You might also like
- Brock Biology of Microorganisms 15th Edition Madigan Test BankDocument15 pagesBrock Biology of Microorganisms 15th Edition Madigan Test Bankloganwalkertcaenpjsid100% (31)
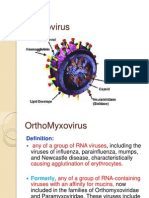
- OrthomyxovirusesDocument39 pagesOrthomyxovirusesማላያላም ማላያላምNo ratings yet
- Viral Structure and Components Properties of VirusesDocument4 pagesViral Structure and Components Properties of Virusescanela1527100% (1)
- Disease: A Deviation of The Normal Structure/function of Any Part of The Body That Is Manifested by ADocument4 pagesDisease: A Deviation of The Normal Structure/function of Any Part of The Body That Is Manifested by ADhanaNo ratings yet
- Chemical Biology: SARS-CoV-2Document9 pagesChemical Biology: SARS-CoV-2Eliakim InsongNo ratings yet
- Attachment and Entry of VirusesDocument34 pagesAttachment and Entry of VirusesAnonymous ekWj8dNo ratings yet
- Virology Course 1Document33 pagesVirology Course 1Uyisabye VénusteNo ratings yet
- Clinical Virology (Dental)Document134 pagesClinical Virology (Dental)samar yousif mohamedNo ratings yet
- Viruses: Shafie Abdulkadir HassanDocument29 pagesViruses: Shafie Abdulkadir HassanShafici CqadirNo ratings yet
- Patrick Ch17Document49 pagesPatrick Ch17Caroline Lessa0% (1)
- Chapter 5: VIRUS 18 - Lacap, Dixie Mae N. Lacap 02. .15Document10 pagesChapter 5: VIRUS 18 - Lacap, Dixie Mae N. Lacap 02. .15Dixie LacapNo ratings yet
- Herpes Simplex Type 1&2Document15 pagesHerpes Simplex Type 1&2ulfah febyNo ratings yet
- Chap 13 Reading WorksheetDocument6 pagesChap 13 Reading WorksheetSarahNo ratings yet
- ArenavirusDocument29 pagesArenavirusRamirez GiovarNo ratings yet
- Biochemistry of CoronaDocument19 pagesBiochemistry of CoronaNikos FinnosNo ratings yet
- Rabies Virus: RhabdovirusesDocument18 pagesRabies Virus: RhabdovirusesHaydas ChannelNo ratings yet
- Viruses:: The Non-Living EntityDocument48 pagesViruses:: The Non-Living EntityhannNo ratings yet
- Day 5 Virology - January 2021Document183 pagesDay 5 Virology - January 2021ShriefElghazalyNo ratings yet
- VIRUSES, Viroids and PrionsDocument66 pagesVIRUSES, Viroids and PrionsGabz GabbyNo ratings yet
- Cellular Structure of Covid 19Document11 pagesCellular Structure of Covid 19atikamaryemNo ratings yet
- Virology of Human Immunodeficiency VirusDocument13 pagesVirology of Human Immunodeficiency Virusemmanuelnwa943No ratings yet
- BIO 2B VirusesDocument47 pagesBIO 2B VirusesRegine FeynmanNo ratings yet
- Human Immunodeficiency Virus (HIV)Document34 pagesHuman Immunodeficiency Virus (HIV)Ahmed SafaNo ratings yet
- Viral ReplicationDocument26 pagesViral ReplicationJhann100% (1)
- Can ZN Be A Critical Element in COVID 19Document9 pagesCan ZN Be A Critical Element in COVID 19gygyNo ratings yet
- Disusun Oleh: Dr. H. Deddy HartantoDocument63 pagesDisusun Oleh: Dr. H. Deddy HartantoAnonymous UbA0ZHCKeNo ratings yet
- VirologyDocument58 pagesVirologymohamedNo ratings yet
- Sars-Cov-2: Phylogenetic Status, Mutations and Therapeutic Research Based On Spike ProteinDocument10 pagesSars-Cov-2: Phylogenetic Status, Mutations and Therapeutic Research Based On Spike ProteinArley GutarraNo ratings yet
- Corona Virus: Q1: Coronavirus Life CycleDocument6 pagesCorona Virus: Q1: Coronavirus Life CycleTufail KhanNo ratings yet
- RapioDocument7 pagesRapioÑaazir ŘomiőNo ratings yet
- Lecture 3Document3 pagesLecture 3Alexandra AlexaNo ratings yet
- Biology of Sars-Cov-2: InfectionDocument3 pagesBiology of Sars-Cov-2: InfectionGlenard EstanteNo ratings yet
- Herpes VirusesDocument6 pagesHerpes VirusesAlya Putri KhairaniNo ratings yet
- 5 Basic VirologyDocument71 pages5 Basic VirologyErdemNo ratings yet
- Virology SummaryDocument24 pagesVirology Summarykevin100% (1)
- Viruses PrintDocument4 pagesViruses PrintAlmaNo ratings yet
- Virology Assisnment 511Document6 pagesVirology Assisnment 511SYED FARHADNo ratings yet
- Rahman-Idid2021 Article CanZnBeACriticalElementInCOVIDDocument9 pagesRahman-Idid2021 Article CanZnBeACriticalElementInCOVIDTu TuongNo ratings yet
- May Be Defined As: VirusesDocument21 pagesMay Be Defined As: VirusesZeresenayNo ratings yet
- Arthropod Borne DiseasesDocument40 pagesArthropod Borne Diseasessamhossain1907No ratings yet
- SARS Vaccine Development: Shibo Jiang, Yuxian He, and Shuwen LiuDocument5 pagesSARS Vaccine Development: Shibo Jiang, Yuxian He, and Shuwen LiuDesiree LesterNo ratings yet
- Virology FinalDocument11 pagesVirology FinalAvin AdamNo ratings yet
- COVID-19 - Where Did It Come FromDocument3 pagesCOVID-19 - Where Did It Come FromKryzler KayeNo ratings yet
- Nomenclature of Virus ProteinsDocument11 pagesNomenclature of Virus ProteinslkokodkodNo ratings yet
- New ChallengeDocument3 pagesNew ChallengeEliana TorresNo ratings yet
- DNA Enveloped Viruses 2Document13 pagesDNA Enveloped Viruses 2Tamara ElyasNo ratings yet
- AIDS (HIV Virus) SalmanDocument17 pagesAIDS (HIV Virus) SalmanFuad AzabNo ratings yet
- Rhabdoviridae: Rabies VirusDocument13 pagesRhabdoviridae: Rabies Virusميمونه عبد الرحيم مصطفىNo ratings yet
- Viruses: Viral SizeDocument5 pagesViruses: Viral SizeSharmeen MohammadNo ratings yet
- HML 214 Lecture 6 2021Document37 pagesHML 214 Lecture 6 2021Linet KariukiNo ratings yet
- Self Discussion QuestionsDocument23 pagesSelf Discussion QuestionsbramguyNo ratings yet
- Chapter 2.4Document28 pagesChapter 2.4Clare MercadoNo ratings yet
- Coronavirus (COVID-19) Quiz Review For NursesDocument11 pagesCoronavirus (COVID-19) Quiz Review For Nurseshasan ahmdNo ratings yet
- Prof Lisyani - SARS-CoV-2 ReinfectionDocument41 pagesProf Lisyani - SARS-CoV-2 ReinfectionEldo TaufilaNo ratings yet
- Spread Thru Olfactory BulbDocument2 pagesSpread Thru Olfactory BulbleoNo ratings yet
- Hand OutDocument8 pagesHand Outhandoko142No ratings yet
- 01 - General Structure and Classification of Viruses1Document38 pages01 - General Structure and Classification of Viruses1Rahul Kumar100% (1)
- Viral CNS Infections - Polio, Rabies Group PresentationDocument49 pagesViral CNS Infections - Polio, Rabies Group Presentationodhiambo samwelNo ratings yet
- Biology of Hiv Particle Description of HIV Particle A) Classification of HIV ParticleDocument10 pagesBiology of Hiv Particle Description of HIV Particle A) Classification of HIV ParticlevictoriousNo ratings yet
- Virology NotesDocument46 pagesVirology NotesJoseph ChanNo ratings yet
- Poliomyelitis CDCDocument12 pagesPoliomyelitis CDCAsiah JelitaNo ratings yet
- Virology The Study of VirusesDocument45 pagesVirology The Study of Virusesdawoodabdullah56100% (2)
- Polio Virus - Assignment PDFDocument12 pagesPolio Virus - Assignment PDFSalu kSNo ratings yet
- Virus Literacy GuideDocument4 pagesVirus Literacy GuideMaurice WashingtonNo ratings yet
- PEDIATRICSDocument51 pagesPEDIATRICSJoanne BlancoNo ratings yet
- Multiple Antiviral Activities of Endemic Medicinal Plants Used by Berber Peoples of MoroccoDocument12 pagesMultiple Antiviral Activities of Endemic Medicinal Plants Used by Berber Peoples of MoroccomohamedtlNo ratings yet
- Ncs University System Department of Health Sciences: Discipline (MLT-04) (VIROLOGY &MYCOLOGY)Document5 pagesNcs University System Department of Health Sciences: Discipline (MLT-04) (VIROLOGY &MYCOLOGY)Habib UllahNo ratings yet
- What Are Viruses?Document5 pagesWhat Are Viruses?ZJC 2333No ratings yet
- Oral Polio Vaccine Product Insert by GlaxoSmithKlineDocument7 pagesOral Polio Vaccine Product Insert by GlaxoSmithKlineHeather X RhodesNo ratings yet
- Plugging Medical BrainDocument3 pagesPlugging Medical BrainAprilVivienCuNo ratings yet
- Drug Study of Oral Polio VaccineDocument2 pagesDrug Study of Oral Polio VaccineDeanne Stephanie Hordista100% (1)
- Enteroviruses: Presented By: Andrea Dora J. Ortaliz MD-2Document56 pagesEnteroviruses: Presented By: Andrea Dora J. Ortaliz MD-2Andrea Dora OrtalizNo ratings yet
- Viral PathogenesisDocument57 pagesViral PathogenesisrezailakotamaNo ratings yet
- Polio Eradication: Global Update & ExperienceDocument32 pagesPolio Eradication: Global Update & ExperiencePankaj AgrawalNo ratings yet
- Research PaperDocument55 pagesResearch PaperAakriti AhlawatNo ratings yet
- PoliomyelitisDocument43 pagesPoliomyelitistummalapalli venkateswara rao100% (4)
- Micro Levinson QuestionsDocument30 pagesMicro Levinson QuestionsadehkordiNo ratings yet
- Oral Polio Vaccine and Inactivated Polio VaccineDocument8 pagesOral Polio Vaccine and Inactivated Polio VaccineJennalyn Padua SevillaNo ratings yet
- Finkelstein DissertationDocument362 pagesFinkelstein DissertationOslo SaputraNo ratings yet
- Afp For MbbsDocument65 pagesAfp For MbbsShyam Sundar SNo ratings yet
- 2 - Introduction To VirusesDocument32 pages2 - Introduction To VirusesrostandtchangoueNo ratings yet
- EBV & PoliovirusDocument10 pagesEBV & PoliovirusIkea BalhonNo ratings yet
- Fifth Meeting of The Containment Advisory GroupDocument51 pagesFifth Meeting of The Containment Advisory GroupRaviKumarNo ratings yet
- Nurses' Roles in Disease SurveillanceDocument9 pagesNurses' Roles in Disease SurveillanceGenevieve MundalaNo ratings yet
- Polio and PreventionDocument2 pagesPolio and PreventionPintu KumarNo ratings yet
- PoliomyelitisDocument50 pagesPoliomyelitisJohn John TorresNo ratings yet
- Vaccination or ImmunizationDocument4 pagesVaccination or ImmunizationPrincessNo ratings yet
- PolioDocument14 pagesPolioapi-31767091450% (2)
- CD Part 2 - Communicable Diseases With Pics (1) ConDocument239 pagesCD Part 2 - Communicable Diseases With Pics (1) ConMackoi SalamanesNo ratings yet