You might also like
- Computerised Payroll Practice Set Using MYOB AccountRight: Australian EditionFrom EverandComputerised Payroll Practice Set Using MYOB AccountRight: Australian EditionNo ratings yet
- VRIO AnalysisDocument2 pagesVRIO AnalysisrenjuannNo ratings yet
- Official Business Trip AuthorizationDocument5 pagesOfficial Business Trip AuthorizationJake MadzNo ratings yet
- Timesheet March 26 To April 9, 2017Document3 pagesTimesheet March 26 To April 9, 2017Joseph Clavano JimenezNo ratings yet
- Formulario 1604-1 Constancia de Alta Del Trabajador: EmpleadorDocument2 pagesFormulario 1604-1 Constancia de Alta Del Trabajador: EmpleadorFlor ArevaloNo ratings yet
- DTR - Aug 16-31, 2019Document25 pagesDTR - Aug 16-31, 2019anon_836445344No ratings yet
- A-03 Leave Application Form TitleDocument2 pagesA-03 Leave Application Form TitleDesti Nur Asyifa DahwantiNo ratings yet
- Register of InjuryDocument3 pagesRegister of InjurypenichopsNo ratings yet
- Revise Ob FormDocument1 pageRevise Ob FormJake MadzNo ratings yet
- Amrita Medical Leave FormDocument1 pageAmrita Medical Leave FormApoorv MahajanNo ratings yet
- ER-PA-rev02: Timekeeping FormDocument3 pagesER-PA-rev02: Timekeeping Formjef comendadorNo ratings yet
- Application For Leave of Absence: (To Be Submitted Before Actually Taking Leave)Document5 pagesApplication For Leave of Absence: (To Be Submitted Before Actually Taking Leave)Maricor MontemorNo ratings yet
- Coa 4.24.2023 PDFDocument2 pagesCoa 4.24.2023 PDFKeycelyn C. SampangNo ratings yet
- NOV 9-NOV 23 Date Morning Afternoon Regular Hours OvertimeDocument10 pagesNOV 9-NOV 23 Date Morning Afternoon Regular Hours OvertimeJollinaNo ratings yet
- SopDocument4 pagesSopJed Samar ManzanillaNo ratings yet
- GOVERNMENT Leave - Form - Complete2Document2 pagesGOVERNMENT Leave - Form - Complete2Marc CaurelNo ratings yet
- Leave FormsDocument1 pageLeave FormsAmadonz Vallespin LlamedoNo ratings yet
- Daily Time Record: Legal SpecialDocument3 pagesDaily Time Record: Legal SpecialJomar LaucNo ratings yet
- Employee Information Sheet: Vivo South Luzon IncDocument5 pagesEmployee Information Sheet: Vivo South Luzon IncRene ChuaNo ratings yet
- Leave Application: 509964187 Procrement Dep. USF-M-020 2329343558 USF 阿美安全设施升级改 造项目Document1 pageLeave Application: 509964187 Procrement Dep. USF-M-020 2329343558 USF 阿美安全设施升级改 造项目Mohamed SolimanNo ratings yet
- New SSG Vacation FormDocument1 pageNew SSG Vacation FormDiego AlvaradoNo ratings yet
- Overtime Request Form 加班申请表: Last Name First NameDocument7 pagesOvertime Request Form 加班申请表: Last Name First NameOlan PrinceNo ratings yet
- Loa July 3, 2021Document1 pageLoa July 3, 2021Daniel AmbrocioNo ratings yet
- Leave FormDocument1 pageLeave FormMohit Kumar ChowdaryNo ratings yet
- Leave Application Form: To Be Filled-Out by EmployeeDocument4 pagesLeave Application Form: To Be Filled-Out by EmployeeNonjTreborTendenillaToltolNo ratings yet
- DTR Sample - Excel SubmissionDocument8 pagesDTR Sample - Excel SubmissionJulina AredidonNo ratings yet
- HR 007 Rev A - Leave Availment Form - BLANK1Document1 pageHR 007 Rev A - Leave Availment Form - BLANK1Jashper Jed CornelNo ratings yet
- Cir Mod Tra 20608027816 45924736 06112023144641Document2 pagesCir Mod Tra 20608027816 45924736 06112023144641MIGUEL LEONNo ratings yet
- Absence Request: Type of Absence Request: Lateness / Home Early Sick Personal Leave MaternityDocument1 pageAbsence Request: Type of Absence Request: Lateness / Home Early Sick Personal Leave MaternitylintangNo ratings yet
- Weekly timesheet tracking hours, breaks and overtimeDocument14 pagesWeekly timesheet tracking hours, breaks and overtimeArun KumarNo ratings yet
- Bosch PrioDocument2 pagesBosch PriojairofrNo ratings yet
- FULL AND FINAL SETTLEMENT - RachnaDocument3 pagesFULL AND FINAL SETTLEMENT - Rachnapooja sankhalaNo ratings yet
- Annual Leave NewDocument6 pagesAnnual Leave NewRoslaini YoNo ratings yet
- CFGV Leave FormDocument1 pageCFGV Leave FormhafizNo ratings yet
- Leave Application FormDocument1 pageLeave Application Formfairoos aliNo ratings yet
- Sick Benefit Ronny Sierra 1 JuneDocument2 pagesSick Benefit Ronny Sierra 1 JunedababyhyprNo ratings yet
- Leave Application FormDocument5 pagesLeave Application FormtalhaNo ratings yet
- Leave Application Form: M/S.Ese Powercon PVT LTDDocument1 pageLeave Application Form: M/S.Ese Powercon PVT LTDuttam mishraNo ratings yet
- Appoinment Doktor: Employee DetailsDocument1 pageAppoinment Doktor: Employee Detailszaid hasanNo ratings yet
- WireWheel Short Term DisabilityDocument7 pagesWireWheel Short Term DisabilitySteve MooreNo ratings yet
- OBFormDocument1 pageOBFormargelNo ratings yet
- Individual Workweek Accomplishment Report Template 1Document2 pagesIndividual Workweek Accomplishment Report Template 1YeyebonlNo ratings yet
- Leave Application FormDocument1 pageLeave Application FormtalhaNo ratings yet
- MemberCardDocument2 pagesMemberCardvikash pandeyNo ratings yet
- Treasury Assistant Timesheet and Overtime RecordsDocument3 pagesTreasury Assistant Timesheet and Overtime RecordsGyra Maturan UrbiztondoNo ratings yet
- LEAVE-FORM-2 (1)Document7 pagesLEAVE-FORM-2 (1)Kean Hart D. BlancoNo ratings yet
- Leave Application Form ApprovalDocument1 pageLeave Application Form Approvaldkc blueNo ratings yet
- Locations Job Application-061121Document2 pagesLocations Job Application-061121Ain FaeiqaNo ratings yet
- Staff Leave Application Form: Staff No. Full Name Dept. Line SuperiorDocument3 pagesStaff Leave Application Form: Staff No. Full Name Dept. Line SuperiorSamiracomputerstation Kuya MarvsNo ratings yet
- Labor Department Application Alien RegistrationDocument4 pagesLabor Department Application Alien RegistrationRetchh Ihsel De TorresNo ratings yet
- DTR Sample - Excel SubmissionDocument10 pagesDTR Sample - Excel SubmissionJulina AredidonNo ratings yet
- Jioint Declaration FormDocument1 pageJioint Declaration FormRohit GuptaNo ratings yet
- Mea NoaiaDocument4 pagesMea NoaiaTaniela FuataimiNo ratings yet
- Official Business/ Reimbursement/ Liquidation ReportDocument3 pagesOfficial Business/ Reimbursement/ Liquidation ReportKin Pearly FloresNo ratings yet
- Leave Application Form (NEW)Document2 pagesLeave Application Form (NEW)AhmedNo ratings yet
- Dustin ByrdDocument3 pagesDustin Byrdapi-3825833No ratings yet
- Leave application formDocument1 pageLeave application formsantosh meenaNo ratings yet
- Customer service timesheetDocument1 pageCustomer service timesheetSean Rhay ComiaNo ratings yet
- Member CardDocument3 pagesMember CardthirumalarajuNo ratings yet
- Flow of Checking Home Quarantine of Employees That Will Report StartingDocument3 pagesFlow of Checking Home Quarantine of Employees That Will Report StartingJoyce AntoinetteNo ratings yet
- Mahal ModuleDocument2 pagesMahal ModuleJoseph Clavano JimenezNo ratings yet
- Release NoteDocument2 pagesRelease NoteJoseph Clavano JimenezNo ratings yet
- ThankyouDocument1 pageThankyouLe ThangNo ratings yet
- 656Document1 page656Joseph Clavano JimenezNo ratings yet
- Release NoteDocument2 pagesRelease NoteJoseph Clavano JimenezNo ratings yet
- Budget For TodayDocument1 pageBudget For TodayJoseph Clavano JimenezNo ratings yet
- RESEARCH PARA SA BAHAY KUBONG MABAHO12312312312312312312423RFASFgacsDFVS DFGASDFSDFDocument1 pageRESEARCH PARA SA BAHAY KUBONG MABAHO12312312312312312312423RFASFgacsDFVS DFGASDFSDFJoseph Clavano JimenezNo ratings yet
- Budget For TodayDocument1 pageBudget For TodayJoseph Clavano JimenezNo ratings yet
- ThankyouDocument1 pageThankyouLe ThangNo ratings yet
- ReadmeDocument1 pageReadmeAfsar AfsarNo ratings yet
- Research para Sa Bahay Kubong MabahoDocument1 pageResearch para Sa Bahay Kubong MabahoJoseph Clavano JimenezNo ratings yet
- SDALKJGSHLCRNIQAWU30947-23094=2134129+38+1283+1623+19273+9A5CSD96FVCASDCFQW3$!@#$@!#%#%$!@#$%#@#!#@$^@!#!@$rcPOASFNUVALDSIRUNCFASDYFCJWKLDHYFHVKWCUHYVKXUFYVQWCIRUYQCIKSJFVCSJKZDUHJVFWISUDHYVSJOTAOWPORF7G8AH89GROA.docxDocument1 pageSDALKJGSHLCRNIQAWU30947-23094=2134129+38+1283+1623+19273+9A5CSD96FVCASDCFQW3$!@#$@!#%#%$!@#$%#@#!#@$^@!#!@$rcPOASFNUVALDSIRUNCFASDYFCJWKLDHYFHVKWCUHYVKXUFYVQWCIRUYQCIKSJFVCSJKZDUHJVFWISUDHYVSJOTAOWPORF7G8AH89GROA.docxJoseph Clavano JimenezNo ratings yet
- Monthly cash advance trackingDocument2 pagesMonthly cash advance trackingJoseph Clavano JimenezNo ratings yet
- RESEARCHDocument1 pageRESEARCHJoseph Clavano JimenezNo ratings yet
- RESEARCHDocument1 pageRESEARCHJoseph Clavano JimenezNo ratings yet
- AasdDocument3 pagesAasdJoseph Clavano JimenezNo ratings yet
- The University of ManilaDocument1 pageThe University of ManilaJoseph Clavano JimenezNo ratings yet
- NEEDINKDocument149 pagesNEEDINKJoseph Clavano JimenezNo ratings yet
- Total Sahod Month Total Sahod Month Total Sahod Month Total Sahod MonthDocument2 pagesTotal Sahod Month Total Sahod Month Total Sahod Month Total Sahod MonthJoseph Clavano JimenezNo ratings yet
- Marketing NetflixDocument17 pagesMarketing NetflixAshley LoyolaNo ratings yet
- People ManagementDocument12 pagesPeople Managementyater32875100% (1)
- "Financial Statement Analysis": A Project Report OnDocument6 pages"Financial Statement Analysis": A Project Report OnRahul GordeNo ratings yet
- TQMDocument13 pagesTQMUmair Moin100% (1)
- Topic 6 - ADS 404 Chapter 6 2018Document25 pagesTopic 6 - ADS 404 Chapter 6 2018Nabil Azeem JehanNo ratings yet
- Chlor Alkali-2Document12 pagesChlor Alkali-2Tadesse ZerihunNo ratings yet
- South Africa'S de Beers: The Most Unethical Corporation in The WorldDocument11 pagesSouth Africa'S de Beers: The Most Unethical Corporation in The WorldFarida JaskaniNo ratings yet
- Chapter 1 The Nature and Scope of Marketing Part 1Document32 pagesChapter 1 The Nature and Scope of Marketing Part 1maghagxxxNo ratings yet
- Carlson School Corporate Investment Decisions Spring 2017Document12 pagesCarlson School Corporate Investment Decisions Spring 2017Novriani Tria PratiwiNo ratings yet
- How Schindler Group Elevated Performance in Its Corporate CultureDocument4 pagesHow Schindler Group Elevated Performance in Its Corporate Cultureshivangi guptaNo ratings yet
- Brief Background About DruckerDocument4 pagesBrief Background About DruckerTabitha WatsaiNo ratings yet
- PGP 1 Group M2 Improves Maya SalesDocument4 pagesPGP 1 Group M2 Improves Maya SalesApoorva SharmaNo ratings yet
- Floor SupervisorDocument3 pagesFloor SupervisorJohn Carlo BautistaNo ratings yet
- 7 Final Accounts of CompaniesDocument15 pages7 Final Accounts of CompaniesAakshi SharmaNo ratings yet
- Strategic and Tactical Marketing ProcessDocument106 pagesStrategic and Tactical Marketing ProcessFadilla Wanda NaseroNo ratings yet
- 2023 Mentorship GEMS ?Document25 pages2023 Mentorship GEMS ?Takunda Elseworth Nyuke100% (1)
- Test Series: March, 2022 Mock Test Paper 1 Foundation Course Paper - 1: Principles and Practice of AccountingDocument5 pagesTest Series: March, 2022 Mock Test Paper 1 Foundation Course Paper - 1: Principles and Practice of AccountingVinithaNo ratings yet
- Form 6 Leave Application FormDocument2 pagesForm 6 Leave Application FormROBERTO RUBEN PULGANo ratings yet
- Business Ethics AssignmentDocument17 pagesBusiness Ethics AssignmentsevinchNo ratings yet
- Maintenance of Machinery & PlantsDocument22 pagesMaintenance of Machinery & PlantszeldotdotNo ratings yet
- PSSC Computer Studies QPDocument19 pagesPSSC Computer Studies QPAndrew ArahaNo ratings yet
- Enhancing Container Terminal Productivity: A Co-Maker Approach Between Carriers and OperatorsDocument3 pagesEnhancing Container Terminal Productivity: A Co-Maker Approach Between Carriers and OperatorsAdn AdinaNo ratings yet
- Sistem Informasi Manajemen Presensi Siswa Berbasis MobileDocument6 pagesSistem Informasi Manajemen Presensi Siswa Berbasis Mobilefahmi nur baihaqiNo ratings yet
- Ethics in Business 1Document7 pagesEthics in Business 1Hana 64No ratings yet
- Mobile App Development Proposal: Prepared ForDocument7 pagesMobile App Development Proposal: Prepared ForSultan KingNo ratings yet
- Taxation of Business IncomeDocument15 pagesTaxation of Business Incomekitderoger_391648570No ratings yet
- BMKT300 Revision 2Document8 pagesBMKT300 Revision 2Jana MizherNo ratings yet
- Amazon InvoiceDocument1 pageAmazon InvoiceSyprotech SolutionsNo ratings yet
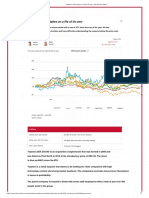
- Teqnion's Stock Takes On A Life of Its Own: TechnionDocument9 pagesTeqnion's Stock Takes On A Life of Its Own: TechnionDaniel ZhangNo ratings yet