You might also like
- THE - Jose SILVA - METHODDocument43 pagesTHE - Jose SILVA - METHODszijsaNo ratings yet
- Coursebook-Livertransplant ch27Document53 pagesCoursebook-Livertransplant ch27Сергей СадовниковNo ratings yet
- Cultural Humility in Psychotherapy SupervisionDocument19 pagesCultural Humility in Psychotherapy SupervisionMilo DueNo ratings yet
- Erich Fromm - A Therapeutic Vision Well Ahead of Its TimeDocument8 pagesErich Fromm - A Therapeutic Vision Well Ahead of Its TimeSteluța DrâmbuNo ratings yet
- Personal Development: Performance TaskDocument3 pagesPersonal Development: Performance TaskharrygolunaNo ratings yet
- Portal Hypertension SurgeryDocument6 pagesPortal Hypertension SurgeryjackSNMMCNo ratings yet
- Ampullary Carcinoma: Treatment and PrognosisDocument24 pagesAmpullary Carcinoma: Treatment and PrognosisHugo Alves100% (1)
- List of Chennai Hospitals 5Document15 pagesList of Chennai Hospitals 5Vaishnavi GnanasekaranNo ratings yet
- Portal Vein Embolization: State-of-the-Art Technique and Options To Improve Liver HypertrophyDocument7 pagesPortal Vein Embolization: State-of-the-Art Technique and Options To Improve Liver HypertrophyalameluNo ratings yet
- Hep4 6 1803Document10 pagesHep4 6 1803Omar Vasquez GomezNo ratings yet
- Meta 4 - de Jong DM - 2022Document13 pagesMeta 4 - de Jong DM - 2022matheus.verasNo ratings yet
- Surgical Techniques For Pancreas Transplantation: Ugo Boggi, Gabriella Amorese and Piero MarchettiDocument10 pagesSurgical Techniques For Pancreas Transplantation: Ugo Boggi, Gabriella Amorese and Piero MarchettiNatalindah Jokiem Woecandra T. D.No ratings yet
- LT 21509 PDFDocument11 pagesLT 21509 PDFAmmar magdyNo ratings yet
- Pembimbing: Dr. Henry Sitanggang, Sp.B. Disusun Oleh: Nama: Cut Heldamarinta NPM: 7110080013Document21 pagesPembimbing: Dr. Henry Sitanggang, Sp.B. Disusun Oleh: Nama: Cut Heldamarinta NPM: 7110080013Ani Riani SunartoNo ratings yet
- Journal ReadingDocument8 pagesJournal ReadingAnonymous Uh2myPxPHNo ratings yet
- Liver Transplantation - 2017 - Thornburg - Interventional Radiology in The Management of The Liver Transplant PatientDocument14 pagesLiver Transplantation - 2017 - Thornburg - Interventional Radiology in The Management of The Liver Transplant PatientSowmya ChitraNo ratings yet
- Klatskin Tumor 2Document8 pagesKlatskin Tumor 2Florian JeffNo ratings yet
- Ha SsDocument7 pagesHa SsSowmya ChitraNo ratings yet
- Review Article: Computed Tomography in The Evaluation For Transcatheter Aortic Valve Implantation (TAVI)Document13 pagesReview Article: Computed Tomography in The Evaluation For Transcatheter Aortic Valve Implantation (TAVI)Paul SchoenhagenNo ratings yet
- Hearts 02 00022Document10 pagesHearts 02 00022HannaTashiaClaudiaNo ratings yet
- AnnCardAnaesth15154-6423638 175036Document10 pagesAnnCardAnaesth15154-6423638 175036ElenaCondratscribdNo ratings yet
- Endovascular Treatment of Femoropopliteal Arterial Occlusive Disease - Current Techniques and LimitationsDocument10 pagesEndovascular Treatment of Femoropopliteal Arterial Occlusive Disease - Current Techniques and Limitationsafso afsoNo ratings yet
- 1 s2.0 S1078588406004801 Main PDFDocument8 pages1 s2.0 S1078588406004801 Main PDFkadek sanggingNo ratings yet
- AnnPediatrCard1138-2478932 065309Document8 pagesAnnPediatrCard1138-2478932 065309Binod KumarNo ratings yet
- Percutaneous Aortic Valve Implantation: The Anesthesiologist PerspectiveDocument11 pagesPercutaneous Aortic Valve Implantation: The Anesthesiologist Perspectiveserena7205No ratings yet
- Znad 431Document4 pagesZnad 431Asadullah khanNo ratings yet
- Pulmonary Artery Cannulation To Enhance Extracorporeal Membrane Oxygenation Management in Acute Cardiac FailureDocument8 pagesPulmonary Artery Cannulation To Enhance Extracorporeal Membrane Oxygenation Management in Acute Cardiac Failurejose lopeNo ratings yet
- 012011SCNA3Document14 pages012011SCNA3mariafmhNo ratings yet
- Abdalla 2002Document7 pagesAbdalla 2002Nikos SerifisNo ratings yet
- Exploración Del ColédocoDocument14 pagesExploración Del ColédocoJavier VegaNo ratings yet
- Curroncol 29 00553Document8 pagesCurroncol 29 00553Alex MariciucNo ratings yet
- Endoscopic Management of Complications From Laparoscopic Cholecystectomy - UpToDateDocument16 pagesEndoscopic Management of Complications From Laparoscopic Cholecystectomy - UpToDateLuis Miguel Díaz VegaNo ratings yet
- Vascular Surgery in Liver Resection: Olga Radulova Mauersberger Jürgen Weitz Carina RiedigerDocument32 pagesVascular Surgery in Liver Resection: Olga Radulova Mauersberger Jürgen Weitz Carina RiedigerariNo ratings yet
- Resection of Colorectal Liver Metastases: Ssat/Ahpba Joint Symposium 2010Document4 pagesResection of Colorectal Liver Metastases: Ssat/Ahpba Joint Symposium 2010Nikos SerifisNo ratings yet
- Argh - Ms.id.555581, DR Muhammad Zafar Mengal ArticlesDocument4 pagesArgh - Ms.id.555581, DR Muhammad Zafar Mengal ArticlesMuhammad Zafar MengalNo ratings yet
- International Journal of Surgery Case ReportsDocument4 pagesInternational Journal of Surgery Case Reportshussein_faourNo ratings yet
- Transplantation 2Document55 pagesTransplantation 2Shahansha Sharan DhammatiNo ratings yet
- Current Treatment of StricutresDocument4 pagesCurrent Treatment of StricutresAditya GNo ratings yet
- Tavr: TaviDocument3 pagesTavr: TaviPaul SchoenhagenNo ratings yet
- Ecr2011 C-0318Document11 pagesEcr2011 C-0318zulvaasNo ratings yet
- Technicalaspectsofbileduct Evaluationandexploration: Sean B. Orenstein,, Jeffrey M. Marks,, Jeffrey M. HardacreDocument16 pagesTechnicalaspectsofbileduct Evaluationandexploration: Sean B. Orenstein,, Jeffrey M. Marks,, Jeffrey M. HardacreBattousaih1No ratings yet
- Angioplasty and Stenting For Peripheral Arterial Disease of The Lower LimbsDocument13 pagesAngioplasty and Stenting For Peripheral Arterial Disease of The Lower Limbsnadia shabriNo ratings yet
- 2021 ArticleDocument9 pages2021 ArticlePNo ratings yet
- Complicacion BrickerDocument17 pagesComplicacion BrickerMCFNo ratings yet
- Ureteral Stent For Ureteral Stricture: James F. Borin and Elspeth M. McdougallDocument13 pagesUreteral Stent For Ureteral Stricture: James F. Borin and Elspeth M. McdougallOoNo ratings yet
- ExtendedRightHepatectomyinaLiverwithaNon-bifurcatingPortalVein theHangingManeuverProtectsthePortalSysteminthePresenceofAnomaliesDocument7 pagesExtendedRightHepatectomyinaLiverwithaNon-bifurcatingPortalVein theHangingManeuverProtectsthePortalSysteminthePresenceofAnomaliesMARIO DCARLO TREJO HUAMANNo ratings yet
- 1 s2.0 S1556858X12000394 MainDocument13 pages1 s2.0 S1556858X12000394 MainHaya RihanNo ratings yet
- International Journal of Surgery: SciencedirectDocument7 pagesInternational Journal of Surgery: SciencedirectFerdian PriantoNo ratings yet
- CTO Retrograde TechniqueDocument11 pagesCTO Retrograde TechniqueNiranjan ReddyNo ratings yet
- Case Series OutcomeDocument5 pagesCase Series OutcomeSowmya ANo ratings yet
- Trauma Hepatico Manejo 2017Document9 pagesTrauma Hepatico Manejo 2017alyss yasminNo ratings yet
- Budd Chiari SyndromeDocument37 pagesBudd Chiari SyndromeNader SaadNo ratings yet
- Factors Causing Prolonged Mechanical Ventilation and Peri Operative Morbidity After Robot Assisted Coronary Artery Bypass Graft SurgeryDocument8 pagesFactors Causing Prolonged Mechanical Ventilation and Peri Operative Morbidity After Robot Assisted Coronary Artery Bypass Graft SurgeryApotik ApotekNo ratings yet
- Trauma Pelvico Empaquetamiento Vs Embolizacion PDFDocument10 pagesTrauma Pelvico Empaquetamiento Vs Embolizacion PDFscribdleonpepeNo ratings yet
- 10.1007@s00261 019 02340 5Document25 pages10.1007@s00261 019 02340 5Pablo Henrique Alves TelesNo ratings yet
- Liver TransplantDocument5 pagesLiver TransplantMaxWittNo ratings yet
- Anesthesiafor Hepatobiliarysurgery: Chris Snowden,, James PrentisDocument17 pagesAnesthesiafor Hepatobiliarysurgery: Chris Snowden,, James PrentisGiovanni AgugginiNo ratings yet
- 2D 3D TEE Transcatheter Guiding With LAA ThrombusDocument16 pages2D 3D TEE Transcatheter Guiding With LAA ThrombusBosman AriestaNo ratings yet
- ChemoemboDocument10 pagesChemoemboAndre HartonoNo ratings yet
- Closure of Loop Ileostomy Potentially ADocument7 pagesClosure of Loop Ileostomy Potentially Ashah hassaanNo ratings yet
- Transcatheter Mitral Valve-in-Valve Therapy: Jose F. Condado,, Brian Kaebnick,, Vasilis BabaliarosDocument7 pagesTranscatheter Mitral Valve-in-Valve Therapy: Jose F. Condado,, Brian Kaebnick,, Vasilis BabaliarosA Pradana HNo ratings yet
- Laparoscopic Splenectomy: Standardized ApproachDocument9 pagesLaparoscopic Splenectomy: Standardized ApproachLauraNo ratings yet
- Current Aspects of The Surgical Management of Organ-Confined, Metastatic, and Recurrent Renal Cell CancerDocument7 pagesCurrent Aspects of The Surgical Management of Organ-Confined, Metastatic, and Recurrent Renal Cell CancermssfadNo ratings yet
- 26 Short-Term Outcomes Following The Use of Self-Expanding Metallic Stents in Acute Malignant Colonic Obstruction e A Single Centre ExperienceDocument5 pages26 Short-Term Outcomes Following The Use of Self-Expanding Metallic Stents in Acute Malignant Colonic Obstruction e A Single Centre ExperienceJoao FonsecaNo ratings yet
- The Liver Graft Before Transplantation: Defining Outcome After Liver TransplantationFrom EverandThe Liver Graft Before Transplantation: Defining Outcome After Liver TransplantationXavier VerhelstNo ratings yet
- Liver Transplantation - 2017 - Thornburg - Interventional Radiology in The Management of The Liver Transplant PatientDocument14 pagesLiver Transplantation - 2017 - Thornburg - Interventional Radiology in The Management of The Liver Transplant PatientSowmya ChitraNo ratings yet
- PDF PreviewDocument9 pagesPDF PreviewSowmya ChitraNo ratings yet
- Ha SsDocument7 pagesHa SsSowmya ChitraNo ratings yet
- Rescue Thrombectomy For Early Hepatic Artery Thrombosis Using Stent Retriever in A Child Post Combined Deceased Donor Liver and Renal TransplantDocument3 pagesRescue Thrombectomy For Early Hepatic Artery Thrombosis Using Stent Retriever in A Child Post Combined Deceased Donor Liver and Renal TransplantSowmya ChitraNo ratings yet
- Shell Helix HX5 15W 40 TDS PDFDocument2 pagesShell Helix HX5 15W 40 TDS PDFhoussem houssemNo ratings yet
- Nurs FPX 4040 Assessment 2 Protected Health Information Phi Privacy Security and Confidentiality Best PracticeDocument5 pagesNurs FPX 4040 Assessment 2 Protected Health Information Phi Privacy Security and Confidentiality Best Practicejoohnsmith070No ratings yet
- Unit 1 - Health Psychology - More On Health Behaviour and TheoriesDocument24 pagesUnit 1 - Health Psychology - More On Health Behaviour and TheoriesSheeba ShamsudeenNo ratings yet
- Daftar Pustaka AsDocument1 pageDaftar Pustaka AsIchsanQuswainNo ratings yet
- Crew Size Simulation Cardiac Arrest TapiaiDocument12 pagesCrew Size Simulation Cardiac Arrest TapiaiJamison ParfittNo ratings yet
- Biotech SyllabusDocument2 pagesBiotech Syllabusmeet2abhayNo ratings yet
- View of Therapeutic Efficacy of VarmamDocument8 pagesView of Therapeutic Efficacy of VarmamMariana SantosNo ratings yet
- Time Management Training by Lisa J DownsDocument6 pagesTime Management Training by Lisa J DownssoberNo ratings yet
- Master Validation Plan SOP and Approval TemplateDocument7 pagesMaster Validation Plan SOP and Approval Templatesiva sankarNo ratings yet
- A - Pratic Guide Pediatric Wound CareDocument9 pagesA - Pratic Guide Pediatric Wound CareLicia GabrielleNo ratings yet
- My Research ArticleDocument7 pagesMy Research ArticleclimedNo ratings yet
- Rencana Anggaran Seksi KesehatanDocument1 pageRencana Anggaran Seksi KesehatantinamirnawatitambaNo ratings yet
- SAMDocument108 pagesSAMAlimyon Abilar MontoloNo ratings yet
- ProRox SDS PDFDocument7 pagesProRox SDS PDFr afriantoNo ratings yet
- Murphy V LamontDocument34 pagesMurphy V LamontHoward FriedmanNo ratings yet
- Sika Line Marking PaintDocument7 pagesSika Line Marking Paintfaisal nadeemNo ratings yet
- 5 Ways To Focus at Work, From An Executive Who's Struggled With ADHDDocument5 pages5 Ways To Focus at Work, From An Executive Who's Struggled With ADHDtinaNo ratings yet
- PANAMA CANAL AUTHORITY ACP Maritime OperDocument70 pagesPANAMA CANAL AUTHORITY ACP Maritime Operagus nurcahyoNo ratings yet
- Mosquito Repellent Property of Ylang YlangDocument9 pagesMosquito Repellent Property of Ylang YlangR RenegadeNo ratings yet
- 5S Japanese Ways To SuccessDocument39 pages5S Japanese Ways To SuccessNerizza SomeraNo ratings yet
- Contoh Review GarciniaDocument8 pagesContoh Review GarciniamarwahNo ratings yet
- Presentation Material: Targeted at Employees in Testing FactoriesDocument10 pagesPresentation Material: Targeted at Employees in Testing FactoriesAhmed ElsawyNo ratings yet
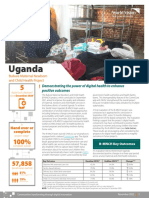
- 2021 Digital Health Factsheet - B-MNCH - UgandaDocument2 pages2021 Digital Health Factsheet - B-MNCH - UgandaMd UmerNo ratings yet
- Lifestyle ModificationDocument48 pagesLifestyle ModificationPGI MANALILI MARIA DIANANo ratings yet
- Internal Medicine Journal - 2020 - Gilmore - Cytomegalovirus in Inflammatory Bowel Disease A Clinical ApproachDocument4 pagesInternal Medicine Journal - 2020 - Gilmore - Cytomegalovirus in Inflammatory Bowel Disease A Clinical ApproachDiego Fernando Ortiz TenorioNo ratings yet