Health
Prsfrssians
Caun*il af Zarnbia
I'rrift\:ng furld1ffiff u' ifeoukolf {fd T'firiing Sidndrr,Ts
THE TTEALTH PROFESSIONS COUNCIL OF ZAMBIA
The Health Professions Act,2009
(ActNo.24of 2W9l
The Health Professions
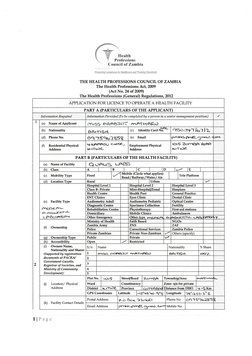
APPLICATION FOR LICENCE TO OPERATE A HEALTH FACILITY
PART A BARTICULARS OF THE
Infornafion:Prouided f o bz, campleted,bg a ?ers an ht a'seniot management p osi*iott)
(a) NameofApplicant flrrrSS FR.atssdT rnATH AR\)
Q5e3i--7 Je=: l:-
oq*75qt)2858 p reta,S" prn€: $rve1r ;"
tttdnFFsu eroe,
14tfuse
PART B (PARTICULARS OFTHE HEALTH FACILITY)
lVlobile (Circle what applies)
(e) FacilityType
nn€F€,eL-
Oi6G+.)C6,t(c-
Private Non-Zambian
(r) OwnersName,
Nationality and Shares
(Supporte il by r egisbation
ilocwnettts aIPACRA/
Gwer*uent Gazeltc,
S.egiskar of Societies, and
Ministry af Cownanity
(,) Location/ Physical
Address
18r'rz'61 .2i16
p.t:.Bo1 2?-tE,O
ft) FacilityContactDetails
llPage
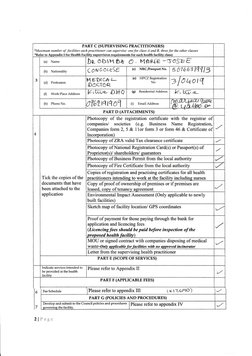
� PART C (SUPERYISING PRACTITIONERS}
*llkaeimum number of
.facilisies each prutctitioner can supervise: ane for class A and B, three for the ather classes
*Refer to Aroendix I for Health Facilitg suoervision reouiremenb fcr each health faeilitg classl
{a) Name D* oblH bk o , Mfr+tE -( rosEe
{b) Nationality Coru GoLeSE {c} NRCI?aespottNo. 5 b76b3 lcll l3
(e)
.,
(d) Profession
F4 FDiC&2-
0oeroR
HPCZ Registration
No 3 l0 lotq
(0 Work Place Address Vt6:<- 0"}la (g) Reeidential Ad&ess 1a-fifi-z-
\-A-,LlIdtU./@
ft) PhoneNo.
cr|znn01 (i) EmailAddress
) t tt\)Mt. a"
PARTD (AT TACHMENTS}
Photocopy of the registratior certificate with the registrar of
companiesl societies (e.g. Business Name Registratiou,
Companies form 2, 5 & 11or form 3 or form 46 & Certificate of
4 Incomoration)
Photocopy of ZRA valid Tax cleatance certificate
Photocopy ofNational Registration Card(s) or Passport(s) of
Proorietor(s)/ shareholders/ crarantors
Photocopy of Business Permit from the local authority
Photocopy of Fire Certificate frorn the local authority
Copies of registration and praetising certifisates for all health
Tick the copies of the practitioners intendinq to work at the facilitv includins ourses
doeuments that have Copy ofproof of ownership ofpremises or if premises are
been attaehed to the leased- coov of tenancv asreement
r/
application Environmental Impact Assessment (Only applicable to newly
built facilities)
Sketch map of facility location/ GPS coordinates
Proof of payment for those paying through the bank for
application and |isgnqing fees
(Lieeneingfees should be paid before inspection of the
pr o o o se d h e alth fa c il itrt\
MOU or signed contract with companies disposing of medical
waste-Ontv aoolieable for facilities a,ith no aooroved incinerator
Letter from the supervising health practitioner
PART E (SCOPE Or SER\rICES)
Indicate services intended to
be provided atthe healih
Please refer to Appendix II
?/
facility
PART F {ATPLICABLE FEES}
6 Fee Schedule Please refer to appendix III ( Kl7,6qo)
PART G (FOLICIES AND PROCEDURES)
the co,ncil policies and procedures Please refer to appendix fV
7 :""J*[ilL?t#lt: I
2fPrrge
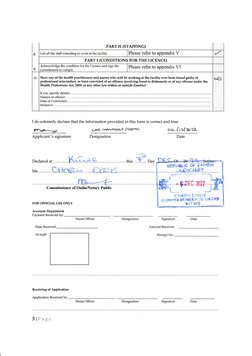
� PARTH (STAFTING}
8 List all the staff intendingto work at the facility Please refer to appendix V
PARTI (CONDITIONS FORTHE LICENCE)
Acknowledge tlre condition for the Licence and sign the Please refer to appendix VI
9 commitment to comDlv
Have any of the health practitioners and nutses who will be working atthe facility ever beenfound guilty of
10
professional misconduct, or been convicted of an offence involving fraud or dishonest5r or of any offence under the
NO
Ifealth Professions Act, 2fi)9, or any other law within or outside Zarrrbia?
If rro< cntrirv dpfril<.
IrJefirrc nf nffcnce'
I do solemnly declare that the information provided in this form is correct and true
PftAV---=r Lne, .\'.FtNriG€s f€e,^n6 oe= /r:-12sfr-.
Applicant's signature Designation Date
Me -C**nB. ?,{. ...... .&r}a-o"S
Commissioner of Oaths/l'{otary PubHc ffiF;;;
CFrAFfi f,ffli!-t
GUMMii gIOi*ET F {JH OAT}IS
FOR OFFICIAL USE ONLY xlTw€
Accounts Deparbnent
Pa;.rnent Received by:
Name Officer Desigr.ation Signature
Date Received Amount Received
STAMP Reeeipt No:
Receiving of Application
Application Received by;
Name Officer Designation Sigrature
3lFage
� APPENDIX I: CLASSIFICATION OF IIEALTH FACILITIES
Class Level Score ofServices Suoervision
Hospices
r A facility to provide palliation ofa chronically ill, terminally ill or seriously ill patieat's pain Medical
and symptoms. and attendiag to their emotional and spiritual aeeds. doctor
1. GeneralOPDservices Full-time
2. Wards: minimum of General Admission ward and Matemity services Medical
Level I 3. Rehabilitations, Pharmaceutical seffices, Theatre, Standard Laboratory, X-ray, Ultrasound, Doctor
Hospital occupational Health & dental clinics
4. In-house/ outsourced support services (Ambulance, kitchen, laundry & mortuary)
5. Mandatorv Eish Desendencv utrit with a caoacitv of 7 bed for everu 700 oatlents
1- OPD seryices with minimum specialities il Ifiemal Medicine, Geaeral Surgery, OBGY and Specialist
Paediatrics. Ophthalmology speciality as desirable. Full-time
2. In-Patients with Minimum of Surgical Medical, Gynae, Obstetrics, neonatal and Paediatrics Medical
ward. Psychiatry services are desirable. Doctcr
Level2 3. Rehabilitations, Pharmaceutical services, Theatre, dental, X-ray, occupational health clinic,
Hospital Ultasound & CT scan/MN
A
4. Laboratory Services with a minimum of Haematologr, Clinical Chemistry, Microbiology &
Blood Baak.
5. In house Support services (Ambulance, Kitchen, Laundry & Mortuary)
6. Stundsd Intensive cnre uniT with a canacitv of I bed {or ewru 100 oatients
1. Out-patient services that include, Filter Clinic, Casualty & speciality Ctinics Specialist
2. In patients wards for standard and specialised services Full-time
3. Rehabilitations, Theatre, dental, occupation health clinic, X-Ray, Ultrasound & CT Medical
Level 3 scan/I\4RI Doctor
Hospital 4. Level 2 Hospital Laboratory Services. Besides, advanced chemistoy profiling, molecular
A11
diagnostics, reproductive diamostics.
5. In house Support services (Ambulance, Kitchen, Laundry & Mortuar"y)
6. Advsnced Intensive care anil with a csaaeirv of I bed for everv 100 ooticnts
1. A11 class A hospital requirements Specialist
Teaching 2. Must be an approved intemship and Specialty Training Programme (STP) site Full-time
Hospital 3. Attached (Linkage) to HPCZ recopised Medical University Medical
4. Recommendation lefier &om the Ministrv resoonsible fcr Health Doctor
a A facility to provide diap.ostic service, prevention aad treatment of disease and illness on Part-time
an out-patient basis and to incorporate the services ofmultiple registered health practitioners Medical
and the use of equipmeat for diagnosis aad treatuen! including medical laboratories and Doctor
B Nil
with the capacity to ofler some level 1 -hospital services on an out-patient basis. This includes
Urtran Health Centres, Zonal Health Centres and multiple specialist clinics. Zonal and Urban
health Cenhes to have proyision for observation ofoatients.
First Aid stations and Sick bays to provide diagnostic services, prevention aod treatment of Part-time
diseases and to perform physical examinations using simple equipment and takiag specimens Clinical
for' laboratory analysis to a specified taxget group, e.g. School first Aid Stations, Optical Officer or
Level 1
equivalent
centres and Industrial Plant etc. These do not require standard pharmacy services but will
have a medicine cupboard and ernergency tray managed by licenced rurses or clinician in
the treatment room for the stabilisatioa ofpatieots.
C I Stand-alone specialised clinics that provide prevention and &eament of diseases without Specialist in
performing invasive pmcedures. The example includes eye clinics and dental clinics. the same field
Level 2
Pharmaceudcal services are optional. Specialised clinics like dental must have a medicine
cuoboard for soecific medicine manaeed bv a licenced health rractitioner.
Fult-time
a For a health facility to provide diagrrostic services, prevention atrd treafrieot ofdiseases and
fliaical
Level 3 to perform physical examinations using simple equipment and to take specimens for
OfEcer or
labomtory analysis. Exanrple Health Pos! Rural Health Centres etc.
mrriwalmt
Level 1 . Soecimer collection centres that shall be suoervised bv a Laboratorv Technolosist Technologist
D"/ Ixvel2y' r Medical diagaostic laboratory or radiological seryice outside a hospital. Degree in
Lwel 3 e The iadustrial laboratory ttrat tests and certifies foo4 water and beverage content same field
Minimum
E Level 2 . Therape$tic stand-aloue physiotherapy and rehabilitation services diplomaia
sanre field
Note: Mobile health services shall be classified usiag the same criteria. Stand-alone ambulance and Rescue vehicle services shall be
licerced as Class C - Level 2 with a defined fleet of vehicles. Ambulanees for the licenced fixed healtt facilities shall be classified as Class
C level 2
5lPage
� APPENDIX II: SCOPE OF SERVICES
Bed Capacity Catchment Population
ServiceArea Seriiee Scope
Aopointment Based
Operating Hours Dav time (Mav excluded Sunday & Weekends)
24 hours services
Patient Triaeine services
General Practice Consultation and Treatment
General Surserv Soecialtv Consultation and Treatment
General Sureery Specialty Consultation and Treatment
Internal Medicine Soecialtv Consultation and Treatrnent
Pediatric & Child Health Surserv Soecialtv Consultation and Treatmenl
Ohstetrics & Gvnecolory Snecia.ltu Consrrltation and Treatment
Neurolosv Soecialtv Consultation and Treatment
Orthooedic Soecialtv Consultation and Treatment
Cardiolosv Special8 Consultation and Treatmeot
Urolosv Soecialw Consultation and Treatrnent
Other Snecialty Consuitation aad Treaknent - Specill
Outpatient Services ART Service
VMMC Services
Cervical Cancer Screening
Other Cancer Screening servrces
Endoscooe Service
Electrocardiosram (ECG)
Patient Observation services
Pharmacv Services Pharmaceutical Services
Serolosical
Hematolosv & Immunolow
\Clinical chemistrv
Laboratory Services Microbioloev
molecular biolow
Histopatholocv
Forensic I-ahoratorv
Pubtc Health. Food & Drue Lab Services
Ultrasound
Echocardiogram
X-Rav lmagine
Fluoroscopy
Medical knaging and
Mammosram
Radiological sewices
Comouter Tomosraphv (CT)
Magnetic Resonance Imasins (MR[)
Dexa Scan
Cardiac Catheterisation- Cat-Lab
General Audiometrv
Audiometry and ENT Pediatrics Audiometrv
Ear. Nose and Throat
Nutrition and dietetics consultation and treatment
UI EIAIV
Kitchen and Cafeteria
Oral Health consultatioa
Periodontics reatment procedures
Oral surgery treatment proceduos
Restorative dentistry
Dental survives Endodontics teatment Drocedures
Prosthodontics treatment Drocedures
Orthodontics treafinoflt orocedures
Dental Lab services
Dental X-rav services
Phvsical rehabilitation General Phvsiotherapv
6lP*g*:
� APPENDIX V: LIST OF STAFF INTEIYDING TO WORK AT TIIE FACILITY
,tr*:=.
f, -*gg"
E q;?
t H
"
Health
\' Professionr
flounril of Zarnbi*
k#r6d€ re*?'$grLr fi Fi*air.hrws ar;d -frnriig StcrCardr
FacilityName: QufrurS Laee rrPCh,#: Districfi xlI{F BedCapacity:-
Section/ Registrat Phone NRC/ Employee
S/N Name Profession ion\pe Nationality
Unit Numtrer Parsport Status
dqbaqrl It-rt53p €c}es"+$
,S',.1e€*Jr$t "4 cn€rreAi- €ttt =l-)fie+rl\Sc{
(e-
1
E iL.- EQ.6i\rfv\Bq O'6"{\e{€ ecrf.sE-. e6
€tr€CTALIST tuLL
2. t-AB F(a6€3:5r f\/\er\lffA+J Are,mesrcftL- Ft-ttt-- (F.B*ffi qso3.rl16{ ep.iflsH
frF.t€.
SrleNJrtqT
ReG{t.(Cg.et! f-iji+-
3. i|-!UgS(: e(eLYt{ Ktut{GA eJlfrc. Fuut- 3q6qz%]z 57o\F3f/€{ Z,et.\Bi6rJ '1.1lYrg
BAhFEA F.IGTJ€ft5#e c.\_eaf$e.f{- ]q-783tirE ++srBk l:zar.^r'uA.: fi:L.u
4. C-L€F'(.{#. FuLr- {\me
.FLJ\-J- R.f.r
5. G{.}AAA Fecrr-s toc€f.ror1.)e. G{AE.D OY.,tqrruSll S5:!+'1til61 ZJa*ErB.-l -rrtY1e
6.
7.
8.
9.
t0.
11.
t2.
13.
t4.
15.
l0lFage
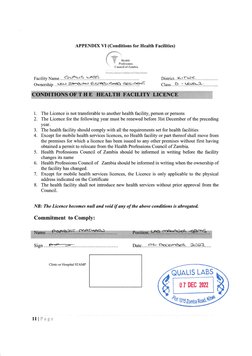
� APPENDIX \{I (Conditions for Health Facilities)
f
E xr*{@
" "'?
i
i F ileatrh
i*if.l$iiii.n*
: ', ,, -, :.J
Facility Name. .. .Q S.:t *.,} l$F.
Ownership .. LioJ. -iz.B.leiF sr .e-S-r-eB!\S S .eg=:.?3ff
1. The Licence is not transferable to another health facility, person or persons
2. The Licence for the following year must be renewed before 31st December of the preceding
year.
3. The health faciiity should comply with all the requirements set for health facilities
4. Except for mobile health services licences, no Health facility or part thereof shall move from
the premises for which a licence has been issued to any other premises without frst having
obtained a permit to relocate from the Health Professions Council of Zambia.
5. Health Professions Council of Zambia should be informed in writing before the facilify
changes its name
6. Health Professions Council af Zambia should be informed in writing when the ownership of
the facility has changed.
7. Except for mobile health services licences, the Licence is only applicable to the physical
address indicated on the Certificate
8. The health faciiity shall not introduce new health services without prior approval from the
Council.
NB: The Licenee becomes null and void if any of the above conditions is abrogated.
Commitment to Comply:
Sim Date aa
Clinic or Hospital STAMP
Qunlts LABs
0I DEC 2022
ffi H
UttotszonnaRoad$$
11 lFage
�INSPECTION OF THE FACILITY
Tick aoorooriatelv
Public Clinic llrban Health Centre Rural Health Cenke Health Post
Hospitai Level 3 Levei 2 Level 1
Zambian Ciinic
Private Hospital
Non-Zambia t lrnrc
Hosoital
Insoectors Comments
Please attach inspection report
Inspector's Name: Date- Signature:
RECOMMENDATION
I have reviewed and verified the following
i. The completeness of the application for licencing Class Facility,
ii. Inspection report
iii. Payments -
iv. Attachments
Comments
and I hereby recorunend that the:
a) The facility be licenced pursuant to Section 38
b) The application be rejected pursuant to Section 39 {a,b, c or d)
Senior Inspections Officer Signature: Date:
APPROVAL
I hereby approve that:
a) The facility be licenced pursuant to Section 38
b) The application be rejected pursuant to Section 39 (a,b, c or d)
(If the application is being rejected, issue notice of rejection pursuant to Regulation 19 (3)
Regional Manager (Name, Signature & Date)
4lFage
�servlces Paediatric Phvsiotheraov
Hvdrotheraov
Soeeeh and lansuase
C)ccuoati on theraov sl.rn
Prosthetics and orthotics
Mentai Health Sewices - Consultation and treatment
Mental Health Services Mental health wards
Rehabilitation serv'ices
Oohthaimic seryices consultation & fteatment
Ophthalmic services Ophrhalmic theatre
Oohthalmic services consultation
Oncology consultation
Cancer Diseases Chemotherapy
Radiotherapv
Occunation health screenins - Yisual
Occupation health screening - Audiometry
vuuuPd
Occuoation health screenins - Heat Tolerance
Occupation heaith screenins - Others
Renal consultation
Renal & Dialysis services
Dialvsis treatment services (Soecifii Units
Intensive Care Unit - ICU (Soecifv Caoacitv
Critical care services Neonatal Intensive Care Unit - MCU (Soecifv Caoacitv-
Hvoerbaric Oxvsen Theraov ffiBOfl Services
Ooeratins theatre services Oneratins theatre services
Pdvate admission rooms
Medical wards
ln-Patient Seryices Sursical wards
Paediatrics
Soecialised wards. Soeci&
Adolescent suooofi service
Matemal services limited to Antenatal. Postnatal & Familv Plannins
MCH & Adolescent
Child health services includins under-5 clinic erowth monitorins
Vaccination
Maternitv Services Matemitv Services
Ambulance-Basic Life Suooort
Ambulance- lntermediate Life Support
Ambulance- Advance Life Suooort
Mobile Services First Responder Vehicle
Rescue Vehicle
Domiciliarv Care
Moblle Clinics
Mortuarv Services
Laundry Services
Support Services
Incineration services
Medical Records and Informatics
Verified by:
Name Officer fFacility Stafg Designation Signature Date
Clinic or Hospital STAMP
TlFag*
� APPENDIX III (FEE SCHEDULE)
A ication Fees - All facilities
ties & serrrices
services
Clinic Zambian Non-Zambian
Class A to E & Mobile health facilities K 450.00 K 450.00
Lice -hees - Private Health facilities
Zambian Non-Zambian
Class A K 3L.900.00 KM,550.40
Class B K28,710.00 K 40,190.00
Class C K 11.650.00 K77,240.00
Class D 'K 11-560.00 K17.240.00 *
Class E K 11_660.00 K"17.240.$A
Mobile health facilities (Air, Water & K 9,260.00 K12,970.80
Road)
Fees - Public Health Facil ties
Zantbian Non-Zambian
Class A & B K 1,130.00 nla
ClassC,D&E K 500.00 nla
Mobile health facilities (Air, Water & K 200.00 n/a
Road)
Accreditation Fees or Provisional) - Private Health Facilities
Zarnbian Non-Zambian
ClassA&B K 4,200.00 K 5.000.00
ClassC,D&E K 1,130.00 K 1,360.00
Accreditation Fees or frovisional) - l'ublic Health facilities
Zanrbian Non-Zambian
Class A & B K1.130.00 nla
Class9D&E K 500.00 nla
Ethical and Clinical Guidelines
National Health Care Standards K 100.00 Professional Code of ethics- GNC
Patients Rieht Charter - Enslish K 50.00 Standard Treatment Guidelines
Patients Rieht Charter - Local Lansuage K 50.00 Zarnbia National F ormularv
Professional Code of ethics- HPCZ K 50.00 British National Formularv - Adults
Confidentialitv suidelines K 50.00 British National Formularv - Paediatrics
Patient consentins guideiines K 50.00 Standard Operating Procedures -
Pafient Record Guidelines K 50.00 specific for the scope of services
Pervasive incentives euidelines K 50.00
SlIlagr:
� APPENDIX Iv (P0LICIES AI{D SOPs)
Standard Details
Governance & Organisation structure
Leadership Action plan and strategic plan
Scope of sewices
Template of contracts for staff
Template for Appraisal of staff
Clinical supervision system
Disciplinary procedures
Safety measures Infection Control procedures
r Sanitation
r Protective equipment
r Waste management
. General sunoundings management
r Post Exposure Prophylaxis
Patients records Patients record management
. Filling system
r Patientinformationmanagement
r Conlidentiality
r Securitv of oatient records
Service-specific Laboratory procedures & policies
procedures Pharmaceutical management procedures and qrddelines
Blood transfusion services procedures & policies
Surgical flheatre) and Dental services procedures & policies
Errergency care (ICU) procedures & policies
Optical and ophthalmic care services
Rehabilitation (Physiotherapy) procedures & policies
Radiology services procedures & policies
Medical social work procedures & policies
Clinical marragement procedures and guidelines
9lPage