You might also like
- Certificate of Creditable Tax Withheld at Source: Redil, AngelikaDocument2 pagesCertificate of Creditable Tax Withheld at Source: Redil, AngelikaAngelika Plaza RedilNo ratings yet
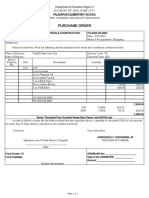
- PurchaseOrder-raq PrincipalDocument1 pagePurchaseOrder-raq PrincipalTheresa Faye De GuzmanNo ratings yet
- Job CompletedDocument11 pagesJob CompletedalsyyedipakistanNo ratings yet
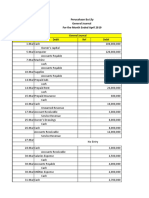
- LedgerDocument3 pagesLedgerGUI DING QUAN MoeNo ratings yet
- Soon KitDocument1 pageSoon KitJun Yi YapNo ratings yet
- Transaction Journal - 090Document1 pageTransaction Journal - 090Meila Fauziah AryaniNo ratings yet
- Solutions To Text Book Exercises: 1. Interest Tables Method: Solution - 1Document10 pagesSolutions To Text Book Exercises: 1. Interest Tables Method: Solution - 1M JEEVARATHNAM NAIDUNo ratings yet
- Paper 7A Direct TaxDocument18 pagesPaper 7A Direct Taxdeshmukh.tanvi090No ratings yet
- Volume V 2Document21 pagesVolume V 2Balu Mahendra SusarlaNo ratings yet
- Cert 2307V2018 InnoveDocument1 pageCert 2307V2018 InnoveLeo BagtasNo ratings yet
- Certificate of Creditable Tax Withheld at Source: San Fermin, Cauayan City, IsabelaDocument8 pagesCertificate of Creditable Tax Withheld at Source: San Fermin, Cauayan City, IsabelaRV Truck and Heavy Equipment Parts SupplyNo ratings yet
- Accrue WW May23Document9 pagesAccrue WW May23gudangasta321 asta321No ratings yet
- 220213190-Fajar Arnas - Slip Gaji April 2023Document1 page220213190-Fajar Arnas - Slip Gaji April 2023bengaklolo92No ratings yet
- Ewt Form For Parts MalolosDocument5 pagesEwt Form For Parts MalolosSKYGO MALOLOSNo ratings yet
- LNL Iklcqd /: Employee Share Employer Share Employee Share Employer ShareDocument2 pagesLNL Iklcqd /: Employee Share Employer Share Employee Share Employer ShareAman DesaiNo ratings yet
- 2307 ISECO CalumbayaDocument62 pages2307 ISECO Calumbayaleo BacuadenNo ratings yet
- Dein Sanctuary Company, Ltd. (PERFORMANCE TASK-PRELIM)Document17 pagesDein Sanctuary Company, Ltd. (PERFORMANCE TASK-PRELIM)Epril RamonedaNo ratings yet
- Book 2Document4 pagesBook 2Anjali DubeyNo ratings yet
- (ANSWER) - 02 - The Recording ProcessDocument12 pages(ANSWER) - 02 - The Recording ProcessdeltakoNo ratings yet
- CRDocument100 pagesCRTeamNo ratings yet
- Eliza C. Antonio Gen. Merchandize 2306 207Document8 pagesEliza C. Antonio Gen. Merchandize 2306 207Jessica CrisostomoNo ratings yet
- APV 139375 PO 7069 Amigo Import & Export Corp Ver2Document6 pagesAPV 139375 PO 7069 Amigo Import & Export Corp Ver2Eniger CaspeNo ratings yet
- General Ledger (Detail) - 5Document7 pagesGeneral Ledger (Detail) - 5Riski Nack OutsiderNo ratings yet
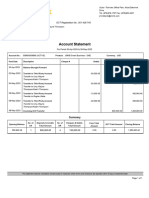
- StatementDocument1 pageStatementDominicNo ratings yet
- Loan Account Statement Details: Generated byDocument7 pagesLoan Account Statement Details: Generated byMd. Shahidul Islam PkNo ratings yet
- Assignment 03 Tam3535-Management Studies: R.A.D.S.Niwarthana Center-Colombo DUE-DATE-12/13/2022Document7 pagesAssignment 03 Tam3535-Management Studies: R.A.D.S.Niwarthana Center-Colombo DUE-DATE-12/13/2022K.A.S.A.pierisNo ratings yet
- Activity 25 - Journal Entry To Post-ClosingDocument23 pagesActivity 25 - Journal Entry To Post-ClosingAdam Cuenca100% (1)
- BNK #0923-049 - Onboarding Manager's Fee - Sep 2023 - Angel Antonio - 35,000.00Document5 pagesBNK #0923-049 - Onboarding Manager's Fee - Sep 2023 - Angel Antonio - 35,000.00Rojay Ignacio IINo ratings yet
- MAA AssignmentDocument13 pagesMAA AssignmenthemanshaNo ratings yet
- Barangay SupportingDocument29 pagesBarangay SupportingJans CastroNo ratings yet
- 347 School Office Supplies IncDocument2 pages347 School Office Supplies IncBen Carlo RamosNo ratings yet
- Business Account Statement 2022Document5 pagesBusiness Account Statement 2022mrgrayinthedarkNo ratings yet
- Maria Concepcion Julian 2307 - EWT Computation June2019Document2 pagesMaria Concepcion Julian 2307 - EWT Computation June2019ReinapotNo ratings yet
- Statement of Account Central Bank of India: Mr. Aniket Bhardwaj - Account No.: 3998318164Document1 pageStatement of Account Central Bank of India: Mr. Aniket Bhardwaj - Account No.: 3998318164Anju Manish BhardwajNo ratings yet
- Statement Showing Particulars of Claims by An Employee For Deduction of Tax Under Section 192Document2 pagesStatement Showing Particulars of Claims by An Employee For Deduction of Tax Under Section 192Mayank JainNo ratings yet
- Acknowledgment of Debt - TrozadoDocument3 pagesAcknowledgment of Debt - TrozadoJP VillanuevaNo ratings yet
- Ledger Details21 Dec 2023 215Document3 pagesLedger Details21 Dec 2023 215Manasa B.P.No ratings yet
- Wesel TagihDocument7 pagesWesel TagihMuhammad Fallah100% (1)
- 2307 Jan 2018 ENCS v3 SignedDocument2 pages2307 Jan 2018 ENCS v3 SignedStanleyMarkPardiñanLazagaNo ratings yet
- Transaction History Permata PagingDocument1 pageTransaction History Permata PagingHendra HendraNo ratings yet
- Answer To The Question No. 1 (A) General JournalDocument16 pagesAnswer To The Question No. 1 (A) General JournalSurmaNo ratings yet
- Account Transactions (Accrual)Document1 pageAccount Transactions (Accrual)HeriNo ratings yet
- Account Transactions (Accrual) BB Bank MuamalahDocument2 pagesAccount Transactions (Accrual) BB Bank MuamalahHeriNo ratings yet
- PT Milineal Sentosa: Pro Forma InvoiceDocument4 pagesPT Milineal Sentosa: Pro Forma InvoicethaniaNo ratings yet
- Principles of Accounting: Individual AssignmentDocument9 pagesPrinciples of Accounting: Individual AssignmentHuynh Minh Tien (K16HCM)No ratings yet
- Emp Annual Statement-2Document1 pageEmp Annual Statement-2shivamrajsingh12042001No ratings yet
- C Ertificate of Creditable Tax W Ithheld at Source C Ertificate of Creditable Tax W Ithheld at SourceDocument3 pagesC Ertificate of Creditable Tax W Ithheld at Source C Ertificate of Creditable Tax W Ithheld at SourceVher Christopher Ducay0% (1)
- 5 DepDocument2 pages5 Depshreyash436No ratings yet
- 2307 Jan 2018 ENCS v3Document2 pages2307 Jan 2018 ENCS v3Mark Patrics Comentan VerderaNo ratings yet
- Chap # 3 (P3-1a) (P3-2a)Document18 pagesChap # 3 (P3-1a) (P3-2a)Råjà Āhsán BràndNo ratings yet
- P2 2A Financial AccountingDocument12 pagesP2 2A Financial AccountingFerris126GTNo ratings yet
- Sec Header Tax Component Declarations (INR) Proof (INR) Cleared (INR) Rejected (INR) RemarksDocument2 pagesSec Header Tax Component Declarations (INR) Proof (INR) Cleared (INR) Rejected (INR) RemarksJogesh KumarNo ratings yet
- Ravina Ivy Mirzi-092921Document1 pageRavina Ivy Mirzi-092921YviIrzimPascualAntipatiaNo ratings yet
- 2307 - Regan IndustrialDocument1 page2307 - Regan IndustrialbadethvillafuertetangcayNo ratings yet
- (Last Name, Given Name, Middle Name) : Fundamentals of AccountingDocument4 pages(Last Name, Given Name, Middle Name) : Fundamentals of AccountingDe chavez, John carlo R.No ratings yet
- Republic of The Philippines Schedule of Advances To Officers & EmployeesDocument10 pagesRepublic of The Philippines Schedule of Advances To Officers & EmployeesDilg LuponNo ratings yet
- Ledger 23 07 1Document10 pagesLedger 23 07 1Arman AhmedNo ratings yet
- Latmark StructureDocument33 pagesLatmark StructureJealousy MarumisaNo ratings yet
- Chap14 The Calculation & Interpretation of Accounting RatiosDocument6 pagesChap14 The Calculation & Interpretation of Accounting RatiosSaiful AliNo ratings yet
- CH 5 6 Capital BudgetingDocument94 pagesCH 5 6 Capital BudgetingNikita AggarwalNo ratings yet
- No Description Qty Unit Price Disc Mig Torch Euro Type: QuotationDocument3 pagesNo Description Qty Unit Price Disc Mig Torch Euro Type: QuotationReneoNo ratings yet
- OM Session 3Document38 pagesOM Session 3mayra salirrosasNo ratings yet
- GG METALKRAFTS, Moradabad: Missing Documents in BUSY Data (GSTR2)Document1 pageGG METALKRAFTS, Moradabad: Missing Documents in BUSY Data (GSTR2)HeliumByBGC AccountsNo ratings yet
- The Intercultural Challenges Faced by Tesco in PolandDocument16 pagesThe Intercultural Challenges Faced by Tesco in Polandgdrive0018No ratings yet
- Commercial Bank Research PaperDocument5 pagesCommercial Bank Research Paperjppawmrhf100% (1)
- BUS620 - Kishor Alo PDFDocument14 pagesBUS620 - Kishor Alo PDFAmina MatinNo ratings yet
- Finance DossierDocument108 pagesFinance DossierAbhishek VarshneyNo ratings yet
- Agec 343 - Farm Management PrinciplesDocument38 pagesAgec 343 - Farm Management PrinciplesKenani WycliffeNo ratings yet
- MGT400 Individual AssignmentDocument9 pagesMGT400 Individual AssignmentNUR SABRINA RIDUANNo ratings yet
- Outline of MOSMS Practice Guide 2020Document32 pagesOutline of MOSMS Practice Guide 2020Pathy LNo ratings yet
- Example:: To Record Depreciation From - ToDocument21 pagesExample:: To Record Depreciation From - Todebate ddNo ratings yet
- Strategic ManagementDocument52 pagesStrategic ManagementDesmondNo ratings yet
- Time Preferences - 2023Document96 pagesTime Preferences - 2023zelekebelay647No ratings yet
- Parsons Fashion Business SyllabusDocument10 pagesParsons Fashion Business SyllabusJawanNo ratings yet
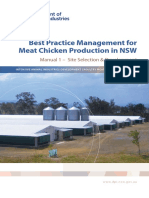
- BPM For Meat Chicken Production in NSW Manual 1Document86 pagesBPM For Meat Chicken Production in NSW Manual 1MohamedNo ratings yet
- 7 Steps To Proctorize Your Budget and Change Your LifeDocument1 page7 Steps To Proctorize Your Budget and Change Your LifeCristina Gazner CristescuNo ratings yet
- Determinants of Brand Equity in Hair Care Products An Empirical StudyDocument20 pagesDeterminants of Brand Equity in Hair Care Products An Empirical StudychaubeydsNo ratings yet
- DQS258 - Chapter 4 WoodworkDocument29 pagesDQS258 - Chapter 4 WoodworkFauzan FikhriNo ratings yet
- ROGERS PDF Jake Thompson's Daily Scorecard 2020Document1 pageROGERS PDF Jake Thompson's Daily Scorecard 2020xoNo ratings yet
- G. Maier, Pauline The Revolutionary Origins of The American CorporationDocument35 pagesG. Maier, Pauline The Revolutionary Origins of The American CorporationjorgekmpoxNo ratings yet
- SPL Terms N Conditions For Phase III 270716Document12 pagesSPL Terms N Conditions For Phase III 270716Mahesh KumarNo ratings yet
- Accounting & Statistical ProceduresDocument52 pagesAccounting & Statistical ProceduresHesham AlabaniNo ratings yet
- Turn Your Sink: Into A SpaDocument19 pagesTurn Your Sink: Into A SpaLeo CabelosNo ratings yet
- Form VAT - 17: Return by A Registered PersonDocument3 pagesForm VAT - 17: Return by A Registered PersonYf WoonNo ratings yet
- Adaptive Trading Strategies Across Liquidity PoolsDocument47 pagesAdaptive Trading Strategies Across Liquidity PoolsChibuzor NkemdilimNo ratings yet
- Fascino MakeupDocument4 pagesFascino MakeupSamara Mendoza GrisalesNo ratings yet
- Big Data NotesDocument4 pagesBig Data NotesVivek KavtaNo ratings yet
- Directory of International Sales AgentsDocument25 pagesDirectory of International Sales AgentsAna De NevadoNo ratings yet