You might also like
- Crystal+Essentials a+Beginners+Guide+to+Crystals FINALDocument7 pagesCrystal+Essentials a+Beginners+Guide+to+Crystals FINALGretchenNo ratings yet
- Hema Lec CompiledDocument68 pagesHema Lec Compiledchris andrieNo ratings yet
- Hematological Investigation or Quantitative Evaluation of The Hematopoietic SystemDocument21 pagesHematological Investigation or Quantitative Evaluation of The Hematopoietic SystemMAMA LALANo ratings yet
- (PATHO) LEC 013 RBC-and-Bleeding-DisordersDocument20 pages(PATHO) LEC 013 RBC-and-Bleeding-DisordersEzhilNo ratings yet
- Chapter 1: An Overview of Clinical LaboratoryDocument13 pagesChapter 1: An Overview of Clinical LaboratoryAshley Tañamor100% (2)
- Ninja® Foodi™ Smart XL 6-In-1 Indoor Grill Quick Start GuideDocument2 pagesNinja® Foodi™ Smart XL 6-In-1 Indoor Grill Quick Start GuidehawkjohnNo ratings yet
- (Trans) Chapter 16: Anemias - Red Blood Cell Morphology and Approach To DiagnosisDocument4 pages(Trans) Chapter 16: Anemias - Red Blood Cell Morphology and Approach To Diagnosisgotvelvet world dominationNo ratings yet
- Dr. Sailendra Nayak Assistant Professor MedicineDocument49 pagesDr. Sailendra Nayak Assistant Professor MedicineAishwarya JeeNo ratings yet
- Hematopathology All LecturesDocument226 pagesHematopathology All LecturesYousif AlaaNo ratings yet
- RBC DisordersDocument8 pagesRBC DisordersDavid JohnNo ratings yet
- Hematology Notes for Medical StudentsFrom EverandHematology Notes for Medical StudentsRating: 5 out of 5 stars5/5 (1)
- Heamatology Dr. Osama PDFDocument94 pagesHeamatology Dr. Osama PDFAnmar ZawahraNo ratings yet
- Basic Hematologic TestsDocument9 pagesBasic Hematologic TestsdtimtimanNo ratings yet
- Personal Grooming PDFDocument8 pagesPersonal Grooming PDFayuNo ratings yet
- Sure Track SystemDocument2 pagesSure Track SystemIcal AgamNo ratings yet
- What Is Anemia, How Do You Diagnose Anemia, and How Are The Different Anemias Classified?Document60 pagesWhat Is Anemia, How Do You Diagnose Anemia, and How Are The Different Anemias Classified?Priyanka MhNo ratings yet
- Tuning Solution V16.0.3.0Document16 pagesTuning Solution V16.0.3.0Amine HerbacheNo ratings yet
- Chapter 13 Rodaks HematologyDocument10 pagesChapter 13 Rodaks HematologyRALPH JAN T. RIONo ratings yet
- Midterms 88%Document18 pagesMidterms 88%jrence80% (5)
- Solutions and Solubility Practice Hon-18Document3 pagesSolutions and Solubility Practice Hon-18api-368121935No ratings yet
- Anemia 1Document104 pagesAnemia 1maryam ijazNo ratings yet
- Dresses For Every Occasion: Pattern SheetDocument19 pagesDresses For Every Occasion: Pattern SheetManuela IacobNo ratings yet
- Name: Gotoh, Aaron Tzergio C. DATE: 05/12/20 Erythrocyte Indices WorksheetDocument3 pagesName: Gotoh, Aaron Tzergio C. DATE: 05/12/20 Erythrocyte Indices WorksheetMarie LlanesNo ratings yet
- 8.1 RBC MorphologyDocument5 pages8.1 RBC MorphologyChelsea PialagoNo ratings yet
- MLS305 Hema Lec PrelimsDocument16 pagesMLS305 Hema Lec PrelimsEvanka BaguistanNo ratings yet
- RBC 2014 EngDocument38 pagesRBC 2014 Engsnowrose2609No ratings yet
- Module 4 RBC Morphology 2Document6 pagesModule 4 RBC Morphology 2Pauline Louise S. DURANNo ratings yet
- HematocritDocument3 pagesHematocritMaybelle Acap PatnubayNo ratings yet
- Red CellDocument4 pagesRed CellUmer naeemNo ratings yet
- RBC PathologyDocument7 pagesRBC PathologyKent CruzNo ratings yet
- Haematology 2 ManualDocument26 pagesHaematology 2 Manualhayamitib11No ratings yet
- Hem OncDocument26 pagesHem OncJim XieNo ratings yet
- Introduction of Natural ImmunityDocument4 pagesIntroduction of Natural ImmunitySamanthaNo ratings yet
- Hemoglobin Determination: Cyanmethemoglobin MethodDocument32 pagesHemoglobin Determination: Cyanmethemoglobin MethodNasser DabiNo ratings yet
- Case 1: 25 Yr Old Patient With History of FatigueDocument79 pagesCase 1: 25 Yr Old Patient With History of FatigueMira Wrycza100% (1)
- Harr ReviewerDocument5 pagesHarr ReviewerBernard Garcia OledanNo ratings yet
- Blood IndicesDocument4 pagesBlood IndicesCharmaine RosalesNo ratings yet
- Hema FIN NotesDocument8 pagesHema FIN NotessansastarkNo ratings yet
- CP RBC DisorderDocument15 pagesCP RBC DisorderDETECTIVE CONANNo ratings yet
- Strategi Diagnosis AnemiaDocument49 pagesStrategi Diagnosis Anemianiniek yusidaNo ratings yet
- Anemia: Hematologic System Choi DabiDocument15 pagesAnemia: Hematologic System Choi DabiAftab KhalilNo ratings yet
- Anemia: Hematologic System Choi DabiDocument15 pagesAnemia: Hematologic System Choi DabiAftab KhalilNo ratings yet
- 02 - Examination of Blood and Bone Marrow HematologyDocument3 pages02 - Examination of Blood and Bone Marrow Hematologyhamadadodo7No ratings yet
- RBC AnomaliesDocument5 pagesRBC AnomaliesThe16LoverrNo ratings yet
- UntitledDocument112 pagesUntitledMerriyet MbNo ratings yet
- Lab Activity No. 5 - Slide PresentationDocument24 pagesLab Activity No. 5 - Slide PresentationChelsea Padilla Delos ReyesNo ratings yet
- Red Blood Cell MorphologyDocument5 pagesRed Blood Cell MorphologyRyan KadavilNo ratings yet
- 7 - MT Hematology Module 7 LectureDocument3 pages7 - MT Hematology Module 7 LectureAnthonyNo ratings yet
- HEMATOLOGYDocument153 pagesHEMATOLOGYmariel clementeNo ratings yet
- Hematology Tests - G I SVDocument49 pagesHematology Tests - G I SVSV. Trần Hữu ThắngNo ratings yet
- Hematology & UrinalysisDocument77 pagesHematology & UrinalysismekuriawNo ratings yet
- Red and White Blood Cell DisordersDocument11 pagesRed and White Blood Cell DisordersVittorio Di PaoloNo ratings yet
- Complete Blood Count by DakhanDocument18 pagesComplete Blood Count by Dakhankhan khanNo ratings yet
- Basic Examinations of The Blood: 0.5G SHB/DL of Blood O Hemoglobin Concentration DeterminationDocument14 pagesBasic Examinations of The Blood: 0.5G SHB/DL of Blood O Hemoglobin Concentration DeterminationZllison Mae Teodoro MangabatNo ratings yet
- Anemia OsamaDocument57 pagesAnemia Osamaosamafoud7710No ratings yet
- HematologyDocument26 pagesHematologyScolaNo ratings yet
- Hemoglobin Determination: Cyanmethemoglobin MethodDocument31 pagesHemoglobin Determination: Cyanmethemoglobin Methodبراءة أحمد السلاماتNo ratings yet
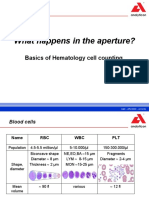
- What Happens in The Aperture?: Basics of Hematology Cell CountingDocument16 pagesWhat Happens in The Aperture?: Basics of Hematology Cell CountingYaser AlaniNo ratings yet
- Clinpath - : Red Blood CellsDocument14 pagesClinpath - : Red Blood CellsYolanda Primrosa NurhanNo ratings yet
- Anemia, Tic, DLC MbbsDocument50 pagesAnemia, Tic, DLC Mbbssharads221004No ratings yet
- Integrated Therapeutics Iii Credit 4Hrs/Week: Instructor: Tamrat Legesse (B.Pharm, MSC in Clinical Pharmacy)Document145 pagesIntegrated Therapeutics Iii Credit 4Hrs/Week: Instructor: Tamrat Legesse (B.Pharm, MSC in Clinical Pharmacy)dawitNo ratings yet
- Anemia OsamaDocument57 pagesAnemia Osamaosamafoud7710No ratings yet
- Back To The BasicsDocument5 pagesBack To The BasicsNinjafrankiiiNo ratings yet
- Hematocrit and Red Cell IndicesDocument10 pagesHematocrit and Red Cell Indicespodcast gazalNo ratings yet
- HEMATOLOGYDocument5 pagesHEMATOLOGYMA. ANDREA NICOLE BITOINNo ratings yet
- HEMATOLOGYDocument17 pagesHEMATOLOGYMA. ANDREA NICOLE BITOINNo ratings yet
- HEMATOLOGYDocument5 pagesHEMATOLOGYMA. ANDREA NICOLE BITOINNo ratings yet
- HEMATOLOGYDocument36 pagesHEMATOLOGYMA. ANDREA NICOLE BITOINNo ratings yet
- Media FillDocument13 pagesMedia FillraghuNo ratings yet
- F2-14 Budget PreparationDocument18 pagesF2-14 Budget PreparationJaved Imran100% (1)
- Module 5 Advanced MechanicsDocument60 pagesModule 5 Advanced Mechanicsiknowvictoriassecret49No ratings yet
- English: Quarter 1 - Module 1Document34 pagesEnglish: Quarter 1 - Module 1Roel MabbayadNo ratings yet
- Acc CH2Document4 pagesAcc CH2Trickster TwelveNo ratings yet
- Stroke - Wikipedia, The Free EncyclopediaDocument31 pagesStroke - Wikipedia, The Free EncyclopediaRhonskiiNo ratings yet
- GSE580Document132 pagesGSE580Anonymous g4wR41qNeNo ratings yet
- Health Related Fitness and NutritionDocument4 pagesHealth Related Fitness and NutritionKarol RydloNo ratings yet
- CS687 - Access Control 1 - Spring 2020Document41 pagesCS687 - Access Control 1 - Spring 2020Dawit GetchoNo ratings yet
- Uponor v. Sioux Chief Mfg.Document5 pagesUponor v. Sioux Chief Mfg.PriorSmartNo ratings yet
- Seuring+and+Muller 2008Document12 pagesSeuring+and+Muller 2008Stephanie Cutts CheneyNo ratings yet
- Development LetterDocument3 pagesDevelopment Lettertan balanNo ratings yet
- Newsflash MagazineDocument64 pagesNewsflash MagazineIan LuoNo ratings yet
- Master Thesis In-Depth InterviewsDocument5 pagesMaster Thesis In-Depth Interviewsrqopqlvcf100% (1)
- Gregg Djs Dict OcrDocument424 pagesGregg Djs Dict OcrscribdNo ratings yet
- J4500 Basic Electrical Schematics (Epa2017, Gen V) W/Parker VMM, Effective With Unit 68229Document91 pagesJ4500 Basic Electrical Schematics (Epa2017, Gen V) W/Parker VMM, Effective With Unit 68229HamiltonNo ratings yet
- Chapter OneDocument36 pagesChapter OneJeremiah Alhassan100% (1)
- STOD-GEN-AED-0000-ME-SPE-0012 - Functional Specification For AGP Booster PumpsDocument14 pagesSTOD-GEN-AED-0000-ME-SPE-0012 - Functional Specification For AGP Booster PumpsAHMED AMIRANo ratings yet
- Cambridge International Examinations Cambridge International Advanced LevelDocument8 pagesCambridge International Examinations Cambridge International Advanced LevelIlesh DinyaNo ratings yet
- Ebook PDF Consumer Behaviour Asia Pacific Edition by Wayne D Hoyer PDFDocument41 pagesEbook PDF Consumer Behaviour Asia Pacific Edition by Wayne D Hoyer PDFmarvin.tappen826100% (35)
- Sekar KSP - Hypoglicemia Ec Tipe 2 DMDocument28 pagesSekar KSP - Hypoglicemia Ec Tipe 2 DMdianarahimmNo ratings yet
- BMI Middle East and Africa Oil and Gas Insight March 2016Document10 pagesBMI Middle East and Africa Oil and Gas Insight March 2016Anonymous pPpTQrpvbrNo ratings yet