Calves: A Review of Literature: Bashahun, G. M. and Amina ADocument10 pagesColibacillosis in Calves: A Review of Literature: Bashahun, G. M. and Amina APrabhu KumarNo ratings yet
- ABG Tic Tac Toe CalculationDocument6 pagesABG Tic Tac Toe CalculationnatkwqNo ratings yet
- Manual Therapy of The HipDocument23 pagesManual Therapy of The HipSardarChangezKhanNo ratings yet
- Offer LetterDocument2 pagesOffer LetterAtiqah JohanNo ratings yet
- Benign Essential Blepharospasm Information Page - National Institute of Neurological Disorders and StrokeDocument2 pagesBenign Essential Blepharospasm Information Page - National Institute of Neurological Disorders and StrokeJP OmerNo ratings yet
- Five Machine Learning Supervised Algorithms For The Analysis and The Prediction of ObesityDocument9 pagesFive Machine Learning Supervised Algorithms For The Analysis and The Prediction of ObesityInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Sevenhills Rises From The Dust: InsideDocument28 pagesSevenhills Rises From The Dust: Insideudhaya kumarNo ratings yet
- Furosemide Stress Test As A Predictive Marker of Acute Kidney Injury Progression or Renal Replacement TherapyDocument13 pagesFurosemide Stress Test As A Predictive Marker of Acute Kidney Injury Progression or Renal Replacement Therapyjose luis iribarrenNo ratings yet
- Critical Care Nursing AssignmentDocument13 pagesCritical Care Nursing Assignmentiqmal irfamimi50% (2)
- MMSU Psychosocial Assessment GuideDocument8 pagesMMSU Psychosocial Assessment GuideJohn Michael TaylanNo ratings yet