You might also like
- Biochemical Aspects of Plant-Parasite Relationships: Proceedings of The Phytochemical Society Symposium University of Hull, England April, 1975From EverandBiochemical Aspects of Plant-Parasite Relationships: Proceedings of The Phytochemical Society Symposium University of Hull, England April, 1975J. FriendNo ratings yet
- Kang, Sewong, Etc. 2019. Fitzpatrick's Dermatology 9th Edition, 2-Volume Set FF. p-3436-3448Document10 pagesKang, Sewong, Etc. 2019. Fitzpatrick's Dermatology 9th Edition, 2-Volume Set FF. p-3436-3448gia purnamaNo ratings yet
- Pen GDocument3 pagesPen GjohannakatebellyNo ratings yet
- Human Defensins Facilitate Local Unfolding of Thermodynamically Un - 2014 - ImmuDocument13 pagesHuman Defensins Facilitate Local Unfolding of Thermodynamically Un - 2014 - ImmuDaniah Marwan Dawood DAWOODNo ratings yet
- Bachteriophage: Phage T4 Infected Bacterium E.coliDocument29 pagesBachteriophage: Phage T4 Infected Bacterium E.coliTiara AmbarNo ratings yet
- FCM DifteriDocument1 pageFCM Difterishafa ikeuNo ratings yet
- Bacteria Trigger Words Biology, Virulence and Epidemiology Disease Diagnosis Treatment, Prevention and ControlDocument3 pagesBacteria Trigger Words Biology, Virulence and Epidemiology Disease Diagnosis Treatment, Prevention and ControlEdward IbarraNo ratings yet
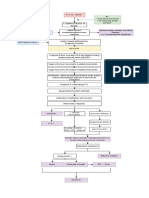
- Diphtheria Schematic Diagram (Pathophysiology0Document3 pagesDiphtheria Schematic Diagram (Pathophysiology0Kathlene Boleche100% (1)
- 181 Supplement 1 S156Document12 pages181 Supplement 1 S156Hanung PujanggaNo ratings yet
- Nature 14098Document19 pagesNature 14098Noelia Alexandra Estrada SilvaNo ratings yet
- The Dynamics of Dendritic Cell Mediated Innate Immune RegulationDocument6 pagesThe Dynamics of Dendritic Cell Mediated Innate Immune RegulationSofi Papel JachoNo ratings yet
- Summary Lecture 20 PDFDocument7 pagesSummary Lecture 20 PDFmanar aleneziNo ratings yet
- Microbiome and Diseases: Pathogen Infection: Christine Josenhans and Guntram A. GrasslDocument22 pagesMicrobiome and Diseases: Pathogen Infection: Christine Josenhans and Guntram A. GrasslÂngela Souza BarroqueiroNo ratings yet
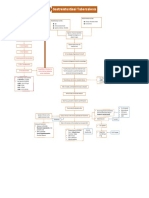
- Gastrointestinal Tuberculosis: PathogenesisDocument1 pageGastrointestinal Tuberculosis: Pathogenesis알파No ratings yet
- Resolving InflammationDocument13 pagesResolving InflammationTalita FernandesNo ratings yet
- Cory Ne Bacteria FinalDocument3 pagesCory Ne Bacteria Final2013SecBNo ratings yet
- MB GP 4 B& C PassDocument3 pagesMB GP 4 B& C PassJulia IshakNo ratings yet
- Bacillus Thuringiensis A Century of Research, Development and Commercial ApplicationDocument18 pagesBacillus Thuringiensis A Century of Research, Development and Commercial ApplicationNguyễn Thị Hoài ThươngNo ratings yet
- 0.5 ML Repeat at 4-8weeks After First Dose and at 6-12 Months After Second DoseDocument2 pages0.5 ML Repeat at 4-8weeks After First Dose and at 6-12 Months After Second DoseLenneth Ann M. LozadaNo ratings yet
- 5.2 Melchizedek Santander - Clinical Case Activity NMD 4 Group 5 Cellulitis and Necrotizing Fasciitis Week 5 Day 2Document2 pages5.2 Melchizedek Santander - Clinical Case Activity NMD 4 Group 5 Cellulitis and Necrotizing Fasciitis Week 5 Day 2Melchizedek M. SantanderNo ratings yet
- Nejat 2017Document16 pagesNejat 2017László SágiNo ratings yet
- Staphylococcus: Skin Infections Osteomyelitis Bloodstream Infection Food Poisoning Foreign Body Infections MRSADocument7 pagesStaphylococcus: Skin Infections Osteomyelitis Bloodstream Infection Food Poisoning Foreign Body Infections MRSAnour achkarNo ratings yet
- Leptospira PDFDocument15 pagesLeptospira PDFcarlos javierNo ratings yet
- Correspondence: Peritonitis Due To Multiresistant Rhizobium RadiobacterDocument5 pagesCorrespondence: Peritonitis Due To Multiresistant Rhizobium RadiobacterFrontiersNo ratings yet
- Micro paraDocument2 pagesMicro parafeminaNo ratings yet
- Prokaryotes DoneDocument39 pagesProkaryotes Doneeyadballas35No ratings yet
- Ryan-Adley2014 Article RalstoniaSppEmergingGlobalOppo PDFDocument14 pagesRyan-Adley2014 Article RalstoniaSppEmergingGlobalOppo PDFYohanna GomesNo ratings yet
- Khurana2019 PDFDocument9 pagesKhurana2019 PDFEka FaridaNo ratings yet
- DIPTHERIADocument1 pageDIPTHERIAGrace StephanieNo ratings yet
- Antimicrobial Drugs of ChoiceDocument9 pagesAntimicrobial Drugs of ChoiceB-Pharma Traders ugNo ratings yet
- Ciprofloxacin Conjugated To Diphenyltin (IV) : A Novel Formulation With Enhanced Antimicrobial ActivityDocument15 pagesCiprofloxacin Conjugated To Diphenyltin (IV) : A Novel Formulation With Enhanced Antimicrobial ActivitymaczweiNo ratings yet
- Quiz On Prepositions Stative Verbs and Logical FallaciesDocument3 pagesQuiz On Prepositions Stative Verbs and Logical FallaciesBeatrice Lianne Francisco EstacioNo ratings yet
- MIT Environment 11-18-04Document3 pagesMIT Environment 11-18-04Dr. Ir. R. Didin Kusdian, MT.No ratings yet
- Coaggregation Chicken LactobacilliDocument6 pagesCoaggregation Chicken LactobacillianjaliboseNo ratings yet
- Harmful Algae: ReviewDocument27 pagesHarmful Algae: Reviewdioalif anantaNo ratings yet
- ImmunityDocument37 pagesImmunityRand Hussein100% (1)
- Fungal Genetics and Biology: Antifungal Resistance in Dermatophytes: Recent Trends and Therapeutic ImplicationsDocument9 pagesFungal Genetics and Biology: Antifungal Resistance in Dermatophytes: Recent Trends and Therapeutic ImplicationsputriNo ratings yet
- Development of Neutralizing and Non Neutralizing Antibodies Targeting Known and Novel Epitopes Os TCDBDocument16 pagesDevelopment of Neutralizing and Non Neutralizing Antibodies Targeting Known and Novel Epitopes Os TCDBClovis Moreira JrNo ratings yet
- Tonsilitis + Scarlet + MeningitisDocument3 pagesTonsilitis + Scarlet + Meningitisd3mooz13No ratings yet
- Wuolah Free Bacteria TableDocument11 pagesWuolah Free Bacteria TableELENA FERNANDEZNo ratings yet
- Dexamethasone Nanomedicines For COVID-19: Comment - FOCUSDocument3 pagesDexamethasone Nanomedicines For COVID-19: Comment - FOCUSmwdhtirahNo ratings yet
- Periowave Benhamou Case StudyDocument8 pagesPeriowave Benhamou Case StudyJas SandhuNo ratings yet
- 1-Mbio - 2021 - Gago-Córdoba C Et, AlDocument15 pages1-Mbio - 2021 - Gago-Córdoba C Et, AlAntonNo ratings yet
- Editorial: Recent Progresses in Amebiasis: Anjan Debnath, Mario Alberto Rodriguez and Serge AnkriDocument4 pagesEditorial: Recent Progresses in Amebiasis: Anjan Debnath, Mario Alberto Rodriguez and Serge AnkriJonatan GalvánNo ratings yet
- Crawford Hes Lec Sas 11Document10 pagesCrawford Hes Lec Sas 11Divo SkyeNo ratings yet
- 2012-Bti ABC Transporter Toxin ModeDocument8 pages2012-Bti ABC Transporter Toxin ModeDwiNo ratings yet
- Hai Toolkit For LTCDocument82 pagesHai Toolkit For LTCShannaNo ratings yet
- Par Veen 2019Document15 pagesPar Veen 2019Shirley RamirezNo ratings yet
- Criptococosis 2021Document13 pagesCriptococosis 2021Alejandra OrtizNo ratings yet
- Metronidazole: Jerod L. Nagel and David M. AronoffDocument12 pagesMetronidazole: Jerod L. Nagel and David M. AronoffSOFIA TORRES OLAYANo ratings yet
- (PDF) Successful Treatment of Recalcitrant Condyloma With Topical CidofovirDocument2 pages(PDF) Successful Treatment of Recalcitrant Condyloma With Topical Cidofoviralihass88No ratings yet
- T Lymphocyte Exhaustion During Human and Experimental Visceral LeishmaniasisDocument15 pagesT Lymphocyte Exhaustion During Human and Experimental Visceral LeishmaniasisLuis Carlos Calvanapon TerronesNo ratings yet
- Bacterial Toxins: Yogi Khoirul Abror Departement of Immunology Postgraduate Programme Airlangga UniversityDocument20 pagesBacterial Toxins: Yogi Khoirul Abror Departement of Immunology Postgraduate Programme Airlangga UniversityYogiabrorNo ratings yet
- Kocluhetemoglu 2018Document5 pagesKocluhetemoglu 2018adNo ratings yet
- Systematic Approach in Selecting AntibioticsDocument5 pagesSystematic Approach in Selecting AntibioticsWu Yi FanNo ratings yet
- AntibioticosDocument11 pagesAntibioticosdroswaldo88No ratings yet
- Patient Based PathophysiologyDocument3 pagesPatient Based PathophysiologyJeizel IgnacioNo ratings yet
- PlantPathology McNew 23-34 58-60Document26 pagesPlantPathology McNew 23-34 58-60Gabriel ViniciusNo ratings yet
- Lab Report Exp 5Document5 pagesLab Report Exp 5Brilliant SiemaNo ratings yet
- Trichomonas 3Document11 pagesTrichomonas 3ELSA NOVANTINo ratings yet
- Patient Centred Surveillance of Drug Resistant PathogensDocument19 pagesPatient Centred Surveillance of Drug Resistant PathogensHanna alexanderNo ratings yet
- Types of FeverDocument10 pagesTypes of Fevermd191031No ratings yet
- Dorrington, DR Alex Microscopic Colitis - A4 - 141220 PDFDocument2 pagesDorrington, DR Alex Microscopic Colitis - A4 - 141220 PDFRamesh SinghNo ratings yet
- Rheumatic-FeverDocument35 pagesRheumatic-FeverHasan Diab0% (2)
- Immunization - Dr. SarahDocument14 pagesImmunization - Dr. Sarahf6bk6xnppyNo ratings yet
- Molluscum ContagiosumDocument2 pagesMolluscum ContagiosumMalueth AnguiNo ratings yet
- University of Santo Tomas Faculty of Medicine and Surgery Department of Pediatrics Clinical DivisionDocument3 pagesUniversity of Santo Tomas Faculty of Medicine and Surgery Department of Pediatrics Clinical DivisionJolaine ValloNo ratings yet
- Rehman Medical Institute: Test Result Unit Reference ValuesDocument1 pageRehman Medical Institute: Test Result Unit Reference ValuesfahadbasahirNo ratings yet
- Elisa & RiaDocument4 pagesElisa & Riadihajum3No ratings yet
- Clinical Immunology and Serology A Laboratory Perspective 3rd Edition Stevens Test BankDocument12 pagesClinical Immunology and Serology A Laboratory Perspective 3rd Edition Stevens Test Banktracybrownfmaczqejxw100% (16)
- Handbook For Vaccine and Cold Chain HandlersDocument128 pagesHandbook For Vaccine and Cold Chain HandlersRyza Jazid Baharuddin NurNo ratings yet
- LimfadenitisDocument24 pagesLimfadenitisrahmah ningsihNo ratings yet
- WEEK 10 LABORATORY EXERCISE - Lymphatic Immune SystemDocument7 pagesWEEK 10 LABORATORY EXERCISE - Lymphatic Immune SystemEricka ElloNo ratings yet
- Rho (D) Immune Globulin (Human) - RhogamDocument4 pagesRho (D) Immune Globulin (Human) - RhogamJamaicah IliganNo ratings yet
- Study Notes Respiratory SystemDocument19 pagesStudy Notes Respiratory SystemAnde Mangkuluhur Azhari ThalibbanNo ratings yet
- WM68Document8 pagesWM68Garima AgrawalNo ratings yet
- Individualized Neoantigen-Specific ImmunotherapyDocument16 pagesIndividualized Neoantigen-Specific ImmunotherapyEhed AymazNo ratings yet
- Hepatits DDocument13 pagesHepatits Dmihnea soareNo ratings yet
- COVID19 Flu A&b Ag Combo Rapid Test SELL SHEET OG (1) - CompressedDocument3 pagesCOVID19 Flu A&b Ag Combo Rapid Test SELL SHEET OG (1) - CompressedmlgraziosiNo ratings yet
- Nursing Care For A Family Caring For Children With Infectious DiseaseDocument4 pagesNursing Care For A Family Caring For Children With Infectious DiseasekdfhjfhfNo ratings yet
- Faktor HospesDocument22 pagesFaktor Hospesari purwandiniNo ratings yet
- Otology: Dave Pothier ST Mary's 2003Document36 pagesOtology: Dave Pothier ST Mary's 2003Mamadovic MubarekNo ratings yet
- Capaian Mutu Respon Time Igd-2Document1,536 pagesCapaian Mutu Respon Time Igd-2Arsyad AkmatulNo ratings yet
- University of Northern PhilippinesDocument4 pagesUniversity of Northern PhilippinesCatherine PradoNo ratings yet
- Nursing Lab 3 Skill Performance Checklist Administering A Blood Transfusion S U NP CommentsDocument2 pagesNursing Lab 3 Skill Performance Checklist Administering A Blood Transfusion S U NP CommentsCandice Cheng88% (8)
- Who Influenza SurveillanceDocument153 pagesWho Influenza SurveillanceRidho Al FiqriNo ratings yet
- CV-polar Flagella PE - Multiple Flagella: Spore Survives in BC GRAM POS OBLIGATE AEROBE - Bacillus, NocardiaDocument4 pagesCV-polar Flagella PE - Multiple Flagella: Spore Survives in BC GRAM POS OBLIGATE AEROBE - Bacillus, NocardiaMica SaeronNo ratings yet
- Mumps: Resurgence of A Once-Dormant Disease: Published Ahead-Of-PrintDocument4 pagesMumps: Resurgence of A Once-Dormant Disease: Published Ahead-Of-Printanindya nandiniNo ratings yet
- Dengue Fever Health TeachingDocument3 pagesDengue Fever Health TeachingDante Sales100% (3)
- Haemophilus, BordetellaDocument26 pagesHaemophilus, BordetellaCătălina ProcopieNo ratings yet