You might also like
- R E M Ind Er S:: UHC v.1 January 2020Document2 pagesR E M Ind Er S:: UHC v.1 January 2020Melody Frac ZapateroNo ratings yet
- PhilHealth Member Registration FormDocument2 pagesPhilHealth Member Registration FormAbraham JunioNo ratings yet
- PMRF 012020Document2 pagesPMRF 012020DLPS HSENo ratings yet
- Philhealth FormDocument2 pagesPhilhealth FormJordan CabreraNo ratings yet
- PhilHealth Member Registration FormDocument2 pagesPhilHealth Member Registration FormValerie LalinNo ratings yet
- PMRF - Final 2019Document2 pagesPMRF - Final 2019Silverghost Sun Dance Studio82% (17)
- PMRF RegistrationDocument2 pagesPMRF RegistrationArvin Dayag100% (2)
- Government FormsDocument5 pagesGovernment Formstrixie jealaine s. rosero100% (2)
- PhilHealth Member Registration FormDocument2 pagesPhilHealth Member Registration FormJenilyn Gonzales Narrido100% (2)
- Philhealth FormDocument2 pagesPhilhealth FormJaymart Ingreso100% (1)
- PhilHealth Member Registration FormDocument2 pagesPhilHealth Member Registration FormMyla Rose AcobaNo ratings yet
- PMRF 012020Document2 pagesPMRF 012020Mam BoyNo ratings yet
- Reminders:: UHC v.1 January 2020 Philhealth Identification Number (Pin)Document8 pagesReminders:: UHC v.1 January 2020 Philhealth Identification Number (Pin)YhelLappayNo ratings yet
- Reminders:: UHC v.1 January 2020 Philhealth Identification Number (Pin)Document3 pagesReminders:: UHC v.1 January 2020 Philhealth Identification Number (Pin)Jhepoy Lumanglas AstillaNo ratings yet
- PhilHealth Member Registration FormDocument3 pagesPhilHealth Member Registration FormHanzo GamingNo ratings yet
- Langcuyan Jonalyn Dacles: Please Carefully Read Instructions at The Back Before Accomplishing This FormDocument10 pagesLangcuyan Jonalyn Dacles: Please Carefully Read Instructions at The Back Before Accomplishing This FormPaHm Iglesias LeeNo ratings yet
- Pag-Ibig FormDocument1 pagePag-Ibig FormWellaine LorithyNo ratings yet
- Pagibig Loan Form v2020 With ESIG-Final PDFDocument2 pagesPagibig Loan Form v2020 With ESIG-Final PDFKeyserr VillaflorNo ratings yet
- Multi-Purpose Loan (MPL) Application Form: FilipinoDocument2 pagesMulti-Purpose Loan (MPL) Application Form: Filipinocamlon khajarNo ratings yet
- Philhealth Identification Number (Pin) Important Reminders:: PurposeDocument3 pagesPhilhealth Identification Number (Pin) Important Reminders:: PurposeMhelaril AnneNo ratings yet
- SLF066 Calamity Loan Application Form - V05Document2 pagesSLF066 Calamity Loan Application Form - V05Selyun E OnnajNo ratings yet
- PmrffsfsafDocument2 pagesPmrffsfsafManolito MacanasNo ratings yet
- Pag-IBIG Loyalty Card Plus ApplicationDocument2 pagesPag-IBIG Loyalty Card Plus ApplicationKillah BeatsNo ratings yet
- SLF065 MultiPurposeLoanApplicationForm V06Document2 pagesSLF065 MultiPurposeLoanApplicationForm V06izze veraniaNo ratings yet
- Reference No. CEF17202009-03240813202107185435Document7 pagesReference No. CEF17202009-03240813202107185435Marielle J GarciaNo ratings yet
- Fish R FormDocument1 pageFish R Formlibertygavarra1No ratings yet
- Reactivation Application Form 2Document4 pagesReactivation Application Form 2alina aguirre de la cruzNo ratings yet
- CFO Form PDFDocument2 pagesCFO Form PDFJego ElevadoNo ratings yet
- Pag-IBIG Loyalty Card FormDocument2 pagesPag-IBIG Loyalty Card FormJason Sylar100% (4)
- Calamity Loan Application Form: (E.g., JR., II) (For Married Women) (Check If Applicable Only)Document2 pagesCalamity Loan Application Form: (E.g., JR., II) (For Married Women) (Check If Applicable Only)Jaypee VegaNo ratings yet
- Pop MDFDocument2 pagesPop MDFCee Pee IIINo ratings yet
- Calamity Loan Application Form: (E.g., JR., II) (For Married Women) (Check If Applicable Only)Document2 pagesCalamity Loan Application Form: (E.g., JR., II) (For Married Women) (Check If Applicable Only)Chel MiNo ratings yet
- MPL loan application formDocument2 pagesMPL loan application formAndreRicamaraNo ratings yet
- SLF065 MultiPurposeLoanApplicationForm V06Document2 pagesSLF065 MultiPurposeLoanApplicationForm V06izze veraniaNo ratings yet
- SLF065 MultiPurposeLoanApplicationForm V04 Fillable FinalDocument2 pagesSLF065 MultiPurposeLoanApplicationForm V04 Fillable FinalBernellie Mae AranetaNo ratings yet
- Revised Membership FormDocument2 pagesRevised Membership FormJoan May DegojasNo ratings yet
- Loyalty Card Sample Format-SignedDocument2 pagesLoyalty Card Sample Format-SignedLoriene BuenafeNo ratings yet
- Pag-IBIG MPL Loan ApplicationDocument2 pagesPag-IBIG MPL Loan Applicationcliford caballeroNo ratings yet
- Philhealth - Pag-Ibig MibDocument8 pagesPhilhealth - Pag-Ibig MibChino PaciaNo ratings yet
- PFF108 LoyaltyCardPlusApplicationForm V06Document2 pagesPFF108 LoyaltyCardPlusApplicationForm V06Charlene borneoNo ratings yet
- Loyalty Card Plus: Application FormDocument2 pagesLoyalty Card Plus: Application FormRaisa GeleraNo ratings yet
- Afl Peaksun Enterprises and Export Corporation Pgaksun: 2F Peaksun Building 1505 Princeton St. Mandaluyong CityDocument4 pagesAfl Peaksun Enterprises and Export Corporation Pgaksun: 2F Peaksun Building 1505 Princeton St. Mandaluyong CityCarlo Dela CruzNo ratings yet
- BIR Form 1901 Application for RegistrationDocument4 pagesBIR Form 1901 Application for RegistrationMark Domingo MendozaNo ratings yet
- CIS Individual EditableDocument6 pagesCIS Individual EditableJUNIE DAVE ORQUITANo ratings yet
- 03/29/2000 Gamu, Isabela FilipinoDocument5 pages03/29/2000 Gamu, Isabela FilipinoSolomonNo ratings yet
- Loyalty Card Plus: Application FormDocument2 pagesLoyalty Card Plus: Application FormGlaiza Mae Olivar-ArguillesNo ratings yet
- UBP - Form DocsDocument2 pagesUBP - Form DocsJelvan RicolcolNo ratings yet
- Please Carefully Read Instructions at The Back Before Accomplishing This Form. PurposeDocument2 pagesPlease Carefully Read Instructions at The Back Before Accomplishing This Form. PurposeMosses BryanNo ratings yet
- Member'S Data Form (MDF) : Membership CategoryDocument2 pagesMember'S Data Form (MDF) : Membership CategoryRonstar Molina TanateNo ratings yet
- Customer Information Form IndividualDocument9 pagesCustomer Information Form IndividualJean MojadoNo ratings yet
- HLF1036 HousingLoanApplicationCoBorrower V01Document2 pagesHLF1036 HousingLoanApplicationCoBorrower V01Andrei Notario Manila100% (1)
- Reference No. CEF13022038-45050711202129886890Document10 pagesReference No. CEF13022038-45050711202129886890lattaeNo ratings yet
- Philippines Health Insurance FormDocument2 pagesPhilippines Health Insurance FormDBVS GRAY MORTERANo ratings yet
- Revised Incident Record Form BELITDocument2 pagesRevised Incident Record Form BELITJennie Amando100% (1)
- Wall Footing Detail: Plan PlanDocument1 pageWall Footing Detail: Plan Plancoolmer drugstore08No ratings yet
- FOUNDATION AND FRAMING PLANSDocument1 pageFOUNDATION AND FRAMING PLANScoolmer drugstore08No ratings yet
- J.M.P.F: John Michael P. Fernandez, Uap A Proposed Renovation of Two-Storey Residential UnitDocument1 pageJ.M.P.F: John Michael P. Fernandez, Uap A Proposed Renovation of Two-Storey Residential Unitcoolmer drugstore08No ratings yet
- Serology Answer Sheet 02.07.2022Document2 pagesSerology Answer Sheet 02.07.2022coolmer drugstore08No ratings yet
- Immunology Answer Sheet 02.07.2022Document1 pageImmunology Answer Sheet 02.07.2022coolmer drugstore08No ratings yet
- Matutiã - A Grezel MaeDocument1 pageMatutiã - A Grezel Maecoolmer drugstore08No ratings yet
- Controls: Instruction ManualDocument16 pagesControls: Instruction ManualOG100% (1)
- 1032 Fy Fxe Duplex Power Pump PDFDocument2 pages1032 Fy Fxe Duplex Power Pump PDFJunior Francisco QuijanoNo ratings yet
- Python Date TimeDocument6 pagesPython Date TimeNataliaNo ratings yet
- Building With Earth in Nigeria: A Review of The Past and Present Efforts To Enhance Future Housing DevelopmentsDocument15 pagesBuilding With Earth in Nigeria: A Review of The Past and Present Efforts To Enhance Future Housing DevelopmentsSANI SULEIMANNo ratings yet
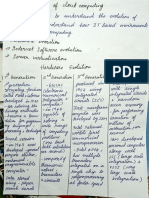
- Evolution of Cloud ComputingDocument3 pagesEvolution of Cloud ComputingVaishnavi ChockalingamNo ratings yet
- 4as119068 - Uc 500e Ed.2 Data - SheeDocument12 pages4as119068 - Uc 500e Ed.2 Data - SheeayyakkottaiyurNo ratings yet
- PTT205 Heat and Mass Transfer: EvaporatorDocument43 pagesPTT205 Heat and Mass Transfer: Evaporatorkkk100% (1)
- Hands-On Keyboard 5 - WiresharkDocument16 pagesHands-On Keyboard 5 - Wiresharkpenumudi233No ratings yet
- Prestressed ConcreteDocument66 pagesPrestressed ConcreteTech BisuNo ratings yet
- Troubleshooting PDFDocument49 pagesTroubleshooting PDFHedenarol Ramirez RojasNo ratings yet
- What Is UtautDocument2 pagesWhat Is UtautBunaya Mngwale HamisiNo ratings yet
- Workshop (03W 2205)Document152 pagesWorkshop (03W 2205)Евгений Губарев0% (2)
- Heat Exchangers: Thermal Activity and Fluid MotionDocument14 pagesHeat Exchangers: Thermal Activity and Fluid Motionishu vohraNo ratings yet
- Maintaining Critical COWP PumpsDocument7 pagesMaintaining Critical COWP PumpsScherraine Khrys CastillonNo ratings yet
- Technical ReportDocument2 pagesTechnical ReportsihamNo ratings yet
- Bk3500 BrochureDocument6 pagesBk3500 Brochurewillyg2k5No ratings yet
- Carbon FibersDocument6 pagesCarbon FibersHarish SonawaneNo ratings yet
- Hilberseimer's Theories on Urban Planning and DecentralizationDocument2 pagesHilberseimer's Theories on Urban Planning and DecentralizationSwati ThakurNo ratings yet
- Link-Belt Syntron Manual HandlingDocument160 pagesLink-Belt Syntron Manual Handlingjose castillo100% (1)
- Dan's Fanuc Spindle InfoDocument13 pagesDan's Fanuc Spindle InfoPham LongNo ratings yet
- Express Publishing Repetytorium-Test 3bDocument2 pagesExpress Publishing Repetytorium-Test 3bLena NowickaNo ratings yet
- Course Outline1Document42 pagesCourse Outline1Fierre NouxNo ratings yet
- Sample Use Case LoginDocument5 pagesSample Use Case Logindaljsinj96No ratings yet
- RTS350OperationsGuide 85Document1,400 pagesRTS350OperationsGuide 85Eduardo Valldeperas100% (1)
- BB2920-04 Cylinder Block-1Document5 pagesBB2920-04 Cylinder Block-1Volcambus SacNo ratings yet
- Mr. RONAK J BHUVA's SBI account statement from 15-16 Dec 2021Document2 pagesMr. RONAK J BHUVA's SBI account statement from 15-16 Dec 2021Ronak BhuvaNo ratings yet
- Hawker perfect plus PzB-element technical data sheetDocument6 pagesHawker perfect plus PzB-element technical data sheetcrash2804No ratings yet
- Engine Block Manufacturing ProcessDocument5 pagesEngine Block Manufacturing ProcessDavid U. AnyegwuNo ratings yet
- Difference Betweew Celeron and PentiumDocument3 pagesDifference Betweew Celeron and PentiumAkash RuhilNo ratings yet
- Device Integration Cisco WLCDocument6 pagesDevice Integration Cisco WLCSpyman_pcNo ratings yet