You might also like
- Themes in Romeo and JulietDocument7 pagesThemes in Romeo and JulietChiosa AdinaNo ratings yet
- Aerobic High-Intensity Intervals Improve 07Document7 pagesAerobic High-Intensity Intervals Improve 07Lindsay OrtizNo ratings yet
- Complete Guide To E-Commerce TechnologyDocument420 pagesComplete Guide To E-Commerce Technologypilatus100% (4)
- Gearbox Vibration Analysis - Forcing Frequencies: 16 Things Many Vibration Analysts Don't Do (But They Should)Document19 pagesGearbox Vibration Analysis - Forcing Frequencies: 16 Things Many Vibration Analysts Don't Do (But They Should)Pedro RosaNo ratings yet
- Cell Selection ReselectionDocument35 pagesCell Selection ReselectionThiaguNo ratings yet
- Pebc CompilationDocument14 pagesPebc CompilationAarti AroraNo ratings yet
- Maximize your fitness with VO2 maxDocument5 pagesMaximize your fitness with VO2 maxdick headNo ratings yet
- 10.1007 S004210050402 Changes in Performance Muscle Metabolites Enzymes and Fibre Types After Short Sprint TrainingDocument7 pages10.1007 S004210050402 Changes in Performance Muscle Metabolites Enzymes and Fibre Types After Short Sprint TrainingNaDer HamedChamanNo ratings yet
- Wasserman Chest 1997Document13 pagesWasserman Chest 1997Filip BreskvarNo ratings yet
- Tirfor: Lifting and Pulling Machines With Unlimited Wire RopeDocument26 pagesTirfor: Lifting and Pulling Machines With Unlimited Wire RopeGreg ArabazNo ratings yet
- Validity of 3 Protocols For Verifying VO2maxDocument5 pagesValidity of 3 Protocols For Verifying VO2maxAlvaro LopezNo ratings yet
- Compressors in Energy Transition: Cornerstones Filtration ComponentsDocument60 pagesCompressors in Energy Transition: Cornerstones Filtration ComponentscsrpirataNo ratings yet
- Pressure Transient Formation and Well Testing: Convolution, Deconvolution and Nonlinear EstimationFrom EverandPressure Transient Formation and Well Testing: Convolution, Deconvolution and Nonlinear EstimationRating: 2 out of 5 stars2/5 (1)
- Preparation, Characterization, Properties, and Application of NanofluidFrom EverandPreparation, Characterization, Properties, and Application of NanofluidNo ratings yet
- ACL GRC Risk Manager - Usage Guide V1.1Document28 pagesACL GRC Risk Manager - Usage Guide V1.1Rohit ShettyNo ratings yet
- Oxygen Uptake Kinetics During Treadmill Running Across Exercise Intensity DomainsDocument9 pagesOxygen Uptake Kinetics During Treadmill Running Across Exercise Intensity DomainsPaulo PiresNo ratings yet
- Relationship of Exercise Test Variables To Cycling Performance in An Ironman TriathlonDocument9 pagesRelationship of Exercise Test Variables To Cycling Performance in An Ironman TriathlonvictornevarezNo ratings yet
- Rockport Adulto JovenDocument11 pagesRockport Adulto JovenAlejandra VasquezNo ratings yet
- Beltz 2016Document13 pagesBeltz 2016Einar Cumplido MartínezNo ratings yet
- 2013 BERTUZZI Energy System Contributions During Incremental Exercise TestDocument7 pages2013 BERTUZZI Energy System Contributions During Incremental Exercise TestEduardo de SouzaNo ratings yet
- The Sustainability of Vo2maxDocument12 pagesThe Sustainability of Vo2maxkullNo ratings yet
- Clint R. Bellenger Et - Al, 2015 - Predicting Maximal Aerobic Speed Through Set Distance Time-TrialsDocument9 pagesClint R. Bellenger Et - Al, 2015 - Predicting Maximal Aerobic Speed Through Set Distance Time-Trialsok okNo ratings yet
- Alterations in VO2max and The VO2 Plateau With Manipulation of Sampling IntervalDocument8 pagesAlterations in VO2max and The VO2 Plateau With Manipulation of Sampling IntervalvovaatanasovNo ratings yet
- Is The VO Max That We Measure Really Maximal?: Bruno P. C. Smirmaul, Danilo R. Bertucci and Inaian P. TeixeiraDocument4 pagesIs The VO Max That We Measure Really Maximal?: Bruno P. C. Smirmaul, Danilo R. Bertucci and Inaian P. TeixeiraHari25885No ratings yet
- JEP Journal of Exercise Physiology: OnlineDocument8 pagesJEP Journal of Exercise Physiology: OnlineMuthu GopalNo ratings yet
- Multi-Stage 20-m Shuttle Run Fitness Test, Maximal Oxygen Uptake and Velocity at Maximal Oxygen UptakeDocument7 pagesMulti-Stage 20-m Shuttle Run Fitness Test, Maximal Oxygen Uptake and Velocity at Maximal Oxygen UptakeAlifa Diar UtamieNo ratings yet
- Helgerund (Estudio Intervalos)Document7 pagesHelgerund (Estudio Intervalos)Andres PdrejnNo ratings yet
- Validation of An Arm Crank Ergometer Test For Use in Sedentary AdultsDocument7 pagesValidation of An Arm Crank Ergometer Test For Use in Sedentary AdultsKaribeños San JavierNo ratings yet
- Jones e Doust 1997Document11 pagesJones e Doust 1997Paulo Eduardo RedkvaNo ratings yet
- Chester Step TestDocument6 pagesChester Step TestDandy KurniawanNo ratings yet
- Predicted Maximal Oxygen Consumption (VO2MAX) Values Obtained During The Maximal Treadmill Test Using Different ProtocolsDocument7 pagesPredicted Maximal Oxygen Consumption (VO2MAX) Values Obtained During The Maximal Treadmill Test Using Different ProtocolsYsik RodriGuezNo ratings yet
- Aerobico - 483Document9 pagesAerobico - 483DVD FUTBOLNo ratings yet
- OK A Critical Evaluation of Current MethodsDocument8 pagesOK A Critical Evaluation of Current MethodsElcio Alvares NetoNo ratings yet
- Validity and Reliability of The VO2 Master Pro For Oxygen Consumption andDocument20 pagesValidity and Reliability of The VO2 Master Pro For Oxygen Consumption andnorazmiNo ratings yet
- Ijerph 17 09250 v2Document11 pagesIjerph 17 09250 v2Brayan Estiben Agudelo RodriguezNo ratings yet
- IJSM - 29 - 453-459 - 2008 - Pace e RPEDocument7 pagesIJSM - 29 - 453-459 - 2008 - Pace e RPEWellington VicenteNo ratings yet
- Flouris-2010-Prediction of VO2maxDocument4 pagesFlouris-2010-Prediction of VO2maxBumbum AtaunNo ratings yet
- Ingestion of Oxygenated Water Enhacted Lactate...Document7 pagesIngestion of Oxygenated Water Enhacted Lactate...Jamilatunisa AnwarNo ratings yet
- ISRP InhalAirflMeasDocument20 pagesISRP InhalAirflMeasBibbity123No ratings yet
- Effects of Step Duration in Ramp Protocols on Peak Power & Max VO2Document8 pagesEffects of Step Duration in Ramp Protocols on Peak Power & Max VO2Fernando IsaacNo ratings yet
- Inghametal 2008Document7 pagesInghametal 2008ko piNo ratings yet
- The Effect of Carbohydrate Mouth Rinse On 1 h.17Document5 pagesThe Effect of Carbohydrate Mouth Rinse On 1 h.17adawfNo ratings yet
- VAMEVAL Test Determines Max Oxygen Consumption in Young CamerooniansDocument5 pagesVAMEVAL Test Determines Max Oxygen Consumption in Young Camerooniansclaudiu constantinNo ratings yet
- Test MarchaDocument9 pagesTest Marchaholahola123No ratings yet
- Cross-Validation of The 20-Versus 30-s Wingate Anaerobic TestDocument8 pagesCross-Validation of The 20-Versus 30-s Wingate Anaerobic TestNursahanizaNo ratings yet
- Art:10.1186/1465 9921 7 127Document7 pagesArt:10.1186/1465 9921 7 127dvenumohanNo ratings yet
- Ajpheart 1995 268 6 H2311Document10 pagesAjpheart 1995 268 6 H2311hari vijayNo ratings yet
- Heart Rate As A Measure of Exercise Testing Early After Acquired Brain InjuryDocument5 pagesHeart Rate As A Measure of Exercise Testing Early After Acquired Brain InjuryJaviera Soto AndradeNo ratings yet
- Fotheringham. Walking Test Comparisons.Document19 pagesFotheringham. Walking Test Comparisons.Stijn van den BerkmortelNo ratings yet
- Comparison of The YMCA Cycle SubDocument2 pagesComparison of The YMCA Cycle SubBryan Allen Q. ValleNo ratings yet
- New Equations Estimate College Students' Max Oxygen UptakeDocument6 pagesNew Equations Estimate College Students' Max Oxygen UptakeKıymet KayaNo ratings yet
- Cross-Validation of The 20-Versus 30-s Wingate Anaerobic TestDocument8 pagesCross-Validation of The 20-Versus 30-s Wingate Anaerobic TestHanna RikaswaniNo ratings yet
- The Effect of Plyometric Training Volume On Jumping PerformanceDocument5 pagesThe Effect of Plyometric Training Volume On Jumping Performanceja jaojaozinNo ratings yet
- One Minute STST Vs 6MWT en EPOCDocument10 pagesOne Minute STST Vs 6MWT en EPOCMaxi BoniniNo ratings yet
- Rotstein, Dotan, Bar-Or, Tenenbaum. IJSM 1986 - Training Effects On AnT, MaxVO2, & WAnT in Preadolescent BoysDocument6 pagesRotstein, Dotan, Bar-Or, Tenenbaum. IJSM 1986 - Training Effects On AnT, MaxVO2, & WAnT in Preadolescent BoysTeguh SukmaNo ratings yet
- 01 The Physiology of The World Record Holder - DR Andrew JonesDocument16 pages01 The Physiology of The World Record Holder - DR Andrew JonesbiratãNo ratings yet
- Hydration 2009Document1 pageHydration 2009giannidietNo ratings yet
- Bioenergetics Applied To SwimmingDocument23 pagesBioenergetics Applied To SwimmingLoweNo ratings yet
- Influence of Altitude Training On Performance and HbmassDocument11 pagesInfluence of Altitude Training On Performance and HbmassYousri ElghoulNo ratings yet
- Physiological Responses To The Alterg Anti-Gravity TreadmillDocument6 pagesPhysiological Responses To The Alterg Anti-Gravity TreadmillAnonymous b2k9ABe7eNo ratings yet
- Laforgia 1997Document7 pagesLaforgia 1997volmedo28No ratings yet
- Ironman Pacing Strategy PDFDocument9 pagesIronman Pacing Strategy PDFRonald GeorgeNo ratings yet
- Maximal Aerobic Capacity Testing of Older Adults: A Critical ReviewDocument10 pagesMaximal Aerobic Capacity Testing of Older Adults: A Critical ReviewIlham Amal MNo ratings yet
- Six Minute Walk Test A Simple and Useful Test To Evaluate Functional Capacity in Patients With Heart Failure.Document8 pagesSix Minute Walk Test A Simple and Useful Test To Evaluate Functional Capacity in Patients With Heart Failure.Carolina Millan SalfateNo ratings yet
- Comparison of Treadmill Based and Track Based Rockport 1 Mile Walk Test For Estimating Aerobic Capacity in Healthy Adults Ages 30-50 YearsDocument4 pagesComparison of Treadmill Based and Track Based Rockport 1 Mile Walk Test For Estimating Aerobic Capacity in Healthy Adults Ages 30-50 Yearsmanjula dangeNo ratings yet
- RBCDH: Performance Prediction of Endurance Runners Through Laboratory and Track TestsDocument10 pagesRBCDH: Performance Prediction of Endurance Runners Through Laboratory and Track TestsBrayan Estiben Agudelo RodriguezNo ratings yet
- Rowing PDFDocument8 pagesRowing PDFkullNo ratings yet
- Validity of The Favero Assioma Duo Power PedalDocument14 pagesValidity of The Favero Assioma Duo Power PedalcsrpirataNo ratings yet
- Cdj-200 Owners ManualDocument92 pagesCdj-200 Owners ManualNik100% (2)
- CDJ 200 Pro cdmp3 PlayerDocument20 pagesCDJ 200 Pro cdmp3 PlayercsrpirataNo ratings yet
- Scandinavian Med Sci Sports - 2023 - Nuzzo - Overview of Muscle Fatigue Differences Between Maximal Eccentric andDocument15 pagesScandinavian Med Sci Sports - 2023 - Nuzzo - Overview of Muscle Fatigue Differences Between Maximal Eccentric andcsrpirataNo ratings yet
- Cdj-200 Owners ManualDocument92 pagesCdj-200 Owners ManualNik100% (2)
- 22-1K-1 Test Configuration Velometer 2021-06-07Document160 pages22-1K-1 Test Configuration Velometer 2021-06-07csrpirataNo ratings yet
- Install LCD4linux on your DreamboxDocument1 pageInstall LCD4linux on your DreamboxcsrpirataNo ratings yet
- Entry requirementsDocument1 pageEntry requirementscsrpirataNo ratings yet
- Validity and Reliability of The Leomo Motion-Tracking DeviceDocument14 pagesValidity and Reliability of The Leomo Motion-Tracking DevicecsrpirataNo ratings yet
- Polarized Training Has Greater Impact On Key Endurance Variables Than Threshold, High Intensity, or High Volume TrainingDocument9 pagesPolarized Training Has Greater Impact On Key Endurance Variables Than Threshold, High Intensity, or High Volume TrainingsergiNo ratings yet
- Feedback Reporting FormDocument1 pageFeedback Reporting FormcsrpirataNo ratings yet
- Feedback Reporting FormDocument1 pageFeedback Reporting FormcsrpirataNo ratings yet
- Dynamix 2500 Data Collector: User ManualDocument218 pagesDynamix 2500 Data Collector: User ManualcsrpirataNo ratings yet
- Exploded View and Spare Part Listing for Three Air Conditioner ModelsDocument10 pagesExploded View and Spare Part Listing for Three Air Conditioner ModelscsrpirataNo ratings yet
- Bascula Nutrition Scales PDFDocument101 pagesBascula Nutrition Scales PDFcsrpirataNo ratings yet
- Colector Analizador de Vibraciones Falcon PDF 2 MBDocument6 pagesColector Analizador de Vibraciones Falcon PDF 2 MBGabriel Alexis MartínezNo ratings yet
- Progress Tracker Site VersionDocument9 pagesProgress Tracker Site VersioncsrpirataNo ratings yet
- Building Aerobic FitnessDocument9 pagesBuilding Aerobic FitnesscsrpirataNo ratings yet
- A Season Review VeloDocument10 pagesA Season Review VelocsrpirataNo ratings yet
- RMS o Peak To Peak Acceleration Enveloping AlarmDocument1 pageRMS o Peak To Peak Acceleration Enveloping AlarmcsrpirataNo ratings yet
- 2015-11-18 - Suplementos para Corredores de Fondo y TriatletasDocument4 pages2015-11-18 - Suplementos para Corredores de Fondo y TriatletascsrpirataNo ratings yet
- How To Powercrank Firmware UpdatesDocument1 pageHow To Powercrank Firmware UpdatescsrpirataNo ratings yet
- The Effect of Bicycle Seat-Tube Angle On Muscle Activation of Lower ExtremityDocument5 pagesThe Effect of Bicycle Seat-Tube Angle On Muscle Activation of Lower ExtremitycsrpirataNo ratings yet
- An Introduction To TrainingPeaks MetricsDocument1 pageAn Introduction To TrainingPeaks MetricscsrpirataNo ratings yet
- Retrofit GPS Antenna Installation GuideDocument1 pageRetrofit GPS Antenna Installation GuidecsrpirataNo ratings yet
- H2288 FullDocument12 pagesH2288 FullcsrpirataNo ratings yet
- Vehicle ListDocument44 pagesVehicle ListcsrpirataNo ratings yet
- POPULARITY OF CREDIT CARDS ISSUED BY DIFFERENT BANKSDocument25 pagesPOPULARITY OF CREDIT CARDS ISSUED BY DIFFERENT BANKSNaveed Karim Baksh75% (8)
- mcs2019 All PDFDocument204 pagesmcs2019 All PDFRheydel BartolomeNo ratings yet
- Barelwiyah, Barelvi Chapter 1 (Part 2 of 5)Document31 pagesBarelwiyah, Barelvi Chapter 1 (Part 2 of 5)Dawah ChannelNo ratings yet
- Rotational Equilibrium SimulationDocument3 pagesRotational Equilibrium SimulationCamille ManlongatNo ratings yet
- Grade 8 Lily ExamDocument3 pagesGrade 8 Lily ExamApril DingalNo ratings yet
- Answer Questions Only: Chemical Engineering DeptDocument2 pagesAnswer Questions Only: Chemical Engineering DepthusseinNo ratings yet
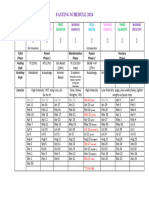
- Moon Fast Schedule 2024Document1 pageMoon Fast Schedule 2024mimiemendoza18No ratings yet
- Oracle® E-Business Suite: Integrated SOA Gateway Implementation Guide Release 12.2Document202 pagesOracle® E-Business Suite: Integrated SOA Gateway Implementation Guide Release 12.2yadavdevenderNo ratings yet
- OPHTHALDocument8 pagesOPHTHALVarun ChandiramaniNo ratings yet
- Solutions: Spheres, Cones and CylindersDocument13 pagesSolutions: Spheres, Cones and CylindersKeri-ann MillarNo ratings yet
- 3.1 C 4.5 Algorithm-19Document10 pages3.1 C 4.5 Algorithm-19nayan jainNo ratings yet
- Vincent Ira B. Perez: Barangay Gulod, Calatagan, BatangasDocument3 pagesVincent Ira B. Perez: Barangay Gulod, Calatagan, BatangasJohn Ramsel Boter IINo ratings yet
- Lateral capacity of pile in clayDocument10 pagesLateral capacity of pile in clayGeetha MaNo ratings yet
- Characteristics and Guidelines of PublicspaceDocument3 pagesCharacteristics and Guidelines of PublicspaceJanani SurenderNo ratings yet
- 10 Tips To Support ChildrenDocument20 pages10 Tips To Support ChildrenRhe jane AbucejoNo ratings yet
- LogDocument119 pagesLogcild MonintjaNo ratings yet
- Strategic Flexibility: The Evolving Paradigm of Strategic ManagementDocument3 pagesStrategic Flexibility: The Evolving Paradigm of Strategic Managementnanthini kanasanNo ratings yet
- Omobonike 1Document13 pagesOmobonike 1ODHIAMBO DENNISNo ratings yet
- Siga-Cc1 12-22-2010Document6 pagesSiga-Cc1 12-22-2010Felipe LozanoNo ratings yet
- Admission Procedure For International StudentsDocument8 pagesAdmission Procedure For International StudentsAndreea Anghel-DissanayakaNo ratings yet
- Ringkasan LaguDocument4 pagesRingkasan LaguJoe PyNo ratings yet
- 2 5 Marking ScheduleDocument6 pages2 5 Marking Scheduleapi-218511741No ratings yet
- PedigreesDocument5 pagesPedigreestpn72hjg88No ratings yet
- Decembermagazine 2009Document20 pagesDecembermagazine 2009maria_diyah4312No ratings yet