Professional Documents
Culture Documents
S41565-021-00870-Y Computationally Guided High-Throughput Design of Self-Assembling Drug Nanoparticles
Uploaded by
He ZeeOriginal Title
Copyright
Available Formats
Share this document
Did you find this document useful?
Is this content inappropriate?
Report this DocumentCopyright:
Available Formats
S41565-021-00870-Y Computationally Guided High-Throughput Design of Self-Assembling Drug Nanoparticles
Uploaded by
He ZeeCopyright:
Available Formats
Articles
https://doi.org/10.1038/s41565-021-00870-y
Computationally guided high-throughput design
of self-assembling drug nanoparticles
Daniel Reker 1,2,9, Yulia Rybakova1, Ameya R. Kirtane 1,2, Ruonan Cao1,3, Jee Won Yang 1,2,4,
Natsuda Navamajiti1,5, Apolonia Gardner1,6, Rosanna M. Zhang1,6, Tina Esfandiary 1,
Johanna L’Heureux1, Thomas von Erlach1, Elena M. Smekalova1, Dominique Leboeuf7, Kaitlyn Hess 1,
Aaron Lopes1, Jaimie Rogner1, Joy Collins1, Siddartha M. Tamang1, Keiko Ishida1, Paul Chamberlain1,
DongSoo Yun 1, Abigail Lytton-Jean 1, Christian K. Soule1, Jaime H. Cheah1, Alison M. Hayward1,2,
Robert Langer 1,8 and Giovanni Traverso 2,8 ✉
Nanoformulations of therapeutic drugs are transforming our ability to effectively deliver and treat a myriad of conditions.
Often, however, they are complex to produce and exhibit low drug loading, except for nanoparticles formed via co-assembly
of drugs and small molecular dyes, which display drug-loading capacities of up to 95%. There is currently no understanding
of which of the millions of small-molecule combinations can result in the formation of these nanoparticles. Here we report the
integration of machine learning with high-throughput experimentation to enable the rapid and large-scale identification of such
nanoformulations. We identified 100 self-assembling drug nanoparticles from 2.1 million pairings, each including one of 788
candidate drugs and one of 2,686 approved excipients. We further characterized two nanoparticles, sorafenib–glycyrrhizin and
terbinafine–taurocholic acid both ex vivo and in vivo. We anticipate that our platform can accelerate the development of safer
and more efficacious nanoformulations with high drug-loading capacities for a wide range of therapeutics.
S
mall molecular therapeutics are often poorly soluble in water1. therapy, and antiviral, antimalarial and antifungal drug delivery.
This can cause formation of micrometre-sized colloidal aggre- We performed ex vivo and in vivo proof-of-concept studies on two
gates2,3, decreasing bioavailability and therapeutic efficacy3,4. novel co-aggregated nanoparticles. Both validations highlight the
Solid drug nanoparticles stabilized by lipids and/or polymers can ability of our platform to facilitate the generation of nanoparticles
alleviate these problems5,6, but their low drug loading is an impor- with high drug loading and improved bioavailability.
tant limitation7–9. Recently, it has been shown that co-formulating
certain cancer drugs with specific small molecular dyes such as High-throughput platform for co-aggregate identification
Congo red10 or IR78311 can form stable nanoparticles with ultrahigh We selected drugs that self-aggregate into colloidal macrostructures
drug loading. We propose that formulating drug nanoparticles by as candidates for our platform, since self-aggregating molecules
excipient-aided co-assembly is not limited to chemotherapeutics are more prone to co-aggregation10,11. A random forest model can
and chemical dyes but transferable to a wider range of drugs and identify self-aggregators with precision of 77 ± 2% in retrospec-
excipients. It is currently not understood which of the millions of tive cross-validation experiments (Supplementary Table 1)3,13. This
possible drug–excipient combinations lead to nanoparticle forma- model identified 788 approved drugs as likely to self-aggregate and
tion with the desired properties. therefore as candidate material for our nanoparticle formulation
In this Article, we integrated molecular dynamics (MD) simula- platform (Supplementary Note 1). We selected 20 compounds for
tions and machine learning with a high-throughput experimental screening to span a variety of indications while ensuring chemical
co-aggregation platform to identify drug–excipient combinations diversity (Supplementary Fig. 1). We used dynamic light scattering
that form stable, self-assembled solid drug nanoparticles on the (DLS) to confirm the self-aggregation propensity of these candi-
basis of solvent exchange without the need for chemical synthesis dates and found that four of the selected drugs did not show detect-
(Fig. 1a). We identified a total of 100 novel co-aggregated solid drug able self-aggregates and were discarded (Supplementary Table 2).
nanoparticles from 2.1 million possible pairings of 788 candidate The other 16 drugs formed micrometre-sized self-aggregates and
drugs with one of 2,686 excipients. We used US Food and Drug represented a diverse set of candidate drugs for co-aggregation.
Administration (FDA)-approved drugs and excipients to accelerate A set of 90 excipients were selected from the FDA list of inactive
the translation of these nanoformulations9,12, with potential applica- ingredients12, the FDA list of ‘generally recognized as safe’ ingredi-
tions including cancer therapy, immunosuppressive therapy, asthma ents14, and other FDA-approved small molecules15. Selection criteria
1
Koch Institute for Integrative Cancer Research, Massachusetts Institute of Technology, Cambridge, MA, USA. 2Division of Gastroenterology, Hepatology
and Endoscopy, Department of Medicine, Brigham and Women’s Hospital, Harvard Medical School, Boston, MA, USA. 3Division of Engineering Science,
University of Toronto, Toronto, Ontario, Canada. 4Robert Frederick Smith School of Chemical and Biomolecular Engineering, Cornell University, Ithaca,
NY, USA. 5Biomedical Engineering Program, Faculty of Engineering, Chulalongkorn University, Bangkok, Thailand. 6Department of Electrical Engineering
and Computer Science, Massachusetts Institute of Technology, Cambridge, MA, USA. 7Skolkovo Institute of Science and Technology, Moscow, Russia.
8
Department of Mechanical Engineering, Massachusetts Institute of Technology, Cambridge, MA, USA. 9Present address: Department of Biomedical
Engineering, Duke University, Durham, NC, USA. ✉e-mail: cgt20@mit.edu
Nature Nanotechnology | VOL 16 | June 2021 | 725–733 | www.nature.com/naturenanotechnology 725
Articles NaTure NanOTecHnOlOgy
included chemical diversity (Supplementary Fig. 1) and commer- gies and kinetic energies. Together, these computations gener-
cial availability. With the exception of Congo red, which served ated a 4,515-dimensional descriptor per drug–excipient pair. A
as a positive control10, none of these materials had been used in total of 1,440 data points collected from the high-throughput
co-aggregating nanoparticles. However, our material selection did co-aggregation experimentation, as described above, were used as
specifically select excipients with precedence for biomedical appli- the training set (Fig. 1c).
cations to facilitate in vivo and human testing and provide a path- We employed a random forest machine learning model given
way towards human translation. its robust performance in molecular machine learning and its
We followed established protocols for nanoprecipitation inherent ability to select relevant features. Our model exhibited
to generate nanoparticles from our pairs of drugs and excipi- promising performance in retrospective evaluations based on ten-
ents (Supplementary Note 2)6,7,10. To automate this process and fold cross- and ‘leave one drug out’18 validations (Supplementary
improve reproducibility, we coupled a liquid-handling deck to a Table 3), indicating that our model accurately captures the
high-throughput DLS. This enabled us to rapidly screen 384-well co-aggregation relationships and is able to prioritize suitable
plates of nanoformulations using as little as 1 nmol of drug or excipients for a novel drug. A model that included all parameter
excipient for each experimental replicate. In total, we generated and types was most accurate in predicting co-aggregation outcomes
experimentally tested 1,440 formulations for their ability to form (Supplementary Table 3), although feature importance analysis
co-aggregating nanoparticles. (Supplementary Fig. 3) indicated that simulation-derived quanti-
To determine whether excipients would prevent colloidal fications of molecular interactions and the excipient’s refractivity19
self-aggregation of the drug they were paired with, we compared are most informative to predict co-aggregation (Supplementary
the size of the drug–excipient co-aggregates with the size of the col- Table 4 and Supplementary Note 3). Parameter ablation experi-
loidal self-aggregates formed by the drug alone. We considered a ments confirmed the relevance of the most important features for
size reduction to be meaningful only if the co-aggregates were less our machine learning model (Supplementary Fig. 4). The random
than half as large as the self-aggregates formed by the drug alone forest model outperformed other established machine learning
(Supplementary Fig. 2). Out of 1,440 measured combinations, 94 approaches for our data (Supplementary Table 5), and adversarial
(6.5%) showed the targeted size reduction (Fig. 1b). While some controls indicated that our model identified meaningful patterns
excipients appeared to facilitate co-aggregation more than oth- (Supplementary Table 6)20. Finally, out-of-bag performance of
ers, overall the data suggest a complex molecular-recognition models trained on random subsets of the training data revealed that
mechanism with distinct behaviours emerging across the different the model performance was converging (Fig. 1d), indicating that
pairings. additional screening rounds would most likely not lead to strong
improvements in model quality and advocating for more directed
Machine learning for nanoparticle design acquisition of additional data through predictive modelling.
We hypothesized that a machine learning model trained on these To this end, we modelled the complete co-aggregation landscape
co-aggregation patterns would enable us to extrapolate from this of all 788 aggregating drugs combined with any of the 2,686 avail-
data and rapidly identify additional drug–excipient pairs without able excipients using our machine learning model. In total, 2.1 mil-
the need for laborious high-throughput screening. We described lion formulations were computationally assessed for their ability to
every drug–excipient pair using the chemical substructures and form self-assembling co-aggregated nanoparticles. Given the infea-
physicochemical properties of both the drug and excipient follow- sibility of running MD simulations for all 2.1 million combinations,
ing standard protocols in molecular machine learning16,17. In addi- we applied a machine learning model trained exclusively on chemi-
tion, we performed short MD simulations to quantify non-covalent cal and physicochemical properties. This modified model exhibited
interaction potentials among drugs and excipients on the basis of slightly lower retrospective performance (Supplementary Table 3)
summary statistics on intermolecular distances, potential ener- but higher computational tractability. The machine learning model
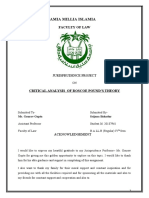
Fig. 1 | High-throughput screening of solid drug nanoparticles and machine learning model development. a, A schematic of the high-throughput
experimental workflow to create nanoparticles using a nanoprecipitation technique and rapid assessment using DLS. b, Left: high-throughput testing of
all 1,440 combinations of 16 drugs and 90 excipients (inactive ingredients, generally recognized-as-safe food and drug additives and other FDA-approved
compounds). The colour gradient indicates a size reduction of the nanoparticle compared with the unformulated drug, where white corresponds to
less than a 50% reduction in size, and black corresponds to a 90% reduction in size with linear interpolation (cf. colour bar at bottom). Right: machine
learning-based assessment of nanoparticle-forming potential of drug–excipient pairs according to their chemical structures, physicochemical properties
and pairwise interaction potential determined from short MD simulations. The gradient indicates predictive confidence from tenfold cross-validation
(white 0% confidence, black 100% confidence, linear interpolation, cf. colour bar at bottom). We found good agreement between the computational
assessments (right) and the real-world experimentation (left), with 91% of the experiments correctly predicted. DBU, diazabicycloundecene. c, A
schematic explaining the relationship of MD simulations and machine learning. The MD simulations of drug–excipient systems are computationally
analysed to quantify non-covalent interaction potentials. These potentials serve as input for our machine learning model. The machine learning model
uses both these interaction potentials and the molecular properties of drugs and excipients to predict which drug–excipient pairs will most likely lead to
nanoparticle formation. Furthermore, the analysis of the predictive architecture of the machine learning model enables us to determine the most important
variables that govern co-aggregation prediction (Supplementary Table 4). In a separate analysis, MD trajectories were analysed to identify the most
relevant non-covalent interactions for different drug–excipient pairs (Supplementary Table 8). d, Performance analysis of the machine learning model
trained on different training dataset sizes. Shown is the mean Matthews correlation coefficient (MCC) of 20 independent models trained on randomly
selected data subsets. e, Using the developed computational prediction model, we predicted 2.1 million pairs constituting all exhaustive combinations
of 788 drugs each paired with one of 2,686 excipients. The machine learning model predicted that a majority of the drugs and excipients would not
co-aggregate, resulting in colloidal self-aggregation of the drug and precipitation. For 38,464 combinations (1.8%), the machine learning model predicted a
potential interaction between the drug and the excipient, leading to formation of a stabilized, co-assembled nanoparticle. Some excipients (blue dots) are
predicted to enable creation of nanoparticles with many different drugs (red dots) while other excipients were predicted to be able to create nanoparticles
with only a single drug. The node size corresponds to the number of predicted excipients/drugs enabling formation of nanoparticles with this compound.
Combinations further characterized in this paper are highlighted with purple edges and are numbered I–VI (cf. Fig. 2) and labelled with the corresponding
drug and excipient constituting this pair. The novel component that was not previously used in the screen is underscored.
726 Nature Nanotechnology | VOL 16 | June 2021 | 725–733 | www.nature.com/naturenanotechnology
NaTure NanOTecHnOlOgy Articles
predicted a total of 38,464 combinations (1.8% of all possible pairs) revealed a range of complex microstructures (Fig. 2a). When mix-
to co-aggregate into nanoparticles (Fig. 1e). ing the drugs with the excipients, DLS indicated the formation of
monodisperse, nano-sized co-aggregates (Supplementary Table 7).
In-silico-designed nanoparticles improve drug dispersion Using TEM, we imaged the drug–excipient samples and con-
We selected six of the co-aggregation predictions for experimen- firmed that co-aggregation of the selected drugs and excipients
tal testing, specifically selecting novel excipients (Fig. 2, I–III), new formed homogeneous populations of nanoparticles (Fig. 2b). None
drugs (Fig. 2, IV and V) or combinations of a novel drug and excipi- of the co-aggregation acquisitions were flagged, suggesting stable
ent (Fig. 2, VI). We used DLS to measure the size of the colloidal nanoparticle dispersions (Supplementary Table 7).
self-aggregates of the selected drugs. All six drugs self-aggregated To further assess the stability of nanoparticle dispersions, we
into micrometre-sized, polydisperse structures (Supplementary escalated nanoparticle concentrations by increasing drug and
Table 7). A large number of automatically flagged acquisitions for excipient concentration while maintaining drug-to-excipient
these drug aggregates suggested interference with the measurement ratios during production. With the exception of nelfinavir–ribo-
through precipitation. Transmission electron microscopy (TEM) flavin, all of the nanoparticulate co-aggregates exhibited clear or
a b
Chlorpromazine HCl
Chlorpromazine HCl
Lumefantrine
Lumefantrine
Atovaquone
Atovaquone
Clofazimine
Clofazimine
Rapamycin
Rapamycin
Fulvestrant
Fulvestrant
Curcumine
Curcumine
Pranlukast
Pranlukast
Econazole
Econazole
Rilpivirine
Rilpivirine
Sorafenib
Sorafenib
Etravirine
Etravirine
Nelfinavir
Nelfinavir
Physcion
Physcion
Gefitinib
Gefitinib
Taxol
Taxol
Caffeine Caffeine
Succinic acid Succinic acid
Octyl gallate Octyl gallate
DL-malic acid DL-malic acid
Adipic acid Adipic acid
10 nmol Add drug Mixing Solvent DLS Triazabicyclodecene Triazabicyclodecene
excipient 10 nmol exchange DBU DBU
L-asparagine L-asparagine
Theobromine Theobromine
3,3'-Thiodipropionic acid 3,3'-Thiodipropionic acid
Theophylline Theophylline
Borneol Borneol
Cinnamaldehyde Cinnamaldehyde
Aspartame Aspartame
c Squalene
Benzaldehyde
Squalene
Benzaldehyde
Interaction potentials Sodium deoxycholate Sodium deoxycholate
Cholic acid Cholic acid
Glycocholic acid Glycocholic acid
Feature analysis Sucrose octaacetate Sucrose octaacetate
Molecular simulations Trans-anethole Trans-anethole
Machine learning Indomethacin Indomethacin
Terpinyl butyrate Terpinyl butyrate
Molecular properties
New predictions Hydrocortisone Hydrocortisone
Candesartan cilexetil Candesartan cilexetil
Neohesperidin DC Neohesperidin DC
Ursodiol Ursodiol
Diclofenac Diclofenac
Eucalyptol Eucalyptol
Beta-carotene Beta-carotene
Menthol Menthol
d Alpha-terpineol Alpha-terpineol
Fenchyl alcohol Fenchyl alcohol
0.3 Biotin Biotin
Model performance
Xylitol Xylitol
(out-of-bag MCC)
Trans-cinnamic acid Trans-cinnamic acid
0.2 Thimerosal Thimerosal
Tyramine Tyramine
Fumaric acid Fumaric acid
0.1 Congo red Congo red
Vanillin Vanillin
Saccharin Saccharin
0 Allantoin Allantoin
Vitamin A palmitate Vitamin A palmitate
Acetylcholine chloride Acetylcholine chloride
200 400 600 800 1,000 1,200 1,400 Dibutyl phthalate Dibutyl phthalate
Size of training dataset Trometamol Trometamol
Benzoyl peroxide Benzoyl peroxide
Triethyl citrate Triethyl citrate
Triacetin Triacetin
e Glycerol
Propylene glycol
Glycerol
Propylene glycol
Mebendazole Mebendazole
L-proline L-proline
L-lysine L-lysine
L-ascorbic acid L-ascorbic acid
Stearic acid Stearic acid
(R)-(+)-Limonene (R)-(+)-Limonene
Meglumine Meglumine
Hydrochlorothiazide Hydrochlorothiazide
Ketoprofen Ketoprofen
Memantine HCl Memantine HCl
III Nelfinavir and riboflavin Naproxen sodium Naproxen sodium
Mannitol Mannitol
D-sorbitol D-sorbitol
Tannic acid Tannic acid
Atovaquone and Rhodamine B Rhodamine B
II α-tocopherol Moxifloxacin Moxifloxacin
Ciprofloxacin Ciprofloxacin
Certirizine Certirizine
Budesonide Budesonide
Etidronic acid Etidronic acid
Emtricitabine Emtricitabine
Metoprolol-(+)-tartrate Metoprolol-(+)-tartrate
Phenytoin Phenytoin
Propranolol HCl Propranolol HCl
Danazol and tannic acid Captan Captan
IV Neotame Neotame
Alendronate sodium Alendronate sodium
Piroxicam Piroxicam
Sorafenib and Desipramine HCl Desipramine HCl
glycyrrhizin I Nadolol Nadolol
VI Terbinafine and Omeprazole Omeprazole
taurocholic acid Labetalol HCl Labetalol HCl
Prednisone Prednisone
Risperidone Risperidone
Fluconazole Fluconazole
Methotrexate hydrate Methotrexate hydrate
Tenofovir alafenamide Tenofovir alafenamide
V Carbamazepine Carbamazepine
Celecoxib and indomethacin 50 1 0 100
Size (% control) Confidence (%)
High-throughput Computational
experimentation predictions
Nature Nanotechnology | VOL 16 | June 2021 | 725–733 | www.nature.com/naturenanotechnology 727
Articles NaTure NanOTecHnOlOgy
a b c d e
Sorafenib Sorafenib and glycyrrhizin
+ Glycyrrhizin
concentration (%)
100
Sorafenib
I 50 Pure sorafenib
0
1 µm 500 nm Sorafenib + Glycyrrhizin
0 2 4 6 8
Time (h)
Atovaquone Atovaquone and α-Tocopherol
concentration (%)
100
Atovaquone
+ α-Tocopherol
50 Pure
II atovaquone
0
2 µm 2 µm Atovaquone + α-Tocopherol 0 50 100 150 200
Time (min)
Nelfinavir Nelfinavir and riboflavin
concentration (%)
100 Pure nelfinavir
Nelfinavir
III 50 + Riboflavin
Nelfinavir + Riboflavin 0
1 µm 500 nm 0 50 100 150 200
Time (min)
Danazol Danazol and tannic acid
concentration (%)
100 + Tannic acid
Danazol
IV 50
Pure
danazol
0
2 µm 2 µm Danazol +Tannic acid 0 50 100 150 200
Time (min)
Celecoxib Celecoxib and indomethacin
concentration (%)
100
+ Indomethacin
Celecoxib
50
V
Pure celecoxib
Celecoxib + Indomethacin 0
2 µm 2 µm 0 20 40 60
Time (min)
Terbinafine Terbinafine and taurocholic acid
+ Taurocholic acid
concentration (%)
100
Terbinafine
VI 50
Pure terbinafine
+ Taurocholic 0
1 µm 1 µm Terbinafine acid 0 2 4 6 8
Time (h)
Fig. 2 | Computationally prioritized combinations of drugs and excipients form nanoparticles. Numbering corresponds to edges highlighted in Fig. 1e.
Nanoparticle formation was primarily evaluated using DLS (Supplementary Table 7). a,b, These data were further validated using TEM images of
micrometre-sized aggregates formed by the pure drug (a), and TEM images of the nanoparticles formed by co-aggregating the drugs and excipients (b).
c, Photos show dispersion of the nanoparticles compared with unformulated drug during concentration escalation experiments. d, Dispersion stability
was quantified by analysing time–concentration curves according to OECD guidelines. e, Short MD simulations map non-covalent interaction potential
between drugs and excipients. In the MD visualizations, drugs are visualized through black van der Waals spheres, while excipients are visualized through
transparent and coloured van der Waals spheres. For a–c, representative images are shown from ten acquisitions generated through two independent
experiments, and all images reproduced the here depicted behaviour.
728 Nature Nanotechnology | VOL 16 | June 2021 | 725–733 | www.nature.com/naturenanotechnology
NaTure NanOTecHnOlOgy Articles
milky dispersions at high drug concentrations up to 1 mM; drugs Sorafenib nanoparticles improve anticancer efficacy in vivo
without excipients precipitated rapidly (Fig. 2c). Since visibility For our second proof-of-concept study, we selected sorafenib nano-
of precipitation is a subjective measure, we followed established formulations. Sorafenib is a multi-kinase inhibitor used as a thera-
protocols from the Organisation for Economic Cooperation and peutic to treat several types of cancer and the standard of care for
Development (OECD) to quantitatively assess nanoparticle disper- front line therapy of advanced hepatocellular carcinoma (HCC)30.
sion stability (Supplementary Fig. 5)21. The nanoparticles formed However, given modest clinical efficacy of sorafenib and due to
stable dispersions as indicated by maintaining high drug concentra- increasing incidence rate31 and poor prognosis of HCC30, there is
tions for longer time periods compared with the drugs without the a pressing clinical need for new therapeutic options. Nanoparticles
excipients, with the exception of nelfinavir (Fig. 2d). The excipients have been shown to improve sorafenib efficacy11, which motivated
remained highly soluble throughout the duration of the experiment us to use our platform to identify sorafenib nanoparticles.
(Supplementary Fig. 6). We decided to contextualize our predicted stabilizer glycyr-
To investigate the non-covalent forces that govern co-aggregation, rhizin against the screening hits candesartan cilexitel, indometha-
we conducted additional MD simulations using our established cin and tannic acid. Meloxicam, a low-confidence prediction,
parameters for larger systems of 20 drug and 20 excipient molecules was included since it represents a cyclooxygenase inhibitor like
(Fig. 2e). Every drug–excipient system interacted with distinct pat- indomethacin. Although none of these molecules had been used
terns of specific non-covalent forces, suggesting that co-aggregation as excipients in self-assembling nanoparticles before, they are
of our nanoparticles is governed by complex molecular-recognition well understood to be safe or have been proposed for clinical
mechanisms and through various non-covalent interactions use together with sorafenib. Although glycyrrhizin is a known
(Supplementary Table 8). 11β-hydroxysteroid dehydrogenase inhibitor associated with
reversible hypermineralocorticoid-like effects after intensive con-
Terbinafine particles for antifungal applications sumption, it is still considered a safe food and drug ingredient with
Onychomycosis is the most common nail disorder observed in daily consumption of up to 3.6 mg kg−1 (ref. 32). Tannic acid is ‘gener-
clinical practice22. Terbinafine is an antifungal drug used to treat ally regarded as safe’14. Candesartan has been co-administered clini-
cutaneous mycoses, including onychomycosis. It can be given orally cally with sorafenib to counter sorafenib-associated hypertension33.
or topically; however, its effectiveness is limited in oral applications Cyclooxygenase inhibitors such as meloxicam and indomethacin
due to systemic toxicity and in topical applications due to low tissue have been studied as synergistic enhancers of the anticancer effects
penetration23. We hypothesized that our terbinafine–taurocholic of sorafenib34,35. Formulating sorafenib with such drugs might con-
acid nanoparticles could increase skin penetration of terbinafine, stitute an important step towards excipient-free formulations where
thereby increasing topical efficiency. all included materials serve a therapeutic purpose5. Using DLS
Using TEM, we observed distinct aggregation dynamics with and TEM, we measured the size of the co-assembled nanoparticles
populations of different types of low density nanoparticles forming. created with the five excipients; all nanoparticles had radii below
Through timed TEM imaging, we identified three different types of 100 nm (Fig. 4a and Supplementary Table 10), complying to strin-
nanostructures corresponding to different phases of the nanopar- gent nanoformulation thresholds36. All particles enabled full drug
ticle formation process (Fig. 3a). The particles grew over the course dispersion over 8 h (Fig. 4b), except for meloxicam which provided
of several hours, most likely through condensation or coagulation24. only marginal stability. DLS indicated a potentially longer stability
We hypothesized that the particles could nevertheless provide use- beyond 8 h for stable particles (Supplementary Table 11).
ful materials since these growth dynamics were sufficiently slow to We applied our particles in a cellular phenotypic screen. The
warrant the biochemical application of fresh particles11,25. nanoparticles exhibited significantly higher cytotoxicity in human
We purified the nanoparticles using centrifugation. The liver carcinoma HUH7 with twofold more potent half-maximum
particles exhibited low density and precipitated in the supernatant. inhibitory concentration (IC50) values compared with the unformu-
Analytics of the purified nanoparticles revealed high encapsula- lated drug (Fig. 4c). We confirmed that nanoparticle formation did
tion efficiency (75.6 ± 0.4%) and drug loading (93.0 ± 0.5% w/w) not prevent sorafenib from engaging with one of its main targets,
(Supplementary Table 9). We performed a chemical analysis using Raf1, by observing an equivalent inhibition of MEK phosphoryla-
scanning transmission electron microscopy-energy dispersive spec- tion compared with free sorafenib (Supplementary Fig. 8).
troscopy and found that the nanoparticles contained sulfur from With the exception of tannic acid, none of the utilized excipi-
the excipient taurocholic acid, providing further evidence that the ents showed significant cytotoxicity in HUH7 alone (Fig. 4c inset
nanoparticles are indeed co-aggregates of drugs and excipients and Supplementary Fig. 9), ruling out additive effects leading to the
(Supplementary Fig. 7). increased cytotoxicity. Instead, we proposed that the nanoparticles
Next, we tested whether the nanoparticles would retain the enable higher drug uptake compared with the larger microscale
fungistatic effect of terbinafine against Candida albicans, a major structures formed by unformulated sorafenib (Supplementary
source of onychomycosis in immunocompromised individu- Fig. 10). The glycyrrhizin particles most significantly improved
als26. Measuring in vitro viability for C. albicans revealed a sig- drug availability and almost doubled cytosolic sorafenib content
nificant effect of our nanoparticles compared with the vehicle (Fig. 4d), potentially enhanced by glycyrrhizin’s ability to target
and non-treatment control, while terbinafine alone showed no hepatocytes37. Inhibiting caveolin-mediated endocytosis strongly
significant difference to any treatment (one-way analysis of vari- reduced particle uptake while modulation of clathrin-mediated
ance (ANOVA) P = 0.017, Tukey’s post hoc P < 0.05). Our particles endocytosis did not affect uptake (Fig. 4e).
halted biofilm formation with slightly higher but comparable effi- We purified our particles using centrifugation, which revealed
ciency compared with free terbinafine; the excipient alone was not that the nanoparticles had high drug loading (94.9 ± 1.2%) and
fungistatic (Fig. 3b,c). encapsulation efficiency (92.6 ± 0.6%) (Supplementary Table 12).
Skin uptake of our nanoparticles was twice that of free terbin- Using scanning transmission electron microscopy-energy disper-
afine (Fig. 3d), possibly due to higher diffusivity of the smaller par- sive spectroscopy, we observed that the particles contained fluo-
ticles as expected according to the Stokes–Einstein equation27,28 or rine from sorafenib (Supplementary Fig. 11), confirming that the
through permeation enhancement caused by the excipient tauro- particles were enriched with drug as expected from the analytics
cholic acid29. Taken together, our data suggested that our nanopar- (Supplementary Table 12). Using DLS, we observed that the par-
ticles can retain the fungistatic activity of free terbinafine while ticles were stable in serum and cell media and were not disrupted
locally increasing bioavailability. by shearing forces when administered through a 29-gauge needle or
Nature Nanotechnology | VOL 16 | June 2021 | 725–733 | www.nature.com/naturenanotechnology 729
Articles NaTure NanOTecHnOlOgy
a c
Terbinafine + Taurocholic acid No drug
1 min
10 min
100 min
1 µm 1,000 min
500 µm
b Terbinafine
Free terbinafine NS
150
C. albicans survival (% control)
Terbinafine and
* NS
taurocholic acid
100
Taurocholic acid * NS *
No treatment
Free terbinafine
Terbinafine and
taurocholic acid
50
0 500 µm
0 2.5 25 250
Concentration (µM)
d Terbinafine + taurocholic acid
*
Terbinafine uptake (ng cm–2)
600
400
200
0
ug
id
ac
dr
re
lic
500 µm
Pu
ho
oc
ur
Ta
+
Fig. 3 | Characterization and ex vivo application of terbinafine and taurocholic acid particles. a, Left: TEM images of terbinafine alone. Right:
nanoparticles formulated together with taurocholic acid are shown in TEM images taken at different time points after co-assembly initiation. The scale
bar corresponds to 1 µm, and the scale is consistent across images. b, C. albicans survival after treatment with terbinafine alone (black), terbinafine and
taurocholic acid nanoparticles (red) or pure taurocholic acid (formulation control, light grey). Concentrations indicate terbinafine and/or taurocholic acid
concentration. XTT readouts were normalized according to the untreated control (100% survival, 1% DMSO in PBS, hollow circles), n = 4 independent
samples, lines correspond to mean values and error bars represent one standard deviation. We performed a one-way ANOVA (P = 0.017) followed by
Tukey’s post hoc test and found that terbinafine alone shows no significant difference to any other condition while terbinafine–taurocholic acid significantly
reduced C. albicans viability compared with the control treatments. NS, statistical insignificance (P > 0.05); * indicates statistical significance (P < 0.05)
c, Microscopic images of C. albicans after 17 h of nanoparticle treatment or terbinafine treatment compared with the untreated control. d, Skin uptake of
terbinafine into porcine ear skin in Franz diffusion cell measurements, n = 3 independent samples and P = 0.028 two-sided t-test. Lines correspond to
mean values; error bars represent one standard deviation. * indicates statistical significance (P < 0.05). For a and c, representative images are shown from
ten acquisitions generated through two independent experiments, and all images reproduced the here depicted behaviour.
by centrifugation followed with ultrasound-mediated redispersion model of spontaneous HCC38,39, the most common type of liver
(Supplementary Fig. 12). cancer. Tumourigenesis is induced by an overexpression of human
We refined our formulation protocol to consistently gener- ΔN90-β-catenin and human MET genes in the mouse liver and
ate nanoparticles containing 3 mg ml−1 sorafenib (Supplementary represents an aggressive model of HCC characterized by rapid
Fig. 13), which enabled us to dose 30 mg kg−1 for intravenous formation of a large number of tumour nodules38. We chose this
injection. In a toxicity analysis, our formulation did not induce model because it correlates more strongly with clinical outcomes
abnormal liver function after three injections of elevated dos- compared with simpler xenograft-based models39–41.
ages of 60 mg kg−1 (Supplementary Table 13). Next, we compared HCC-bearing mice were treated three times a week (t.i.w.) for
the in vivo antitumour efficacy of our sorafenib–glycyrrhizin four weeks with our nanoparticle formulations or control treat-
nanoparticles to sorafenib alone in an established genetic mouse ments (Fig. 4f). We tracked alpha-fetoprotein (AFP) levels, a marker
730 Nature Nanotechnology | VOL 16 | June 2021 | 725–733 | www.nature.com/naturenanotechnology
NaTure NanOTecHnOlOgy Articles
of HCC progression and transformed hepatocytes42. While no dif- therapeutic benefit was sorafenib solubilized in cremophor–ethanol
ferences were visible during the early stages of treatment, at week 10 (Supplementary Fig. 18); however, the adverse toxicity of cremo-
the sorafenib–glycyrrhizin nanoparticles showed a successful reduc- phor is an important limitation of this formulation44.
tion in serum AFP levels (Fig. 4g). We observed a similar reduction For pharmacokinetic characterization, we measured the concen-
of AFP in mice receiving only glycyrrhizin (Supplementary Fig. 14), tration–time course of sorafenib in blood, liver, lung, spleen and
which is potentially caused by the known hepatoprotective effects kidney after administering our sorafenib–glycyrrhizin particles to
of glycyrrhizin43. This is encouraging since, although we know glyc- healthy mice (Supplementary Note 4). We compared our formu-
yrrhizin does not target HCC directly (Fig. 4c and Supplementary lation to oral administration of sorafenib and to an intravenous
Fig. 9), it indicates a potential for glycyrrhizin to act as a functional injection of sorafenib dissolved in cremophor–ethanol (Fig. 4i and
adjuvant. The control treatment of sorafenib dissolved in cremo- Supplementary Fig. 19). Our sorafenib–glycyrrhizin particles sig-
phor–ethanol had no effect on AFP levels (Supplementary Fig. 15). nificantly improved liver targeting (Fig. 4i inset and Supplementary
Body weight data suggested that mice treated with sorafenib–glyc- Note 5). Other researchers have shown a preferred accumulation
yrrhizin nanoparticles had a significantly reduced tumour bur- of similar nanoparticles in the lung11,25, suggesting that liver accu-
den (Supplementary Fig. 16) compared with control treatments mulation of these particles is driven by physicochemical differ-
(Supplementary Fig. 17), but we cannot exclude that the body ences between our formulation and those previously reported.
weight difference is at least in part impacted by confounding vari- Overall, our data suggest that this hepatic targeting, combined
ables such as loss of appetite. with endocytosis-driven active drug uptake of the nanoparticles
We evaluated treatment efficacy based on the calculation of into HCC cells (Fig. 4e) and the ability of the particles to release
morbidity-free survival fractions using the Kaplan–Meier method. sorafenib to act on its established pathways (Supplementary Fig. 8),
Mice treated with sorafenib–glycyrrhizin nanoparticles had sig- can explain the improved treatment efficacy of our nanoparticles
nificantly longer morbidity-free survival (P = 0.0032, logrank test) (Fig. 4h).
compared with mice treated with the vehicle control (intravenous
injections of glycyrrhizin in 1% dimethyl sulfoxide (DMSO) in Conclusion
phosphate-buffered saline (PBS)) or mice receiving oral sorafenib Small-molecule-based nanoparticle systems are an important addi-
(Fig. 4h). The only other control treatment that showed any tion to nanomedicine, enabling rapid generation of highly loaded
Fig. 4 | Characterization and in vivo application of sorafenib nanoparticles. a, TEM images of colloidal aggregates formed by unformulated sorafenib
(left) compared with TEM images of nanoparticles formulated with glycyrrhizin, candesartan cilexitel, indomethacin, tannic acid and meloxicam (right).
Scale bar corresponds to 200 nm, and the scale is consistent over all images. A coloured border was added to visually aid identification of nanoparticles
across all panels. Representative images are shown from ten acquisitions generated through two independent experiments, and all images reproduced
the here depicted behaviour. b, Dispersion of sorafenib alone and in nanoformulation with excipients, measured as a concentration–time curve by HPLC.
The percentages for nanoparticles reflect encapsulation efficiency. There were n = 2 independent samples. c, HUH7 human HCC cell survival after
48 h of treatment with different nanoparticles (colours as in b) or free sorafenib. Dose–response curves were fitted in Prism using the inhibitor versus
response (three parameters) model. Sorafenib IC50 = 14 ± 1.1 μM, sorafenib and glycyrrhizin IC50 = 6.2 ± 0.6 μM, sorafenib and candesartan cilexetil
IC50 = 8.7 ± 0.7 μM, sorafenib and indomethacin IC50 = 8.4 ± 0.8 μM and sorafenib and tannic acid IC50 = 7.3 ± 0.7 μM for n = 10 independent samples.
Graphs on the right show box plots of individual measurements (P = 0.0013 two-way ANOVA). The nanoparticle formations were significantly more
potent compared with unformulated sorafenib at all tested concentrations above 6 μM (P < 0.05, Dunnett’s multiple comparisons test). The box extends
from the 25th to 75th percentiles, the line is the median and whiskers extend from maximal to minimal measurement. The inset shows HUH7 viability
after 48 h of incubation with 50 μM excipients only (coloured symbols) or buffer control (hollow diamonds). The difference to buffer control was
evaluated using Dunnett’s multiple comparisons test. Lines correspond to mean values; error bars represent one standard deviation. n = 4 independent
samples. d, Cytosolic sorafenib in HUH7 cells after 2 h incubation with unformulated sorafenib (black), sorafenib-tannic acid particles (orange),
sorafenib-indomethacin particles (blue) or sorafenib–glycyrrhizin particles (green). All treatments were added at 100 μM. n = 5 independent samples,
P = 0.016 one-way ANOVA. Lines correspond to mean values; error bars represent one standard deviation. e, Independent uptake mechanism study
with same experimental conditions as in d but including endocytosis inhibitors sucrose or methyl-beta-cyclodextrin. Sucrose inhibits clathrin-dependent
endocytosis, which did not affect cytosolic sorafenib levels (P = 0.52, Dunnett’s multiple comparisons test). Methyl-beta-cyclodextrin inhibits
caveolin-mediated endocytosis and significantly reduced cytosolic sorafenib levels (P < 0.0001, Dunnett’s multiple comparisons test). P < 0.0001
one-way ANOVA. n = 6 independent samples. Lines corresponds to mean values; error bars represent one standard deviation. f, A schematic of the in vivo
experiment. The tumour was induced by injection of oncogene-coding plasmids. Five weeks after induction, AFP levels were determined to assess tumour
progression and enable group randomization. Mice were randomized according to AFP levels and then treated three times a week (t.i.w.) for four weeks.
Treatments were 30 mg kg−1 sorafenib–glycyrrhizin nanoparticles, 30 mg kg−1 sorafenib oral, 30 mg kg−1 sorafenib in cremophor–ethanol, glycyrrhizin
vehicle control, cremophor–ethanol vehicle control and 1% DMSO in PBS buffer control. AFP levels were measured at week 7 and week 10 to assess
tumour progression during the treatment period (cf. panel g). After this final intervention, mice were monitored for morbidity-free survival (cf. panel h).
g, AFP levels of mice after receiving sorafenib–glycyrrhizin nanoparticles, oral sorafenib or 1% DMSO in PBS buffer control. AFP levels were compared at
the beginning of treatment (week 5), during treatment (week 7) and at end of treatment (week 10). P = 0.027 two-way ANOVA, significance levels shown
for Tukey’s multiple comparisons test for all possible treatment comparisons, n = 12, 7 and 5 for independent animals for sorafenib–glycyrrhizin, vehicle
control and oral sorafenib, respectively. The lines correspond to mean values; error bars represent one standard deviation. h, Kaplan–Meyer analysis shows
that mice treated with sorafenib–glycyrrhizin nanoparticles show longer morbidity-free survival (P = 0.0032, logrank Mantel–Cox test) compared with
oral sorafenib and the glycyrrhizin-only vehicle control, n = 12 independent animals for sorafenib–glycyrrhizin and vehicle control, n = 5 for oral sorafenib.
i, Biodistribution analysis of sorafenib tissue accumulation for sorafenib–glycyrrhizin nanoparticles (green) compared with oral sorafenib administration
(white) and sorafenib dissolved in cremophor–ethanol (grey). The AUC for sorafenib–glycyrrhizin is compared with the two other treatments per tissue
using Dunnett’s multiple comparisons test. P < 0.0001 two-way ANOVA. The inset shows the relative sorafenib content of liver compared with blood.
Sorafenib–glycyrrhizin nanoparticles show significantly better targeting to the liver compared with sorafenib in cremophor–ethanol (P = 0.014, Tukey’s
multiple comparisons test) and oral sorafenib (P = 0.0012, Tukey’s multiple comparisons test). P = 0.0014 one-way ANOVA, n = 3 independent animals
per condition and timepoint. Lines correspond to mean values; error bars represent one standard deviation. For c, d, e, g and i, NS indicates statistical
insignificance (P > 0.5, might be ommited for readability). *P < 0.05, **P < 0.01, ***P < 0.001, ****P < 0.0001.
Nature Nanotechnology | VOL 16 | June 2021 | 725–733 | www.nature.com/naturenanotechnology 731
Articles NaTure NanOTecHnOlOgy
nanocarriers for life-saving therapeutics10,11. High drug loading will rates24. If such conditions can be controlled, dynamic changes to the
ultimately reduce the risk of excipient-triggered adverse reactions9 nanoparticles might be harnessed for adaptive delivery solutions48.
and reduce administered volumes, improving adherence and quality To improve the selection of specific nanoparticles for various
of life45. With machine learning and high-throughput experimenta- applications, it would be useful to have methods that predict physi-
tion (Supplementary Note 6), we broaden the scope of this technol- cal properties of these nanoparticles. Investigating focused sets of
ogy and include a wide array of different types of drugs treating nanoparticles can enable size prediction11. We have provided further
various diseases. Using FDA-approved excipients such as vitamins, evidence that nanoparticle size can correlate with particle stability
nutrients and food compounds generates nanoformulations with (Figs. 2 and 4). Furthermore, our data suggest that predictive uncer-
potential for accelerated translation into humans. tainty measures (cf. meloxicam in Fig. 4) as well as MD analysis (cf.
Under fixed conditions, co-aggregation can be conducted in riboflavin in Fig. 2) can be used to anticipate nanoparticle stability.
a highly reproducible manner (Supplementary Fig. 13) with low Models that could anticipate more complex properties such as bio-
dispersity (Supplementary Tables 7 and 10). An important chal- distribution and release kinetics would further facilitate nanopar-
lenge and opportunity lies in the context-sensitive nature of the ticle selection. Finally, further maturing the described materials, for
self-assembly process. Buffer conditions such as pH, temperature example, to enable functionalization and encapsulation of hydro-
and salt concentrations can significantly alter the co-aggregation philic drugs (Supplementary Note 7), will expand the number of
propensity of the materials2,3,46. Variations of these conditions possible applications of these co-aggregates. By accelerating the
during manufacturing could further broaden the scope of such development of nanomedicines, we anticipate that the approach
platforms and include materials currently unsuitable for simple reported herein and extensions thereof will be an important step
co-precipitation. towards personalized drug delivery9.
In addition, aggregation context can provide further opportu-
nities for the development of adaptive systems that co-aggregate Online content
specifically in situ, for example in gastric conditions47. This might Any methods, additional references, Nature Research report-
ultimately enable responsive systems. For example, we had observed ing summaries, source data, extended data, supplementary infor-
that some of our aggregates grew when heated (Supplementary mation, acknowledgements, peer review information; details of
Fig. 20), potentially due to Ostwald ripening and elevated collision author contributions and competing interests; and statements of
Viability (% control)
a b c
0 50 100
90 + Glycyrrhizin
+ Candesartan cilexitel 100 ***
NS
+ Tannic acid
HUH7 viability (% control)
Sorafenib 85 NS
+ Indomethacin **
+ Glycyrrhizin
80 Methanol
concentration (%)
Candesartan
+ 100 ****
cilexitel ****
****
Sorafenib
+ Indomethacin 50 ****
50 + Meloxicam
1
Viability
+ Tannic acid ****
****
Sorafenib *
***
+ Meloxicam 0 0
50 µM vehicle ****
2 4 6 8 0
****
Time (h) 1 10 100 ****
***
Sorafenib concentration (µM) **
d e f
25 ** ****
Sorafenib content (µg ml–1)
Sorafenib content (µg ml–1)
25
/protein content (mg ml–1)
/protein content (mg ml–1)
20 20
Tumour
30 mg kg–1
15 15 induction Survival study
treatment
10 10
0 5 10 15 Weeks
5 5
0 0
AFP AFP AFP
cy eth ose
tri -
Su itor
n
b
in
ex ta
id
ci
ni
iz
od be
n
ac
ha
b
fe
M ccr
rh
hi
cl yl-
ra
et
yr
ic
in
so
nn
o
ly
do
N
Ta
µM
G
In
+
+
0
+
10
* **
g h i 3
Sorafenib + glycyrrhizin
1% DMSO PBS 2
AFP fold change (% control)
***
Ratio
400 100
Sorafenib AUC (ng × h ml–1)
Oral sorafenib 200
****
NS
* 1
30 mg kg–1 t.i.w. *
Survival (%)
300 150
****
–1
30 mg kg sorafenib 0
NS
Liver/blood
NS
200 50 t.i.w. + glycyrrhizin
sorafenib 100 *
(P = 0.0032)
NS
100 * + Glycyrrhizin
NS
NS
50
Glycyrrhizin + Cremophor
0 0 Oral sorafenib
0
80 90 100 110
10
5
Time (d)
d
ng
y
k
ve
ne
oo
e
ee
ee
Lu
le
ee
Li
d
Bl
W
Sp
Ki
W
732 Nature Nanotechnology | VOL 16 | June 2021 | 725–733 | www.nature.com/naturenanotechnology
NaTure NanOTecHnOlOgy Articles
data and code availability are available at https://doi.org/10.1038/ 25. Ganesh, A. N. et al. Colloidal drug aggregate stability in high serum conditions
s41565-021-00870-y. and pharmacokinetic consequence. ACS Chem. Biol. 14, 751–757 (2019).
26. Jayatilake, J. A. M. S., Tilakaratne, W. M. & Panagoda, G. J. Candidal
onychomycosis: a mini-review. Mycopathologia 168, 165–173 (2009).
Received: 29 September 2019; Accepted: 28 January 2021; 27. Cabral, H. et al. Accumulation of sub-100 nm polymeric micelles in poorly
Published online: 25 March 2021 permeable tumours depends on size. Nat. Nanotechnol. 6, 815–823 (2011).
28. Wong, C. et al. Multistage nanoparticle delivery system for deep penetration
References into tumor tissue. Proc. Natl Acad. Sci. USA 108, 2426–2431 (2011).
1. Hopkins, A. L., Keserü, G. M., Leeson, P. D., Rees, D. C. & Reynolds, C. H. 29. Pavlović, N. et al. Bile acids and their derivatives as potential modifiers of
The role of ligand efficiency metrics in drug discovery. Nat. Rev. Drug Discov. drug release and pharmacokinetic profiles. Front. Pharmacol. 9, 1283 (2018).
13, 105–121 (2014). 30. Villanueva, A. Hepatocellular carcinoma. N. Engl. J. Med. 380, 1450–1462
2. Irwin, J. J. et al. An aggregation advisor for ligand discovery. J. Med. Chem. (2019).
58, 7076–7087 (2015). 31. El-Serag, H. B. & Mason, A. C. Rising incidence of hepatocellular carcinoma
3. Reker, D., Bernardes, G. J. L. & Rodrigues, T. Computational advances in in the United States. N. Engl. J. Med. 340, 745–750 (1999).
combating colloidal aggregation in drug discovery. Nat. Chem. 11, 32. Isbrucker, R. A. A. & Burdock, G. A. A. Risk and safety assessment on the
402–418 (2019). consumption of Licorice root (Glycyrrhiza sp.), its extract and powder as a
4. Owen, S. C., Doak, A. K., Wassam, P., Shoichet, M. S. & Shoichet, B. K. food ingredient, with emphasis on the pharmacology and toxicology of
Colloidal aggregation affects the efficacy of anticancer drugs in cell culture. glycyrrhizin. Regul. Toxicol. Pharm. 46, 167–192 (2006).
ACS Chem. Biol. 7, 1429–1435 (2012). 33. Basso, U., Brunello, A., Bertuzzi, A. & Santoro, A. Sorafenib is active on lung
5. Kipp, J. E. The role of solid nanoparticle technology in the parenteral delivery metastases from synovial sarcoma. Ann. Oncol. 20, 386–387 (2009).
of poorly water-soluble drugs. Int. J. Pharm. 284, 109–122 (2004). 34. Chaparro, M., González Moreno, L., Trapero-Marugán, M., Medina, J. &
6. Mcdonald, T. O. et al. Antiretroviral solid drug nanoparticles with enhanced Moreno-Otero, R. Review article: pharmacological therapy for hepatocellular
oral bioavailability: production, characterization, and in vitro-in vivo carcinoma with sorafenib and other oral agents. Aliment. Pharm. Ther. 28,
correlation. Adv. Healthc. Mater. 3, 400–411 (2014). 1269–1277 (2008).
7. Govender, T., Stolnik, S., Garnett, M. C., Illum, L. & Davis, S. S. PLGA 35. Zhong, J. et al. Meloxicam combined with sorafenib synergistically inhibits
nanoparticles prepared by nanoprecipitation: drug loading and release studies tumor growth of human hepatocellular carcinoma cells via ER stress-related
of a water soluble drug. J. Control. Release 57, 171–185 (1999). apoptosis. Oncol. Rep. 34, 2142–2150 (2015).
8. Westesen, K., Bunjes, H. & Koch, M. H. Physicochemical characterization of 36. Auffan, M. et al. Towards a definition of inorganic nanoparticles from an
lipid nanoparticles and evaluation of their drug loading capacity and environmental, health and safety perspective. Nat. Nanotechnol. https://doi.
sustained release potential. J. Control. Release 48, 223–236 (1997). org/10.1038/nnano.2009.242 (2009).
9. Reker, D. et al. ‘Inactive’ ingredients in oral medications. Sci. Transl. Med. 11, 37. Lin, A. et al. Glycyrrhizin surface-modified chitosan nanoparticles for
eaau6753 (2019). hepatocyte-targeted delivery. Int. J. Pharm. 359, 247–253 (2008).
10. McLaughlin, C. K. et al. Stable colloidal drug aggregates catch and release 38. Tward, A. D. et al. Distinct pathways of genomic progression to benign and
active enzymes. ACS Chem. Biol. 11, 992–1000 (2016). malignant tumors of the liver. Proc. Natl Acad. Sci. USA 104,
11. Shamay, Y. et al. Quantitative self-assembly prediction yields targeted 14771–14776 (2007).
nanomedicines. Nat. Mater. 17, 361–368 (2018). 39. Bogorad, R. L. et al. Nanoparticle-formulated siRNA targeting integrins inhibits
12. Inactive Ingredient Search for Approved Drug Products (FDA, 2016); hepatocellular carcinoma progression in mice. Nat. Commun. 5, 3869 (2014).
https://www.accessdata.fda.gov/scripts/cder/iig/ 40. Lee, J. et al. Tumor stem cells derived from glioblastomas cultured in bFGF
13. Feng, B. Y., Shelat, A., Dorman, T. N., Guy, R. K. & Shoichet, B. K. and EGF more closely mirror the phenotype and genotype of primary tumors
High-throughput assays for promiscuous inhibitors. Nat. Chem. Biol. 1, than do serum-cultured cell lines. Cancer Cell 9, 391–403 (2006).
146–148 (2005). 41. Sharpless, N. E. & DePinho, R. A. The mighty mouse: genetically engineered
14. SCOGS (Select Committee on GRAS Substances) (FDA, 2016); https://www. mouse models in cancer drug development. Nat. Rev. Drug Discov. 5,
accessdata.fda.gov/scripts/fdcc/?set=SCOGS 741–754 (2006).
15. Wishart, D. S. et al. DrugBank 5.0: a major update to the DrugBank database 42. Waidely, E., Al-Yuobi, A. R. O., Bashammakh, A. S., El-Shahawi, M. S. &
for 2018. Nucleic Acids Res. 46, D1074–D1082 (2018). Leblanc, R. M. Serum protein biomarkers relevant to hepatocellular
16. Reker, D. et al. Machine learning uncovers food- and excipient-drug carcinoma and their detection. Analyst 141, 36–44 (2016).
interactions. Cell Rep. 30, 3710–3716.e4 (2020). 43. Lee, C. H. et al. Protective mechanism of glycyrrhizin on acute liver
17. Reker, D., Schneider, P. & Schneider, G. Multi-objective active machine injury induced by carbon tetrachloride in mice. Biol. Pharm. Bull. 30,
learning rapidly improves structure-activity models and reveals new 1898–1904 (2007).
protein-protein interaction inhibitors. Chem. Sci. 7, 3919–3927 (2016). 44. Gelderblom, H., Verweij, J., Nooter, K., Sparreboom, A. & Cremophor, E. L.
18. Gregori-Puigjane, E. & Mestres, J. A ligand-based approach to mining the The drawbacks and advantages of vehicle selection for drug formulation.
chemogenomic space of drugs. Comb. Chem. High T. Scr. 11, 669–676 (2008). Eur. J. Cancer 37, 1590–1598 (2001).
19. Wildman, S. A. & Crippen, G. M. Prediction of physicochemical parameters 45. Singh, A., Iyer, A. K. & Amiji, M. M. in Handbook of Nanobiomedical
by atomic contributions. J. Chem. Inf. Comp. Sci. 39, 868–873 (1999). Research (ed. Torchilin, V.) 199–233 (World Scientific Publishing Company,
20. Chuang, K. V. & Keiser, M. J. Adversarial controls for scientific machine 2014); https://doi.org/10.1142/9789814520652_0006
learning. ACS Chem. Biol. 13, 2819–2821 (2018). 46. Pohjala, L., Tammela, P., Pohjala, L. & Tammela, P. Aggregating behavior of
21. Test no. 318: dispersion stability of nanomaterials in simulated environmental phenolic compounds—a source of false bioassay results? Molecules 17,
media. OECD Guidelines for the Testing of Chemicals, Section 3 https://doi.org 10774–10790 (2012).
/10.1787/9789264284142-en (2017). 47. Traverso, G. & Langer, R. Perspective: special delivery for the gut. Nature 519,
22. Lipner, S. R. & Scher, R. K. Onychomycosis: treatment and prevention of S19 (2015).
recurrence. J. Am. Acad. Dermatol. 80, 853–867 (2019). 48. Cheng, C. J. & Saltzman, W. M. Nanomedicine: downsizing tumour
23. McClellan, K. J., Wiseman, L. R. & Markham, A. Terbinafine. Drugs 58, therapeutics. Nat. Nanotechnol. 7, 346–347 (2012).
179–202 (1999).
Publisher’s note Springer Nature remains neutral with regard to jurisdictional claims in
24. Matteucci, M. E., Hotze, M. A., Johnston, K. P. & Williams, R. O. Drug
published maps and institutional affiliations.
nanoparticles by antisolvent precipitation: mixing energy versus surfactant
stabilization. Langmuir 22, 8951–8959 (2006). © The Author(s), under exclusive licence to Springer Nature Limited 2021
Nature Nanotechnology | VOL 16 | June 2021 | 725–733 | www.nature.com/naturenanotechnology 733
Articles NaTure NanOTecHnOlOgy
Methods Dispersion kinetics. The dispersion stability of nanoparticles was performed
High-throughput formulation assessment. Stock solutions (10 mM) of aggregating according to established protocols in the OECD guidelines ‘Dispersion Stability
drugs and excipients were created in sterile DMSO and stored at −20 °C. For every of Nanomaterials in Simulated Environmental Media’ (Supplementary Fig. 5)21.
experiment, 1 μl drug stock solution was mixed with 1 μl stock solution of any of the Specifically, dispersion was studied at 250 μM drug concentration, except for
excipients (1:1) in a 96-well plate using a Tecan Freedom Evo 150 liquid-handling altered concentrations for celecoxib (500 μM) or nelfinavir (50 μM) to enable
deck. Mixing of the two droplets was ensured through centrifugation. Subsequently, studying dynamics at the same time scales compared with other drugs in spite of
we rapidly added 198 μl sterile-filtered and degassed phosphate-buffered saline (PBS) slower/faster aggregation dynamics and therefore sedimentation rate. Formulations
for solvent exchange and mixed the formulation through repeated pipetting. A 75 μl were generated by mixing 5 μl drug stock solution with 5 μl equimolar excipient
volume of replicate samples were subsequently transferred into a 384-well plate stock in DMSO or 5 μl DMSO followed by solvent exchange by adding 990 μl sterile
for high-throughput DLS assessment on a Wyatt Dyna Pro Plate Reader at 25 °C filtered and degassed PBS. All samples were generated in 4 ml glass vials, briefly
using five independent acquisitions of 5 s duration. DLS enabled us to quantitatively vortexed to ensure dispersion and subsequently stored sealed at room temperature.
assess nanoparticle formation by measuring the size of resulting co-aggregates Formulations were then sampled at predetermined time points by extracting 5 μl
with help of the ‘globular protein’ model. Data was processed by calculating the of formulation with a standard Eppendorf pipette from the centre of the vial. The
median size observed for a specific drug. We required at least a 50% size reduction extracted 5 μl samples were transferred into individual high-performance liquid
of the co-aggregate compared with drug alone to indicate nanoparticle formation. chromatography (HPLC) sample vials (Sigma-Aldrich) and diluted in acetonitrile
Our analysis suggested that this threshold could potentially enable an inclusive (for atovaquone and danazol) or methanol (for celecoxib, sorafenib, terbinafine and
separation of what appeared to be a bimodal distribution of aggregate sizes across nelfinavir) to ensure full solubility of the drug before injection onto the column.
our screen (Supplementary Fig. 2). Measures of dispersity and replicate variance were Diluted samples were stored at 4 °C and drug concentrations were determined via
considered but did not lead to improved predictive performance. We noted that drug liquid chromatography within 24 h as described in the Supplementary Methods.
self-aggregates would result in a large number of flagged DLS acquisitions, indicating
unreliable readouts through macro-aggregates and precipitation, while no such C. albicans XTT assay and microscopy. C. albicans were incubated in sterile
artefacts were observed for our nanoparticles. 50 g l−1 Difco YPD broth overnight at 30 °C on an orbital shaker at 300 r.p.m.
Centrifugation at 3,220 g for 5 min was used to extract the fungus. Washing
Machine learning. Chemical structures for all drugs in simplified molecular-input was performed twice with PBS. The final pellets were resuspended in 20 ml
line-entry system (SMILES) representation were extracted from DrugBank RPMI1640 (Sigma-Aldrich). The fungi concentration was determined using a
5.015. Data for excipients was extracted from the FDA according to previously haemocytometer with bright-field microscopy at ×40 magnification. Fungi were
published protocols9. Compounds were described according to radial chemical seeded at a concentration of 1 million per well in 96-well plates. Terbinafine–
substructures (Morgan Fingerprint, radius 4, 2,048 bits, rdkit.org) and calculated taurocholic acid particles, free terbinafine or taurocholic acid excipient control
physicochemical properties (rdkit.Chem.Descriptors._descList, rdkit.org) based on were added at concentrations of 250 μM, 25 μM and 2.5 μM, respectively. PBS
previously published evaluations16,17. Concatenating the substructure description containing 1% DMSO was used as a buffer control, and 70% isopropanol was used
and the physicochemical properties for every drug and every excipient generated as a positive treatment control. Plates were wrapped with Parafilm and incubated at
a 4,496-dimensional description of a drug–excipient formulation. In addition, 37 °C. Fungus viability was evaluated using an XTT assay after 24 h of incubation.
short MD simulations were run and automatically analysed to assess the enthalpic, To this end, XTT was prepared as a saturated solution at 0.5 g l−1 in sterile PBS
non-covalent interaction potential between drugs and excipients. In brief, under light protection and subsequently sterile filtered with a 0.22 μm pore size
atomic partial charges for drugs and excipients were derived from antechamber filter. XTT solution was aliquoted in 10 ml Falcon tubes and stored at −80 °C.
and parmchk2, and the net charge was calculated using the OpenEye Quacpac Before a measurement, 1 μl of a 10 mM menadione solution in acetone was added
AM1-BCC method. Two excipients and two drug molecules were randomly to the XTT solution and used to substitute the media. Absorbance was measured
positioned using packmol (m3g.iqm.unicamp.br/packmol/) and Amber’s tleap at 490 nm to determine background signal per well. Plates were subsequently
module. After energy minimization of the system, short 20 ns simulations were incubated for another 2 h at 37 °C under light protection and absorbance was
run in OpenMM 7.2.1 (openmm.org) in OBC2 implicit solvent with non-periodic measured at 490 nm to determine fungus viability. Treatment data were normalized
boundary conditions and no cut-off distance. A Langevin integrator was used to the untreated control (100% survival, 1% DMSO in PBS), and positive treatment
at 300 K with a friction coefficient of 1 ps−1. The timestep of the simulation (70% ethanol) was used to ensure experimental consistency. For microscopy, ×40
was 2 fs and the trajectory was saved every 10 ps, creating 2,000 frames. These bright-field images were taken after 17 h incubation using 25 μM free terbinafine,
trajectories were processed with MDTraj (mdtraj.org) to calculate heavy atom 25 μM terbinafine–taurocholic acid nanoparticles or 1% DMSO PBS buffer control
distances between drugs and excipients and derive summary statistics (maximum, at 37 °C.
minimum and average distance, as well as maximum first derivative) for each
pair. Furthermore, the potential and kinetic energies of the conformation in Skin uptake of terbinafine particles. All ex vivo studies were approved by the
the last frame were calculated. Overall, this gave us an additional 19 parameters Massachusetts Institute of Technology Committee on Animal Care. Fresh porcine
to characterize drug and excipient pairs as input to the machine learning ear samples were provided by the Massachusetts Institute of Technology facilities
platform. These 4,515-dimensional numerical characterizations of a formulation and were washed three times with PBS and mounted on a Franz diffusion cell
served as input for the random forest classification machine learning model (FDC-400 flat flange, 15 mm orifice diameter, mounted on an FDC diffusion drive
(scikit-learn) with 500 trees and using ⌊√4,515⌋ = 67 features per classification console providing synchronous stirring at 350 r.p.m., Crown Glass) by gluing the
tree. This model was compared with naive Bayes (GaussianNB), nearest epidermis side of the skin to the donor chamber and subsequent mounting onto
neighbour (KNeighborsClassifier; k = 3), decision trees (DecisionTreeClassifier), the receiver chamber that was preloaded with PBS. Terbinafine–taurocholic acid
neural networks (MLPClassifier) and a support-vector machine (LinearSVC) nanoparticles or free terbinafine were added at 250 μM in 1% DMSO PBS and
implemented with default parameters in scikit-learn. To analyse the correlation loaded to the donor chambers in triplicates. PBS containing 1% DMSO served as
between training dataset size and model performance, we trained our random the buffer control. Parafilm was used to prevent evaporation from both the receiver
forest model on randomly selected subsets of the data and evaluated out-of-bag and the donor chamber. After 4 h of incubation, donor solutions were removed and
predictive performance as a measure of model convergence. This analysis was the skin was washed with PBS to remove excess drug. The perfusion area was cut
run 20 times and mean performance was reported. Code and data for all these into squares and weighed and measured for further analysis. Skin samples were
calculations can be found at https://github.com/DanReker/CoAggregators. loaded into 2 ml homogenizing tubes (Fisher Scientific, Fisherbrand Pre-Filled
Bead Mill Tubes) with methanol at a 1:2 ratio and homogenized at 6,000 r.p.m.
Additional MD simulations. For the six novel combinations of drugs and for 40 s three times. The homogenate was analysed for drug content using
excipients, we converted SMILES compound representations to Tripos mol2 ultra-performance liquid chromatography-electrospray tandem mass spectrometry
files using Openbabel with B3LYP/6-31 G* partial charge calculation with (UPLC-ESI-MS) as described in the Supplementary Methods.
general AMBER force field (GAFF) and systematic rotor search for generating
three-dimensional (3D) conformations. If a systematic confirmation search was HUH7 cell survival assessment. HUH7 cells were gifted by J. Horton (UT
rate limiting, the process automatically switched to a weighted search. Missing Southwestern Medical Center). Cells were not authenticated. Cells were tested
parameters were checked with the parmchk2 module in Ambertools. Using negative for mycoplasma contamination by the diagnostic laboratory of the
packmol, five random system configurations were generated for 20 molecules of Division of Comparative Medicine at MIT. Cells were plated at 10,000 cells in
each pair (20 + 20 = 40 molecules total), or 20 molecules of drug only. A topology 96-well plates and incubated overnight to allow adhesion. The cell medium was
and coordinate file were generated with the tleap module in Ambertools. OpenMM changed and cells were treated with various concentrations of nanoparticles for
7.3.1 was used to create a 20 ns simulation under OBC2 implicit solvent at 1 bar, 48 h. These concentration series were generated by creating a dilution series of the
300 K, with a periodic cut-off distance of 1 nm after initial minimization. The last drug stock solutions and then performing nanoparticle generation at altered stock
frame of this simulation was visualized in PyMol using coloured van der Waals concentrations. Cell viability was measured through quantitation of ATP using
spheres. Molecular interactions for the last frame were determined using the CellTiter-Glo (Promega).
MolBridge webserver (nucleix.mbu.iisc.ernet.in/molbridge) as well as extracting
Baker-Hubbard hydrogen bonds between drugs and excipients through MDTraj Sorafenib uptake experiments. HUH7 cells were plated in 12-well plates at
(http://mdtraj.org/). 200,000 cells (1 ml DMEM medium) and incubated for 24 h to allow for adhesion.
Nature Nanotechnology | www.nature.com/naturenanotechnology
NaTure NanOTecHnOlOgy Articles
Cell medium (900 µl) was changed and cells were treated with (100 µl ×10) 100 µM humanely euthanized at 30 min, 2 h, 4 h, 6 h and 24 h after administration to
sorafenib, 100 µM of nanoparticle formulations or buffer control (0.1% DMSO process organs and blood. For sample preparation, 5% BSA in PBS buffer was
PBS) and incubated for 2 h. Afterwards the supernatant was removed and cells added at a 2:1 volume-to-mass ratio. Samples were homogenized at 6,500 r.p.m.
were carefully washed three times using 2.5% Tween-80 in PBS, which we had twice for 2 min at room temperature. A 100 µl volume of each homogenate was
tested to ensure it dislodged sorafenib aggregates while not changing cell adhesion spiked with 50 µl of 5 µg ml−1 internal standard in acetonitrile. Ethyl acetate
or morphology according to bright-field microscopy images. Cells were lysed (1 ml) was also added to homogenized samples for extraction. Samples were
with Pierce RIPA Buffer (ThermoFisher Scientific) and transferred. Subsequently, vortexed, sonicated for 10 min and centrifuged for 5 min at 6,000 r.p.m. Following
lysate was lyophilized and re-dissolved in methanol (200 µl). The solution was centrifugation, the collected supernatant was allowed to evaporate. The evaporated
centrifuged (10 min at 3,200 r.p.m.) and the supernatant was subsequently samples were reconstituted with 300 µl acetonitrile and centrifuged for 5 min at
analysed using HPLC for sorafenib content as described in the Supplementary 6,000 r.p.m. A 200 µl volume of the supernatant was pipetted into a 96-well plate
Methods. Area under the curve (AUC) values were converted into sorafenib containing 200 µl water. Finally, 0.50 µl was injected onto the UPLC-ESI-MS system
content (µg ml−1) according to a standard curve and normalized according for the analysis of sorafenib content. AUCs for each organ were calculated using
to protein content per replicate (mg ml−1) from an orthogonal bicinchoninic numerical integration following the trapezoidal rule.
acid assay (BCA). To study the mechanism of increased uptake of sorafenib–
glycyrrhizin particles, we performed another uptake experiment according to the Reporting Summary. Further information on research design is available in the
protocol above, but preincubated the cells for 30 min with sucrose (0.15 g ml−1) or Nature Research Reporting Summary linked to this article.
methyl-beta-cyclodextrin (5 mM) to inhibit endocytosis.
Data availability
Drug loading and encapsulation efficiency. Particles were generated using stock All data used in this study were extracted from publicly available sources from the
concentrations of 10 mM for both drugs and excipients. Particles were subsequently DrugBank website (version 5.0, drugbank.ca), the FDA (GRAS version June 2016
washed using two rounds of centrifugation, removal of supernatant and and IIG version 0716 UNII 362O9ITL9D datasets, www.fda.gov) and the Shoichet
redispersion in PBS. Particles were then dissolved in fixed volumes of methanol laboratory (bkslab.org/takeaways/aggregator_hts). The processed and curated data
to ensure full solubility. These solutions were subsequently submitted to liquid are made available through the GitHub repository at https://github.com/DanReker/
chromatography analysis to determine the concentration of drug and excipient in CoAggregators.
these solutions. The amount of drug or excipient in the particles was calculated
by subtracting the expected amount (micrograms of drug/excipient assuming
full solubility in PBS) from the actually measured concentrations. Encapsulation Code availability
efficiency was determined as the amount of drug found in the particles (in ug) All code for this study to perform simulations and machine learning is available
divided by the amount of drug added via the stock solution in particle production through the GitHub repository at https://github.com/DanReker/CoAggregators.
(equation (1)).
Drug in particle Acknowledgements
Encapsulation = (1) D.R. is a Swiss National Science Foundation Fellow (grants P2EZP3_168827 and
Added drug P300P2_177833). Y.R. is grateful to the MIT Skoltech Initiative for financial support.
A.R.K. is grateful to the PhRMA foundation postdoctoral fellowship for financial
Drug loading was calculated as the amount of drug in the particles (in ug) support. We thank the Koch Institute Swanson Biotechnology Center for technical
divided by the mass of the particles given by the cumulative amount of the drug (in support, specifically the High Throughput Sciences Facility, Peterson (1957)
ug) and the amount of excipient (in ug) in the particles (equation (2)). Nanotechnology Materials Core Facility, the Animal Imaging and Preclinical Testing
Drug in particle core, and the Hope Babette Tang (1983) Histology Facility. This work was supported in
Loading = (2) part by the Koch Institute Support (core) grant P30-CA14051 from the National Cancer
Drug in particle + Excipient in particle
Institute and by the NIH grant EB000244. We are grateful to OpenEye for providing
us with an OpenEye Academic License. We are grateful to H. Mazdiyasni for technical
support and to M. Jimenez for providing access to C. albicans and helpful discussions
In vivo cancer study. All in vivo studies were approved by the Massachusetts
throughout the study.
Institute of Technology Committee on Animal Care. Female FVB/N mice were
purchased from Charles River Laboratories. Animals were maintained in a
conventional barrier facility with a climate-controlled environment on a 12 h Author contributions
light/12 h dark cycle, fed ad libitum with regular rodent chow. HCC was induced D.R., R.L. and G.T. conceived the study. D.R., Y.R., A.R.K., R.L. and G.T. designed
as previously described38,39. Briefly, plasmids encoding human ΔN90-β-catenin, experiments. D.R. and J.W.Y. performed in silico experiments. D.R., R.C., J.W.Y., N.N.,
human MET and SB transposase were hydrodynamically injected intravenously R.M.Z., T.E. and J.L. performed in vitro experiments. D.R., R.C. and A.G. performed
into six-to-seven-week-old mice. Plasmids were kindly provided by X. Chen in vivo experiments. Y.R., A.R.K., T.v.E., A.L.-J., C.K.S. and J.H.C. supported in vitro
(UCSF). Plasmids were amplified and isolated in endotoxin-free conditions (<5 EU experiments. Y.R., A.R.K., E.M.S., D.L., J.C., S.M.T., K.I., P.C. and A.M.H. supported
mg−1) by Aldevron. Five weeks after injections, serum levels of AFP were analysed in vivo experiments. D.Y. performed TEM imaging, and K.H., A.L. and J.R. performed
as the HCC marker, and animals were randomized according to AFP levels into the pharmaceutical analytics. D.R., R.L. and G.T. wrote the manuscript with contributions
different treatment groups. Treatment was started six weeks after HCC induction, from the other authors. All authors approved the final version of this manuscript.
and each group of mice was treated three times a week (t.i.w.) for four weeks with
one of the following treatments: intravenous injections of 30 mg kg−1 sorafenib in
sorafenib–glycyrrhizin nanoparticles, sorafenib suspensions at 30 mg kg−1 in PBS Competing interests
with 1% DMSO delivered by oral gavage, intravenous injections of buffer control D.R., Y.R., A.R.K., R.C., J.W.Y., N.N., A.G., R.M.Z., R.L. and G.T. are co-inventors on
(1% DMSO in PBS), intravenous injections of 30 mg kg−1 sorafenib solubilized in multiple patent applications describing novel nanoformulation systems and interactions
a 50:50 ethanol-cremophor mixture or intravenous injections of glycyrrhizin in between excipients and drugs. D.R. acts as a mentor for the German Accelerator Life
1% DMSO in PBS (vehicle control). Mice were evaluated twice daily for tumour Sciences and acts as a scientific consultant for pharmaceutical and biotechnology
burden (>15% increase in body weight) and other clinical signs of discomfort companies.
such as laboured breathing, lethargy, lack of appetite, cachexia, diarrhoea, poor
grooming, hunched appearance and lack of nest building. After the four-week
treatment period, AFP levels and body weight changes were recorded to evaluate Additional information
treatment success. Treatment was stopped and mice were evaluated twice daily for Supplementary information The online version contains supplementary material
progression-free survival according to the same signs of adverse effects. available at https://doi.org/10.1038/s41565-021-00870-y.
Correspondence and requests for materials should be addressed to G.T.
Biodistribution of sorafenib formulations. Healthy, ten-week-old, female
Peer review information Nature Nanotechnology thanks Michael Keiser, Jie Zheng and
FVB/N mice were injected with a single dose of 30 mg kg−1 sorafenib–glycyrrhizin
the other, anonymous, reviewer(s) for their contribution to the peer review of this work.
nanoparticles or 30 mg kg−1 sorafenib dissolved in cremophor–ethanol, or received
a suspension of 30 mg kg−1 sorafenib in PBS orally. Three mice per group were Reprints and permissions information is available at www.nature.com/reprints.
Nature Nanotechnology | www.nature.com/naturenanotechnology
You might also like
- Hide Tanning PDF - FINAL7.23Document32 pagesHide Tanning PDF - FINAL7.23Kevin100% (1)
- SQL Queries Interview Questions and Answers - Query ExamplesDocument25 pagesSQL Queries Interview Questions and Answers - Query Examplesiveraj67% (9)
- PESTEL Analysis of MoroccoDocument2 pagesPESTEL Analysis of Moroccoethernalx67% (15)
- Reverse PharmacolgoyDocument55 pagesReverse Pharmacolgoyعبدالله الجزارNo ratings yet
- Drug Target Interaction (DTI) and Prediction Using Machine LearningDocument9 pagesDrug Target Interaction (DTI) and Prediction Using Machine LearningIJRASETPublicationsNo ratings yet
- LymphomaDocument20 pagesLymphomaChairul Adilla Ardy100% (1)
- Sky & Telescope - February 2016 (Gnv64)Document82 pagesSky & Telescope - February 2016 (Gnv64)bogarguz100% (1)
- Pharmacology in Drug Discovery: Understanding Drug ResponseFrom EverandPharmacology in Drug Discovery: Understanding Drug ResponseNo ratings yet
- Applied Statistics in Business and Economics 5th Edition Doane Solutions ManualDocument26 pagesApplied Statistics in Business and Economics 5th Edition Doane Solutions ManualSharonMartinezfdzp100% (44)
- Bombardier Zefiro Technical Description enDocument15 pagesBombardier Zefiro Technical Description ennickerlesstezla100% (1)
- 06 - Chapter 1Document37 pages06 - Chapter 1Vikash KushwahaNo ratings yet
- Scoring para Predecir SinergismoDocument12 pagesScoring para Predecir SinergismoLaura GarciaNo ratings yet
- Mining Significant Substructure Pairs For Interpreting Polypharmacology in Drug-Target NetworkDocument10 pagesMining Significant Substructure Pairs For Interpreting Polypharmacology in Drug-Target NetworkPhạm Ngọc KhánhNo ratings yet
- New Methods For Drug Synergy PredictionDocument20 pagesNew Methods For Drug Synergy Predictionadelk138019No ratings yet
- Linking Drug Target and Pathway Activation For Effective Therapy Using Multi-Task LearningDocument10 pagesLinking Drug Target and Pathway Activation For Effective Therapy Using Multi-Task LearningBikash Ranjan SamalNo ratings yet
- s12859 017 1638 4 PDFDocument10 pagess12859 017 1638 4 PDFfkamaliyahNo ratings yet
- Structure-Based Pharmacophore Models Generation and Combinatorial Screening of ICE InhibitorsDocument4 pagesStructure-Based Pharmacophore Models Generation and Combinatorial Screening of ICE InhibitorsRaju DasNo ratings yet
- Iskar Et Al (2010)Document8 pagesIskar Et Al (2010)mei mulyaNo ratings yet
- Articulo InteresanteDocument10 pagesArticulo InteresanteMayra Niebles BolivarNo ratings yet
- On The Integration of in Silico Drug Design Methods For Drug RepurposingDocument7 pagesOn The Integration of in Silico Drug Design Methods For Drug RepurposingdarmaNo ratings yet
- Techniques: Application of Systems Biology To Absorption, Distribution, Metabolism, Excretion and ToxicityDocument8 pagesTechniques: Application of Systems Biology To Absorption, Distribution, Metabolism, Excretion and Toxicityppt4056No ratings yet
- Drug Discovery Paper m1Document6 pagesDrug Discovery Paper m1Aditi ShimpiNo ratings yet
- Drug Like PropertiesDocument4 pagesDrug Like PropertiesLe MaNo ratings yet
- AS A F C D S P D L: Ystematic Pproach To Eaturization For Ancer RUG Ensitivity Redictions With EEP EarningDocument16 pagesAS A F C D S P D L: Ystematic Pproach To Eaturization For Ancer RUG Ensitivity Redictions With EEP EarningAustin ClydeNo ratings yet
- On The Integration of in Silico Drug Design Methods For Drug RepurposingDocument7 pagesOn The Integration of in Silico Drug Design Methods For Drug Repurposingnathasya shasykiranaNo ratings yet
- Modeling and Simulation of Drug Release Through Polymer MatricesDocument3 pagesModeling and Simulation of Drug Release Through Polymer MatricesSerotonin سيروتونينNo ratings yet
- Drug Target Interaction (DTI) and Prediction Using Machine LearningDocument9 pagesDrug Target Interaction (DTI) and Prediction Using Machine LearningIJRASETPublicationsNo ratings yet
- Biology Project On Ai in MedicineDocument10 pagesBiology Project On Ai in Medicinejapmansingh45678No ratings yet
- Paper v14 FiguresDocument46 pagesPaper v14 Figuresspanishbear75No ratings yet
- In Silico Pharmacology For Drug Discovery: Applications To Targets and BeyondDocument17 pagesIn Silico Pharmacology For Drug Discovery: Applications To Targets and BeyondAw Yong Yi XiangNo ratings yet
- Perspective: Unnati (2019) - Techniques Used in Metabolite Profiling of BryophytesDocument9 pagesPerspective: Unnati (2019) - Techniques Used in Metabolite Profiling of BryophytesAnn AlcalaNo ratings yet
- Prediction of Drug-Target Interactions and Drug Repositioning Via Network-Based InferenceDocument12 pagesPrediction of Drug-Target Interactions and Drug Repositioning Via Network-Based Inferencesamuel chenNo ratings yet
- 1398857738Document11 pages1398857738Marisa dra anggraNo ratings yet
- Novel Hybrid Ultrafast Shape Descriptor Method For Use in Virtual ScreeningDocument10 pagesNovel Hybrid Ultrafast Shape Descriptor Method For Use in Virtual Screeningsatish kumarNo ratings yet
- Molecules: Challenges, Applications, and Recent Advances of Protein-Ligand Docking in Structure-Based Drug DesignDocument27 pagesMolecules: Challenges, Applications, and Recent Advances of Protein-Ligand Docking in Structure-Based Drug DesignMukul ShuklaNo ratings yet
- Kahlous 2017Document17 pagesKahlous 2017wadelkrid1270No ratings yet
- Journal of Biomolecular ScreeningDocument6 pagesJournal of Biomolecular ScreeningtaymooooNo ratings yet
- Development and Charecterization of PLGA-nanoparticles Containing CarvedilolDocument6 pagesDevelopment and Charecterization of PLGA-nanoparticles Containing CarvedilolSetti MlvNo ratings yet
- Ghose 1999Document18 pagesGhose 1999taoufik akabliNo ratings yet
- In Silico Pharmacology For Drug Discovery: Methods For Virtual Ligand Screening and ProfilingDocument12 pagesIn Silico Pharmacology For Drug Discovery: Methods For Virtual Ligand Screening and ProfilingDwi PuspitaNo ratings yet
- Drug Designing 1Document2 pagesDrug Designing 1ShreyaChakladarNo ratings yet
- Drug 3Document6 pagesDrug 3Salem Optimus Technocrates India Private LimitedNo ratings yet
- Seye 3optimization of The Anticonvulsant Activity of 2-Acetamido-N-Benzyl-2 - (5 - Methylfuran-2-Yl) Acetamide Using QSAR Modeling and Molecular Docking TechniquesDocument19 pagesSeye 3optimization of The Anticonvulsant Activity of 2-Acetamido-N-Benzyl-2 - (5 - Methylfuran-2-Yl) Acetamide Using QSAR Modeling and Molecular Docking TechniquesdavidNo ratings yet
- Design, Formulation, In-Vitro and Ex-Vivo Evaluation of Atazanavir Loaded Cubosomal GelDocument18 pagesDesign, Formulation, In-Vitro and Ex-Vivo Evaluation of Atazanavir Loaded Cubosomal GelAnand ChettupalliNo ratings yet
- Tutorial 1Document3 pagesTutorial 1Xiaojun YanNo ratings yet
- Updated Version: Mol Cancer TherDocument13 pagesUpdated Version: Mol Cancer TherSakshi IssarNo ratings yet
- Computational Methods For Prediction of Drug LikenessDocument10 pagesComputational Methods For Prediction of Drug LikenesssciencystuffNo ratings yet
- High-Throughput Approaches To Uncover SynergisticDocument12 pagesHigh-Throughput Approaches To Uncover SynergisticRodrigo MaxNo ratings yet
- Mass Spectrometry Based Metabolomics A Guide For Annotation, Quantification and Best ReportingDocument10 pagesMass Spectrometry Based Metabolomics A Guide For Annotation, Quantification and Best ReportingsridharNo ratings yet
- Kannan Drugdesign PTDocument16 pagesKannan Drugdesign PTKannan Kathuria100% (1)
- Shahsavari Et Al, 2017Document7 pagesShahsavari Et Al, 2017Ramu RacikNo ratings yet
- PharmaDocument18 pagesPharmagombossandorNo ratings yet
- 2016 Bioinformatics 32 579-586Document8 pages2016 Bioinformatics 32 579-586mbrylinskiNo ratings yet
- Articulo de ApoyoDocument9 pagesArticulo de ApoyoAlejandroNo ratings yet
- Evidence-Based Absorption, Distribution, Metabolism, Excretion (ADME) and Its Interplay With Alternative Toxicity MethodsDocument16 pagesEvidence-Based Absorption, Distribution, Metabolism, Excretion (ADME) and Its Interplay With Alternative Toxicity MethodsAyi Yurike Tri YantiNo ratings yet
- BBRA MeenaDocument15 pagesBBRA MeenaVenkatNo ratings yet
- Full Papers: Santosh Aryal, Che-Ming Jack Hu, and Liangfang ZhangDocument7 pagesFull Papers: Santosh Aryal, Che-Ming Jack Hu, and Liangfang ZhangKamran JalilNo ratings yet
- Deep Learning Based Drug Metabolites PredictionDocument11 pagesDeep Learning Based Drug Metabolites PredictionMony MontelongoNo ratings yet
- The Impact of Natural Products Upon Modern Drug DiscoveryDocument16 pagesThe Impact of Natural Products Upon Modern Drug Discoverytuti ratnasariNo ratings yet
- Riviere Et Al-2014-Pharmaceutical StatisticsDocument11 pagesRiviere Et Al-2014-Pharmaceutical StatisticsCristina CNo ratings yet
- Role of Computer-Aided Drug Design in Modern Drug DiscoveryDocument16 pagesRole of Computer-Aided Drug Design in Modern Drug DiscoverySourav MajumdarNo ratings yet
- Review 1-5 PDFDocument5 pagesReview 1-5 PDFEditor IjprtNo ratings yet
- Natural Products Analysis: Instrumentation, Methods, and ApplicationsFrom EverandNatural Products Analysis: Instrumentation, Methods, and ApplicationsVladimir HavlicekNo ratings yet
- Ghose 1999Document14 pagesGhose 1999taoufik akabliNo ratings yet
- About InhibitorsDocument13 pagesAbout Inhibitorssumera120488No ratings yet
- Prediction of Genotoxic Potential of Cosmetic IngredientsDocument22 pagesPrediction of Genotoxic Potential of Cosmetic IngredientslordstaniusNo ratings yet
- Preclinical Drug Discovery and Development: David S. DuchDocument26 pagesPreclinical Drug Discovery and Development: David S. DuchAkanksha PatelNo ratings yet
- Supplementary DataDocument24 pagesSupplementary DataHe ZeeNo ratings yet
- Liu - Review of The Fundamental Theories Behind Small Angle X-Ray ScatteringDocument22 pagesLiu - Review of The Fundamental Theories Behind Small Angle X-Ray ScatteringHe ZeeNo ratings yet
- Postermall Grå A0Document1 pagePostermall Grå A0He ZeeNo ratings yet
- 2020 - Bacterial Lipase Triggers The Release of Antibiotics From Digestible LiquidDocument15 pages2020 - Bacterial Lipase Triggers The Release of Antibiotics From Digestible LiquidHe ZeeNo ratings yet
- 2013 - Hinton Et Al - Bicontinuous Cubic Phase Nanoparticle Lipid Chemistry Affects Toxicity inDocument13 pages2013 - Hinton Et Al - Bicontinuous Cubic Phase Nanoparticle Lipid Chemistry Affects Toxicity inHe ZeeNo ratings yet
- 2006 - Dong Et Al - Bulk and Dispersed Aqueous Phase Behavior of PhytantriolDocument7 pages2006 - Dong Et Al - Bulk and Dispersed Aqueous Phase Behavior of PhytantriolHe ZeeNo ratings yet
- 2011 - Tri-Hung Nguyen Et Al - Nanostructured Reverse Hexagonal Liquid Crystals Sustain Plasma ConcentraDocument10 pages2011 - Tri-Hung Nguyen Et Al - Nanostructured Reverse Hexagonal Liquid Crystals Sustain Plasma ConcentraHe ZeeNo ratings yet
- User Defined FunctionsDocument67 pagesUser Defined Functionsmohamed aliNo ratings yet
- Lesson 2 - Língua Inglesa 7Document21 pagesLesson 2 - Língua Inglesa 7Shara Maria Venâncio SilvaNo ratings yet
- Explanation Teks: How To Keep The Body HealthyDocument4 pagesExplanation Teks: How To Keep The Body HealthyremybonjarNo ratings yet
- Geologic Report Arches NationalDocument9 pagesGeologic Report Arches NationalJacob AndersonNo ratings yet
- 4 Structure PDFDocument45 pages4 Structure PDFAnil SuryawanshiNo ratings yet
- Tripwire Is An Intrusion Detection SystemDocument28 pagesTripwire Is An Intrusion Detection SystempoornimaNo ratings yet
- Boss DD-6Document28 pagesBoss DD-6Justin Alexander SanzonENo ratings yet
- Purification of Wastewater by Metal Oxide NanoparticlesDocument12 pagesPurification of Wastewater by Metal Oxide NanoparticlesEditor IJTSRDNo ratings yet
- Lesson 1 Exploring Indian LiteratureDocument5 pagesLesson 1 Exploring Indian LiteratureAthan MensalvasNo ratings yet
- Srijana BahadurDocument13 pagesSrijana Bahadurkhadija khanNo ratings yet
- Formalismo Geométrico de La Mecánica Cuántica y Sus Aplicaciones A Modelos MolecularesDocument51 pagesFormalismo Geométrico de La Mecánica Cuántica y Sus Aplicaciones A Modelos Moleculareshugo_valles_2No ratings yet
- Introduction To Public Policy: Course DescriptionDocument15 pagesIntroduction To Public Policy: Course DescriptionJericko Perez AvilaNo ratings yet
- Cedarwood ChromatographyDocument6 pagesCedarwood ChromatographyMartinaNo ratings yet
- Literature Review of Centella AsiaticaDocument6 pagesLiterature Review of Centella Asiaticaea3vk50y100% (1)
- Antenna Mini ProjectDocument65 pagesAntenna Mini ProjectHassan MehsenNo ratings yet
- Laboratory Activity No 3Document11 pagesLaboratory Activity No 3MAE MALALUANNo ratings yet
- Abrar AwolDocument153 pagesAbrar AwolErmias Assaminew AlmazNo ratings yet
- Rasi Navamsa: As Mo Ke Su Ve Mo JuDocument11 pagesRasi Navamsa: As Mo Ke Su Ve Mo JuRavan SharmaNo ratings yet
- DBMS - Lab CAT2 Code SWE1001 SLOT L47+48 DATE 16/10/19Document2 pagesDBMS - Lab CAT2 Code SWE1001 SLOT L47+48 DATE 16/10/19msroshi madhuNo ratings yet
- Newyearbook PDFDocument165 pagesNewyearbook PDFAlberto CenniniNo ratings yet
- The Awakened Goat: Playable RaceDocument2 pagesThe Awakened Goat: Playable RacePJ FlandersNo ratings yet
- DLP L05 - Challenges in AdolescenceDocument3 pagesDLP L05 - Challenges in AdolescenceSora YamazakiNo ratings yet
- Recognition SpielDocument4 pagesRecognition SpielJoeyNo ratings yet