You might also like
- 2 Step PPD FormDocument1 page2 Step PPD FormWilliamNo ratings yet
- GBS Source 1Document4 pagesGBS Source 1PJHG50% (2)
- Asthma Reading Task Text A and B Oet Reading NotesDocument16 pagesAsthma Reading Task Text A and B Oet Reading NotesSakshi RanbhiseNo ratings yet
- Thorn Eh and OutDocument24 pagesThorn Eh and OutNick MaxNo ratings yet
- Prescription Template 10Document2 pagesPrescription Template 10Yasser SebtiNo ratings yet
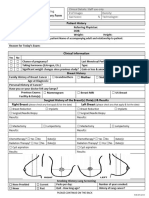
- Mammogram Patient History FormDocument2 pagesMammogram Patient History FormChandrashekhar SohoniNo ratings yet
- FAQs About MammographyDocument3 pagesFAQs About Mammographyh0neylipsNo ratings yet
- Breast Cancer Overview - Dr. Jamal Melhem 25 Sept. 2016Document69 pagesBreast Cancer Overview - Dr. Jamal Melhem 25 Sept. 2016Mohammad BanisalmanNo ratings yet
- Understanding Breast Imaging - Breast360.org - The American Society of Breast Surgeons Foundation PDFDocument5 pagesUnderstanding Breast Imaging - Breast360.org - The American Society of Breast Surgeons Foundation PDFdivyanshu kumarNo ratings yet
- Clinical Evaluation of The BreasDocument6 pagesClinical Evaluation of The BreasSalim Mwiti NabeaNo ratings yet
- Breast Cancer Missed at Screening Hindsight or MiDocument6 pagesBreast Cancer Missed at Screening Hindsight or MideaNo ratings yet
- CI Claim - Doctor's Statement CANCER - Ver JUNE 2020Document3 pagesCI Claim - Doctor's Statement CANCER - Ver JUNE 2020ambonboenda88No ratings yet
- MED2 5.01A Treatment Modalities in Cancer (Part 1) - Dr. F. AdefuinDocument3 pagesMED2 5.01A Treatment Modalities in Cancer (Part 1) - Dr. F. AdefuinAra DiocosNo ratings yet
- 3 - NCM112Document6 pages3 - NCM112Edthel IniegoNo ratings yet
- Breast CA SeminarDocument60 pagesBreast CA SeminarAliyi MuktarNo ratings yet
- Breast CaDocument6 pagesBreast CaSalim Mwiti NabeaNo ratings yet
- Breast Study Guide: Updated 10/2/2015Document3 pagesBreast Study Guide: Updated 10/2/2015Koyawin XNo ratings yet
- 145 1491 PDFDocument5 pages145 1491 PDFNathalie DeviNo ratings yet
- Masa Palpable en MamaDocument22 pagesMasa Palpable en MamaarcaNo ratings yet
- Breast and Ovarian Cancer - PresentationDocument26 pagesBreast and Ovarian Cancer - PresentationRawa MuhsinNo ratings yet
- Mamo GramDocument1 pageMamo GramtaniamarqueslawNo ratings yet
- Breast Implant Evaluation - NarrativeDocument25 pagesBreast Implant Evaluation - Narrativeopenlab.doisNo ratings yet
- Second and Third Trimester Screening For Fetal AnomalyDocument12 pagesSecond and Third Trimester Screening For Fetal AnomalyIqra NazNo ratings yet
- MAMOGRAFIADocument2 pagesMAMOGRAFIAFabián Alejandro Vargas VillalbaNo ratings yet
- Evidence Based Medicine - OncologyDocument17 pagesEvidence Based Medicine - OncologyvivianNo ratings yet
- Cancer Antigen (Ca) 15.3: Subtypes of Breast CancerDocument4 pagesCancer Antigen (Ca) 15.3: Subtypes of Breast Cancerडा. सत्यदेव त्यागी आर्यNo ratings yet
- Untitled PDFDocument9 pagesUntitled PDFFaruq AbdanNo ratings yet
- CRICO/RMF Breast Care Management Algorithm: Improving Breast Patient SafetyDocument8 pagesCRICO/RMF Breast Care Management Algorithm: Improving Breast Patient SafetyAbdur Rachman Ba'abdullahNo ratings yet
- Prophylactic Irradiation To The Contralateral BreaDocument6 pagesProphylactic Irradiation To The Contralateral Breaashnamuni07No ratings yet
- Comparison of Ultrasound and Mammography For Early DiagnosisDocument8 pagesComparison of Ultrasound and Mammography For Early Diagnosishdh1224No ratings yet
- DiscussionDocument22 pagesDiscussionapi-3701915No ratings yet
- What Is A Mammogram?: CalciumDocument8 pagesWhat Is A Mammogram?: CalciumPramu AmanahNo ratings yet
- Fa Lomo 2018Document6 pagesFa Lomo 2018Mateus CespedesNo ratings yet
- Breast CancerDocument4 pagesBreast CancerBlad AnneNo ratings yet
- Document 4Document3 pagesDocument 4bill linNo ratings yet
- Local Management of Invasive Breast Cancer: by Steven Jones, MDDocument37 pagesLocal Management of Invasive Breast Cancer: by Steven Jones, MDsrikadarinahNo ratings yet
- RAFIN - Management of The Client With Cervical - Ovarian-Cancer and HysterectomyDocument12 pagesRAFIN - Management of The Client With Cervical - Ovarian-Cancer and HysterectomyCezanne CruzNo ratings yet
- Breast PainDocument9 pagesBreast PainmarysrbNo ratings yet
- Brca Mast Vs ConservadoraDocument20 pagesBrca Mast Vs ConservadoraVictoria DuqueNo ratings yet
- Wa0039.Document4 pagesWa0039.Debraj SahaNo ratings yet
- ACR Appropriateness Criteria Pancreatic CystDocument9 pagesACR Appropriateness Criteria Pancreatic CystSole GonzalezNo ratings yet
- Breast Cancer ScreeningDocument53 pagesBreast Cancer ScreeningSmita B GoyalNo ratings yet
- Screening For Cancer of The Cervix: An Office Manual For Health Care ProvidersDocument16 pagesScreening For Cancer of The Cervix: An Office Manual For Health Care ProvidersYosie Yulanda PutraNo ratings yet
- Hereditary Breast CancerDocument68 pagesHereditary Breast CancerAkhil Thomas JacobNo ratings yet
- Ijcmr 1184 Dec 28Document3 pagesIjcmr 1184 Dec 28BayuHernawanRahmatMuhariaNo ratings yet
- Tiwari 2017Document3 pagesTiwari 2017Dewa OkaNo ratings yet
- Challenging Clinical Scenarios of The BreastDocument62 pagesChallenging Clinical Scenarios of The BreastMuhammad HassanNo ratings yet
- Brochure Prenatal TestingDocument4 pagesBrochure Prenatal TestingMCuk2606No ratings yet
- GEHC One Stop Clinic - GLOBAL JB17786XXDocument8 pagesGEHC One Stop Clinic - GLOBAL JB17786XXsoyuzmedimaging and diagnostics ltdNo ratings yet
- ImagingDocument2 pagesImagingFitri WirastamiNo ratings yet
- Cjim 12 573Document7 pagesCjim 12 573MR Emam - GamingNo ratings yet
- Paper ERIKA Core BXDocument8 pagesPaper ERIKA Core BXHarlley SenaNo ratings yet
- Diagnostic Imaging Pathways ArticleDocument14 pagesDiagnostic Imaging Pathways Articlemashuri muhammad bijuriNo ratings yet
- Mammogram Report: Digital MammographyDocument2 pagesMammogram Report: Digital MammographyAdrian KitNo ratings yet
- KJR 17 59Document10 pagesKJR 17 59Regi FauzanNo ratings yet
- PIIS1546144009004803Document10 pagesPIIS1546144009004803Cesar ProJimenezNo ratings yet
- Journal ClubDocument60 pagesJournal ClubSataroopa SirigiriNo ratings yet
- Эластография 1Document8 pagesЭластография 1Роман КлоковNo ratings yet
- Breast LectureDocument98 pagesBreast LectureTopher ReyesNo ratings yet
- PIIS1089251613000930Document9 pagesPIIS1089251613000930rasminojNo ratings yet
- Potential Impact of Tomosynthesis On The Detection and Diagnosis of Breast LesionsDocument11 pagesPotential Impact of Tomosynthesis On The Detection and Diagnosis of Breast LesionsMR Emam - GamingNo ratings yet
- SlidesDocument283 pagesSlidesLuis SussiniNo ratings yet
- MATERI WEBINAR PRODIA Ovarian CancerDocument57 pagesMATERI WEBINAR PRODIA Ovarian CancerSylvia LestariNo ratings yet
- Prescription Template 14Document3 pagesPrescription Template 144NM19CS099 KUMAR NISHANTNo ratings yet
- Prescription Template 05Document2 pagesPrescription Template 054NM19CS099 KUMAR NISHANTNo ratings yet
- Prescription Template 07Document3 pagesPrescription Template 074NM19CS099 KUMAR NISHANTNo ratings yet
- Prescription Template 02Document2 pagesPrescription Template 024NM19CS099 KUMAR NISHANTNo ratings yet
- General Medicine Thesis TopicsDocument4 pagesGeneral Medicine Thesis Topicsxxsfomwff100% (2)
- Dengue OutlineDocument6 pagesDengue OutlineLouie George NeriNo ratings yet
- VS TL - Protein - L1 29261 2303 3Document7 pagesVS TL - Protein - L1 29261 2303 3Hadi BitarNo ratings yet
- Geriatric Medicine and Gerontology: Prevention of Frailty in The Elderly Through Physical Activity and NutritionDocument8 pagesGeriatric Medicine and Gerontology: Prevention of Frailty in The Elderly Through Physical Activity and NutritionSARAH AZIZAH 2015No ratings yet
- National Diabetes Fact Sheet, 2011: Diabetes Affects 25.8 Million People 8.3% of The U.S. PopulationDocument12 pagesNational Diabetes Fact Sheet, 2011: Diabetes Affects 25.8 Million People 8.3% of The U.S. PopulationAnonymous bq4KY0mcWGNo ratings yet
- Additional RRLDocument3 pagesAdditional RRLManuel Jaro ValdezNo ratings yet
- DuaventDocument9 pagesDuaventAjurs UrsabiaNo ratings yet
- DkaDocument83 pagesDkaRajaKumar Ponnana100% (1)
- Chronic PeriodontitisDocument3 pagesChronic Periodontitisapi-537687828No ratings yet
- Management of Acne Scarring, Part II: A Comparative Review of Non-Laser-Based, Minimally Invasive ApproachesDocument10 pagesManagement of Acne Scarring, Part II: A Comparative Review of Non-Laser-Based, Minimally Invasive ApproachesShintaNo ratings yet
- SOMATOM Volume Zoom Routine VA40Document136 pagesSOMATOM Volume Zoom Routine VA40gallu797462No ratings yet
- Hope 1 - FitnessDocument13 pagesHope 1 - FitnessMark Clemence R. ParcasioNo ratings yet
- Family Therapy and Systemic PracticeDocument4 pagesFamily Therapy and Systemic PracticeUyên TrươngNo ratings yet
- Parameter For Mindray Reagent On BS-400 (V12.0)Document3 pagesParameter For Mindray Reagent On BS-400 (V12.0)НиколайКрылов100% (1)
- Advanced Drug Delivery Reviews: Sadaf Aghevlian, Amanda J. Boyle, Raymond M. ReillyDocument17 pagesAdvanced Drug Delivery Reviews: Sadaf Aghevlian, Amanda J. Boyle, Raymond M. ReillyKamila MartinNo ratings yet
- LaryngoscopeDocument97 pagesLaryngoscopeMohammed NaserNo ratings yet
- Knowledge, Attitude and Practice (Kap) Study OnDocument52 pagesKnowledge, Attitude and Practice (Kap) Study OnQazi Muhammad IqbalNo ratings yet
- VINCENT P. Et Al. 2007 PDFDocument3 pagesVINCENT P. Et Al. 2007 PDFLiga Odontopediatria RondonienseNo ratings yet
- Trichuris TrichiuraDocument16 pagesTrichuris TrichiuraPaul Avila SorianoNo ratings yet
- Endobutton Family BrochureDocument6 pagesEndobutton Family BrochureRicardo Chaconbenjumea100% (1)
- Clinical Handbook of Couple TherapyDocument2 pagesClinical Handbook of Couple TherapyLaura AndreiNo ratings yet
- Circadian RhythmsDocument4 pagesCircadian Rhythmsapi-642709499No ratings yet
- ParasomniaDocument27 pagesParasomniaVoltic AceroNo ratings yet
- Acute Epididymoorchitis and Torsion of Testis: Seminar 6Document37 pagesAcute Epididymoorchitis and Torsion of Testis: Seminar 6Kumutha MalarNo ratings yet
- 10 - Neonaticide, Infanticide and Child HomicideDocument45 pages10 - Neonaticide, Infanticide and Child HomicideWala AbdeljawadNo ratings yet
- WHO - HQ - Reports G2 PROD EXT TBCountryProfileDocument1 pageWHO - HQ - Reports G2 PROD EXT TBCountryProfileAngelo Santos EstrellaNo ratings yet