Volume 7, Issue 12, December – 2022 International Journal of Innovative Science and Research Technology
ISSN No:-2456-2165
Role of Primary Health Centre for Cancer
Management and People Preference
Kowsalya Murugan, Dr. Rupa Gunaseelan
RUSA, Bharathiar University, Coimbatore – 046.
Abstract:- At present Cancer is found to be one of the Health, Peer Reviewed Journals). In India, the National
largest deaths causing disease worldwide and its Health Mission (NHM) aims to provide universal access to
incidence is also growing. Government owned primary fair, accessible, and high-quality health-care services that
health center (PHC) is located all over the country to are accountable and responsive to people's needs (National
provide good health services to the public. These PHCs Health mission, National Health Portal of India). Under the
plays a vital role in fulfilling the basic health services for NHM, Primary Health Centre (PHC) is established to cover
all the diseases by giving primary diagnosis and a population of 30,000 in rural areas and 20,000 in hilly,
screening facility at nearby. In every PHC there is a tribal and desert areas. The concept of Primary Health
special Non-Communicable Disease (NCD) staff nurse Centre (PHC) is introduced by the Bhore Committee in
who exclusively concentrates the Non communicable 1946. The Bhore Committee proposed the concept of
disease patients; they provide services from screening till Primary Health Centres (PHCs) in 1946. They proposed the
their palliative care. The services provided by the PHCs concept of a PHC as a basic health unit to offer integrated
are not utilized by the people to its fullest due to some of curative and preventive health care to the rural population as
the inconvenience faced by them. If these facilities are near to the people as feasible, with an emphasis on
made better and the requirement of the public is met preventive and promotive components of health care. In
out, the resources will be used fully. Hence there is a India, health planners see the Primary Health Centre (PHC)
need to enhance the role of PHC and to improve the and its Sub-Centres (SCs) as the necessary infrastructure for
facilities provided. This chapter aims to explore the role providing health services to the rural population (Indian
of Primary health center in prevention, early detection Public Health Standards).
and cancer control measures.
The Central Council of Health, at its first meeting held
Keywords:- Primary Health Center, People preference, in January 1953, had recommended the establishment of
cancer, early screening PHCs in community development blocks to provide
comprehensive health care to the rural people. For more
I. INTRODUCTION effective coverage, the 6th Five-Year Plan (1983-88)
advocated reorganizing PHCs on the basis of one PHC for
The PHCs in Tamil Nadu is having a good system for every 30,000 rural people in the plains and one PHC for
cancer management right from early screening till their every 20,000 population in mountainous, tribal, and desert
palliative care. But the system is not utilized in the way as it areas (Indian Public Health Standards). A Sub-Health
is mapped for the welfare of the public. This is because the Centre is the most remote and initial point of interaction
people expect a clean environment, lesser waiting time, between the primary health care system and the community
adequate nurses and a good ambiance. They feel that private in the public sector (Uday W. Narlawar, 2018). The
hospitals have these facilities and hence they prefer to go Minimum Needs Program (MNP) was implemented
there. Also, people living in rural areas do not have throughout the country during the first year of the Fifth
knowledge about the PHC’s cancer screening facility. This Five-Year Plan (1974–78), with the goal of meeting certain
lack of awareness will cause more burden in people as they fundamental needs and so raising people's living conditions.
end with later stage discovery of the disease. It eventually The goal in terms of rural health was to build one Sub-
leads to a higher level of mortality in the society. Therefore, centre for a population of 5000 people in the plains and
there is a need to fulfill the facilities required by the people, 3000 in tribal and mountainous areas, one Primary Health
so that they will make use of the services available at PHCs. Centre (PHC) for 30000 population in plains and for a
II. PRIMARY HEALTH CENTERS population of 120000 in the plains and 80000 in tribal and
hilly areas, there is one Community Health Centre
India has a vast population with a wide range of (CHC/Rural Hospital).
people living. The more densely populated comes with more
challenges in handling the life for meeting out the healthy A sub-centre serves as a point of contact for the
wellbeing of the society. According to World Health community at large, delivering all basic health care services.
Organization, Primary health care (PHC) handles the vast Sub-centres, Primary Health Centres, Community Health
majority of a person's health requirements over the course of Centres, Sub- Divisional/Sub-District Hospitals, and District
their life. This covers physical, emotional, and social well- Hospitals make up the bottom rung of a referral pyramid of
being, and it is focused on individuals rather than diseases. health services (Indian Public Health Standards). The
PHC is a comprehensive approach to health that purpose of Health Sub- centre goal is to prevent and
encompasses health promotion, illness prevention, promote health, but it also provides basic curative treatment
treatment, rehabilitation, and palliative care (Primary (Priyadarsini Suresh, 2018). PHCs are the cornerstone of
IJISRT22DEC825 www.ijisrt.com 625
Volume 7, Issue 12, December – 2022 International Journal of Innovative Science and Research Technology
ISSN No:-2456-2165
rural health services, serving as a first point of contact for third among countries in the world, with an estimated cancer
the ill and those who are referred directly or indirectly from burden of 1.2 million new patients, and second with 7.85
Sub-Centres for curative, preventative, and promotive health lakh cancer- related fatalities. The age-standardized rates per
care. It serves as a referral unit for six Sub-Centres, referring lakh population were 89.4 and 61.4, respectively
cases to Community Health Centres (30-bed hospitals) and (GLOBOCAN, 2018). The registration of new cancer
higher-order public hospitals at sub-district and district occurrences through Population Based Cancer Registries
levels. There are six indoor beds for patients. (Indian Public (PBCR) has been practiced in the state for the past 35 years
Health Standards). Community Health Centres (CHCs), in which Madras Metropolitan Tumor Registry (MMTR)
which make up the First Referral Units (FRUs), and Sub- from 1982 covers 4.8 million population entirely (urban)
district and District Hospitals make up the secondary level residing within the metropolitan limits of Chennai city, and
of health care. The CHCs were created to offer referral Dindigul Ambilikkai Cancer Registry (DACR) from 2003
health care for cases that came from Primary Health Centres covers 2.2 million population (predominantly rural) residing
as well as cases that came to the centre directly in need of in the district of Dindigul. In Tamil Nadu, the Cancer
expert treatment (Pandve HT, 2015). Under each CHC, occurrence incidence rate for one lakh of population is 84.2
typically 4 PHCs are included, serving around 80,000 out of that, 74.5 is male and 93.8 is female. The cumulative
people in tribal/hilly/desert areas and 1,20,000 people in risk of cancer occurrence in one’s life span of 0 – 74 years
plain areas. CHC is a 30-bed hospital that specialises in of age was one-in-12 among women and one-in- eleven
Medicine, Obstetrics and Gynaecology, Surgery, among men. The crude incidence rate of cancer in
Paediatrics, Dental and AYUSH (Indian Public Health Coimbatore district during the year 2016 is 84.9 for male
Standards). and 95.5 for female per one lakh population
(Implementation of Cancer Prevention and Control Policy
III. THREE TIER HEALTH CARE DELIVERY IN for state, 2020)
TAMIL NADU
V. METHODS
Primary care covers a population range between 3000-
5000 in Health Sub Centres (HSC) and population range In this research descriptive way of studying the
between 20,000-30,000 in Primary Health Centres (PHC). characteristic of the population is carried out. The
The Secondary Care covers a population range between population taken for the study is based on the census of
80,000-120,000 in Community Health Centres (CHC) and Coimbatore district in 2011 which is segmented according
District Hospitals covering population in the entire district. to their respective taluks. Taluks covering Coimbatore
The Tertiary Care includes Speciality Hospitals, Regional North, Coimbatore South, Mettupalayam, Pollachi, Sulur
and Central Institutions/Medical Colleges. and Valparai. To a total population of 34,58,045 people the
confined sample size is taken. The sample size is selected
IV. CANCER BURDEN using stratified sampling method, in which the population is
segmented into taluks and again the samples are selected
Cancer is an uncontrollable growth of abnormal cells using random sampling method.
in any organ or tissue of the body. In the world, cancer is
the second leading cause of death which accounts for about A. Sample Size
9.6 million deaths in 2018. The most common types of The sample size taken for the study is 387 respondents
cancer in Men are lung, prostate, colorectal, stomach, oral who are the representation of the population in this
and liver cancer. For women breast, cervical, colorectal, study.The target population of the study are the residents of
lung and thyroid cancer are the most common types of Coimbatore district. According to census 2011, Coimbatore
cancer. According to WHO, Globally the burden for cancer district has 34,58,045 people in its population. This study
continues to grow tremendously on physical, emotional and stratified the population based on its taluks covering
economic conditions for individuals, families and health Coimbatore North, Coimbatore South, Mettupalayam,
systems. Many health care systems in low- and middle- Pollachi, Sulur and Valparai.
income countries are insufficient to cope with this burden,
and a huge percentage of cancer patients worldwide lack B. Data Collection
access to timely, high-quality diagnosis and treatment. Data collection was initiated through pilot study with10
Survival rates for many forms of cancer are increasing in percent of the sample size and analyzed for their reliability
nations with strong health systems owing to early detection, (n=50). Samples are generated by collection of contact
quality treatment and survivorship care. details of respective people in each taluk. And then followed
by randomly sending the online survey forms to each of
The role of Primary Health Centre in cancer them. Similarly, the process is repeated in meeting
management plays an important part in screening and respondents personally on each taluk. Data were collected
diagnosing cancer at an early stage. Non-Communicable using two type of questionnaire format, in which one focus
Diseases or NCDs presently causes more death rate than all on personal interviews with doctors & nurses for deeper
other causes combined, and deaths from NCDs are expected understanding of PHC Cancer Management. Second
to rise from 38 million in 2012 to 52 million by 2030. About questionnaire includes demographic information about the
82 % of mortality rate are caused due to these four major respondents, and the constructs covered in the study were
NCDs namely Cardiovascular Diseases, Cancer, Chronic gathered using Likert five-point scaling and services
Respiratory Diseases and Diabetes. In 2018, India ranked provided in PHCs were framed using dichotomous questions
IJISRT22DEC825 www.ijisrt.com 626
Volume 7, Issue 12, December – 2022 International Journal of Innovative Science and Research Technology
ISSN No:-2456-2165
were collected from general public. To the proportion of A special NCD Staff nurse is appointed exclusively for
each taluk and their respective population, samples were screening of cancer at every PHC. These services come
collected. Data collected from online and hard copy are under the Government’s National Programme for Prevention
decoded according to the numeric form for statistical and Control of Cancer, Diabetes, Cardiovascular Diseases
analysis. The statistical software used for the analysis is and Stroke (NPCDCS). Tamil Nadu government as a part of
IBM SPSS to undergo chi-square test and percentage NPCDCS has initiated a scheme called Amma Arokiya
analysis in the study. To the base of interpretation, all Thittam (AAT) to undergo Annual Wellness Check-up. In
obtained data were analyzed. Questionnaires are made line with this scheme, NCD staff nurses will maintain a
available in two languages which include Tamil (regional separate register to enter the patient details who attend the
language) and English for the participants to choose from. Annual Wellness Check-up at PHC.
As a part of this study, the researcher visited and
interviewed Doctors and NCD staff nurses of Primary Patient details are entered in Health Management
Health Centers located within Coimbatore district. i) Information System (HMIS) web portal by using NCD Staff
Government Primary Health Center, Vagarayampalayam, Nurse User ID. The staff nurse will collect and update the
Sulur Taluk, ii) Upgraded Primary Health Center, Somanur, ration card & Aadhaar card details during registration in
Sulur Taluk, iii) Government Primary Health Center, order to avoid duplication and create a comprehensive
Pogalur, Annur Taluk, iv) Government Primary Health Electronic Health Record (EHR) for the individual
Center, Mookanur, Annur Taluk, v) Government Primary beneficiary. Monitoring of patients at an equal interval by
Health Center, Karamadai, Mettupalayam Taluk were the staff nurse to ensure their current progressive health
visited to understand the current practices involved in conditions. The data collected by the NCD staff nurse will
managing Cancer patients at PHCs. be submitted every month to the NCD District Health
Officer for review.
VI. RESULT
From the data collected using questionnaire one by
interviewing with Nurses and Doctors of various Primary
Health Centers, it is understood that the treatment for cancer
disease at a PHC includes right from screening of
malignancy till palliative care. The Primary Health Centers
screens every person visiting, who are above 18 years of
age. The persons who were suspected are referred to the
secondary care/district hospitals for further confirmation. If
the disease is confirmed for the person, they will be
monitored and guided by the NCD staff nurse of PHCs. Post
confirmation of the diagnosis, these patients will be
continuously followed up by the respective NCD staff
nurses till their palliative care.
IJISRT22DEC825 www.ijisrt.com 627
Volume 7, Issue 12, December – 2022 International Journal of Innovative Science and Research Technology
ISSN No:-2456-2165
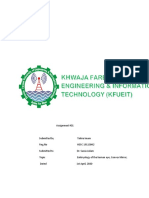
Fig. 1: Current method adopted by Primary Health Centre in Cancer Management
An enhancement training will be given to the NCD staff nurses for every six months. The following flowchart explains the
current method adopted by primary health centers in cancermanagement.
IJISRT22DEC825 www.ijisrt.com 628
Volume 7, Issue 12, December – 2022 International Journal of Innovative Science and Research Technology
ISSN No:-2456-2165
(n=387)
Profile Frequency (%)
Location
Mettupalayam 29 (7.5)
Sulur 36 (9.3)
Coimbatore North 71 (18.3)
Coimbatore South 178 (46.0)
Pollachi 65 (16.8)
Valparai 8 (2.1)
Gender
Male 203 (52.5)
Female 184 (47.5)
Age
Below 18 6 (2)
18-24 116 (30)
25-34 163 42)
35-44 64 (17)
45-54 21 (5)
55-64 11 (3)
65 and above 6 (2)
Marital Status
Married 250 (65)
Single 137 (35)
Qualification
School and below 30 (8)
Undergraduate 152 (39)
Post graduate and above 186 (48)
Others 19 (5)
Occupation
Government employee 42 (11)
Private employee 124 (32)
Business 32 (8)
Professional 58 (15)
Others 131 (34)
Family Income
Less than 10,000 42 (11)
11,000-20,000 97 (25)
21,000-30,000 69 (18)
31,000-40,000 43 (11)
41,000-50,000 34 (9)
51,000 and above 67 (17)
No income 35 (9)
Family Members
2 Members 31 (8)
3-4 Members 280 (72.4)
5-7 Members 73 (18.9)
8 and above 3 (0.8)
Table 1: Demographic profile of respondents
According to census 2011, Location of the respondents difference prevailing among male and female. In Gender, 53
based on their Taluk were collected and analyzed. In which, percent are Male and 47 percent arefemale. Therefore, there
Coimbatore South shows higher responses of 46 percent as is almost equal responses registered irrespective of gender.
per population. And Valparai having low population among Age of the respondents clearly explains the respondents’
all other taluks shows lower responses. Coimbatore North preferences over each segment. Age 25-34 shows greater
and Pollachi shows similar response rate. Coimbatore involvement in responding to the survey.18-24 shows
district population is sub grouped based on their taluk moderate level of responses.18 – 34 age contributes more
according to 2011 census reports. There is a less Significant for the survey. Respondents’ marital status also determines
IJISRT22DEC825 www.ijisrt.com 629
Volume 7, Issue 12, December – 2022 International Journal of Innovative Science and Research Technology
ISSN No:-2456-2165
their decision towards choosing health services to their choosing health services. Family income of the respondents
families.65 percent of the respondents are married and 35 whose income range is of 11,000 – 20,000 responded to
percent are unmarried. Educational Qualification of the about 25 percent, which is greater than all other responses.
respondents influences the interest towards hospital The responses from income range of 21,000-30,000 showed
selection. About 48 percent of respondents were from post 18 percent of their involvement. 41,000 – 50,000 is the least
graduate and above. 39 percent are Undergraduate. count registered by respondents. Respondents having 3-4
Schooling and below are registered as 8 percent for members in a family showed 72 percent of interest towards
respondents educational qualification. Private employees’ the survey. It clearly shows that most of them are nuclear
contribution towards survey is about 32 percent. And others families, while 20 percentage of population are living as
who includes students contributed to about 34 percent. joint family.
Occupation weighs more on family’s preference for
PHC NCD SCREENING PARAMETERS KNOWLEDGE
329
350 287
325
300
284 289
250 259 266
303 243
200 290
238 243
150 214 222 216 260
203 213
198 197
100
189 190
173 165 174 171
121
144 149 103 98
144
84 184 128
127
00
1 97
50
62 58
0
yes no
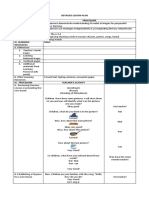
Fig. 2: PHC - NCD screening parameters knowledge among people
The above mentioned are the basic Non- lack of awareness regarding the availability of services such
Communicable Diseases (NCD) service parameters as Peripheral smear, blood creatinine, Ultrasound, Electro
available at Primary Health Centre (PHC). From the figure Cardio Gram, X-ray, Sputum Microscopy, Ophthalmic
1.1 it is inferred that, the respondent’s awareness level is screening and Dermatological screening. Among all these
higher for parameters such as Body Mass Index, Blood parameters, Screening for Cervical, Breast and Oral Cancer
Pressure, Blood Total Count, Blood Differential Count, have very low awareness when compared to other NCD
Hemoglobin, Blood Grouping and Typing, Random Blood services provided by PHCs. There is an immediate need to
Sugar, Blood Cholesterol and Urinary Test. While there is a educate people about the available tests for cancer early
IJISRT22DEC825 www.ijisrt.com 630
Volume 7, Issue 12, December – 2022 International Journal of Innovative Science and Research Technology
ISSN No:-2456-2165
screening so as to lower the mortality rate. Knowledge of respondents. Whereas parameters such as screening for
people regarding NCD parameters differs for each service Ultrasound test, Screening for Cervical cancer, Screening
offered at PHCs. In which Height, Weight, Body mass for Breast cancer, Screening for Oral cancer shows lower
index, Blood pressure, Blood sugar, Blood cholesterol and awareness.
Urinary tests shows a greater awareness among the
n=387
People Preference on PHCs Response Frequency Percentage
Did the ambience inside the PHC is welcoming Strongly disagree 24 6.2
to you?
Disagree 64 16.5
Neutral 152 39.3
Agree 93 24.0
Strongly 54 14.0
agree
Do you think the infrastructure of a PHC is Strongly 44 11.4
similar to that of a local private hospital? disagree
Disagree 87 22.5
Neutral 134 34.6
Agree 87 22.5
Strongly 35 9.0
agree
Is cleanliness in PHC is similar to that of a Strongly 58 15.0
private hospital? disagree
Disagree 90 23.3
Neutral 132 34.1
Agree 75 19.4
Strongly 32 8.3
agree
Does the distance of your nearby PHC is easily Strongly 29 7.5
accessible to you than a private hospital? disagree
Disagree 47 12.1
Neutral 115 29.7
Agree 112 28.9
Strongly 84 21.7
agree
Do you feel that your nearby PHC is having Strongly 45 11.6
adequate space for undergoing treatments? disagree
Disagree 88 22.7
Neutral 120 31.0
Agree 85 22.0
Strongly 49 12.7
agree
Table 2: People preference on Primary Health Centers
From the table it is inferred that, 14 percent of the respondents agrees that both PHC and local private hospital
respondents strongly agree that the ambience inside a Primary are similar, whereas 11 percent strongly disagree with the
Health Center is good. While 24 percent agreed that the infrastructure similarity. And 35 percent of the respondence
ambience is welcoming to them. 39 percent respondents have have no idea about the same. For cleanliness, about 19
no idea regarding the PHC environment. About 17 percent percent agrees that the cleanliness is good in PHCs than that
disagree with the content. Adding to that about 6 percent of of a private hospital. While 34 percent don’t find any
respondents strongly disagree with the existing ambience difference or they don’t notice such differences. 23 percent
inside a PHC. Similarity of the infrastructure in a PHC to disagree with cleanliness of a PHC as they feel that PHC are
that of a local private hospital by which23 percent of not clean to their expectation. When the respondents are
IJISRT22DEC825 www.ijisrt.com 631
Volume 7, Issue 12, December – 2022 International Journal of Innovative Science and Research Technology
ISSN No:-2456-2165
questioned regarding the PHC locality and its accessibility for that the patients are referred for further treatments at District
treatments, about 29 percent agreed with PHCs are near to Government Hospital. However, people’s awareness towards
them and 30 percent were not sure about the PHCs distance. cancer and its screening tends to be less due to their
12 percent don’t feel that the distance of a private hospital inadequate exposure about the disease. The hesitation and the
more accessible than PHC. The adequate space for a PHC to fear factor set back many of them from undergoing screening
undergo treatments results with 22 percent of agreeableness. for cancer. Majority of people have not visited PHC and
And 31 percent were neutral about their opinion towards hence they don’t know the services provided by the PHC.
space. 23 percent disagree with the adequate space for External aspects such as infrastructure, waiting time and
undergoing treatments at PHC. ambiance are the major reasons for people not visiting PHCs.
This research is mainly focused to create awareness among
VII. DISCUSSION people regarding the services provided by PHCs for initial
screening and diagnosis of cancer, also suggest enhancing the
From this study, it is understood that people don’t have facilities of PHCs at Coimbatore District of Tamil Nadu. This
enough knowledge regarding the services rendered by research has taken a speck of geographical area in Tamil
Primary Health Centers. In addition, people do not have Nadu. Therefore, further researchers can be developed in
enough knowledge on cancer and its crucial impact. Due to various geographical areas in Tamil Nadu as well as in India.
lack of knowledge, the disease is diagnosed only at its later Also, future studies can be concentrated on comparative study
stage. This leads to increase in morbidity and results in higher of treatment of cancer at Government Hospitals to that of
mortality rate. In spite of Government providing all the Private Hospitals. Further studies can be made specifically on
facilities at PHCs for free, people are spending more by the problems faced by NCD staff nurses in handling patients.
taking medical services at private sectors. The same scenario Comparative research can be carried out on the difficulties
is followed by people for cancer and its related treatments. In faced by public in Urban and Rural areas for cancer
particular with cancer disease, right from screening till treatments. Extended comparative research on the impact of
palliative care the cost incurred for undergoing such lifestyle changes with regard to susceptibility to cancer at
treatments at private hospitals were unaffordable for most of young age.
the families. While Primary Health Centres & Government
hospitals provide same and even better services at free of REFERENCES
cost. Hence people have to be educated about the available
Government health facilities in-order to utilize them for their [1.] GLOBOCAN (Global Burden of Cancer) 2018.
own benefit. The Department of Health and Family Welfare International Agency for Research on Cancer, Lyon,
of Government of Tamil Nadu, is having an effective medical France,2018. https://gco.iarc.fr/today/home
service facility to ensure the wellness of the public. [2.] Indian Public Health Standards, Guidelines For
Implementation of cancer prevention and control policy by Primary Health Centers
Tamil Nadu Government for the people is working https://nhm.gov.in/images/pdf/guidelines/iphs/iphs-
efficiently, but the awareness among the people regarding revised-guidlines-2012/primay-health- centres.pdf
those services is lagging. Due to which the services are not [3.] Implementation of Cancer Prevention and Control
fully utilized. And people perception towards Government Policy for state, 2020. G.O (Ms) No.228 Health and
medical services were not satisfactory because of longer Family Welfare (EAP II-1) Department dated
waiting time, unappealing infrastructure of hospitals, 02.06.2020
unhygienic environment. There is an urgent need to ensure [4.] Ministry of Health and Family Welfare, Number of
the right proportion of medical staff to be available at all Primary Health Centres (PHCs) Functioning In Rural
PHCs according to the population of the respective area. And Urban Areas,2019. https://pib.gov.in/PressRelease
Renovation of hospital buildings is necessary, so that people Page.aspx? PRID=1656190
can get the same aesthetic view as that of a private hospital. [5.] National Health mission, National Health Portal of
Proper disposal of medical waste on daily basis is required in India. https://www.nhp.gov.in/national- health-
order to avoid dumping of these wastes within the PHC’s mission_pg
campus. This will eradicate health related issues caused by [6.] Pandve HT, Giri PA (2015). “First referral units
biomedical wastes. (FRU): needs focus in Indian context”. Int J
Community Med Public Health; 2:75-6
VIII. CONCLUSION [7.] Primary Health, Journal of Pharmaceutical Care &
Primary Health Centres plays a vital role in diagnosing Health Systems, ISSN: 2376-0419.
cancer at its early stage. The Department of Health and https://www.longdom.org/peer-reviewed-
Family Welfare of Government of Tamil Nadu provides state journals/primary-health-3224.html
of the art facility in managing health services throughout the [8.] Priyadarsini Suresh, Steffi Sam, Robin Lizzy Sunny,
state. Primary Health Centres are located throughout the city Rony Sunny, Jabeen Banu, Ajitha Katta, Suresh
based on their respective population. The introduction of Munuswamy (2018). “Estimating spatial accessibility
Amma ArokiyaThittam (AAT) for treating Non- of public primary health care precisely”. 19th Esri
Communicable Diseases is a great benefit to people of Tamil India User Conference 2018.
Nadu. The screening facilities available at PHCs for early [9.] Report of National Cancer Registry Programme 2020,
detection of cancer help in reduction of morbidity and National Cancer Registry.
mortality rate. NCD staff nurse available at PHC make sure https://www.ncdirindia.org/All_Reports/Report_2020/
default.aspx
IJISRT22DEC825 www.ijisrt.com 632
Volume 7, Issue 12, December – 2022 International Journal of Innovative Science and Research Technology
ISSN No:-2456-2165
[10.] Rural Health: National Health Mission, Gujarat, 2021.
https://nhm.gujarat.gov.in/tribal- rch1.htm
[11.] Uday W. Narlawar, Ujjwal Sourav (2018).
"Assessment of Physical Infrastructure of sub- centres
in Central India as per Indian Public Health Standards
2012 Guidelines: A Cross Sectional Study". JMSCR
Vol 06,Issue 03,Page 160-164
[12.] World Health Organization, Primary Health Care,
India. https://www.who.int/india/health-
topics/primary-health-care
IJISRT22DEC825 www.ijisrt.com 633
You might also like
- Review-Health Systems in India PDFDocument4 pagesReview-Health Systems in India PDFTehMarianNo ratings yet
- Introduction of Health Care Services Under Ayushman Bharat Pradhan Mantri Jan Arogya Yojana AB (PM-JAY) - A Literature ReviewDocument6 pagesIntroduction of Health Care Services Under Ayushman Bharat Pradhan Mantri Jan Arogya Yojana AB (PM-JAY) - A Literature ReviewInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Rural Health in Andhra PradeshDocument5 pagesRural Health in Andhra PradeshInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Healthcare Systems Its Challenges in PakistanDocument7 pagesHealthcare Systems Its Challenges in PakistanYusra NazNo ratings yet
- CC-5 ACCESS TO RURAL HEALTHCARE-minDocument12 pagesCC-5 ACCESS TO RURAL HEALTHCARE-minsmsunil12345No ratings yet
- Unit Wise Question Will Come in Final Exam Unit 1: Q 2 ObjectivesDocument54 pagesUnit Wise Question Will Come in Final Exam Unit 1: Q 2 ObjectivesPoonam Yadav roll no.53No ratings yet
- PHC NotesDocument24 pagesPHC Notessky724526No ratings yet
- Aalok Ranjan ChaurasiaDocument41 pagesAalok Ranjan ChaurasiaHemlata GuptaNo ratings yet
- Primary Health Centre Organization and FunctionsDocument9 pagesPrimary Health Centre Organization and FunctionsKailash NagarNo ratings yet
- National Health and FamilyDocument16 pagesNational Health and FamilyshivaniNo ratings yet
- Healthcare IndustryDocument3 pagesHealthcare IndustryMohammad ImranNo ratings yet
- Pharmacist As Primary Health Care ProviderDocument8 pagesPharmacist As Primary Health Care ProviderRUTH AFUNWANo ratings yet
- Indian Public Health Standard IIDocument19 pagesIndian Public Health Standard IIKailash NagarNo ratings yet
- National Health MissionDocument70 pagesNational Health Missionprabha krishnanNo ratings yet
- Integration of Traditional Medicine and Allopathic Healthcare To Strengthen The Health System in MadagascarDocument23 pagesIntegration of Traditional Medicine and Allopathic Healthcare To Strengthen The Health System in MadagascarMiray RazanajatovoNo ratings yet
- Primary Health Care in IndiaDocument37 pagesPrimary Health Care in Indiadrsanjeev15No ratings yet
- Health Information System in Odisha An Evaluative Study of The Public Health Information Service Infrastructures For Rural Inhabitants of Balasore DistrictDocument4 pagesHealth Information System in Odisha An Evaluative Study of The Public Health Information Service Infrastructures For Rural Inhabitants of Balasore DistrictInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Community Health Nursing: Arby James Abonalla, RN, MSN, PHDN (C)Document237 pagesCommunity Health Nursing: Arby James Abonalla, RN, MSN, PHDN (C)Roshie Kaye AbalorioNo ratings yet
- Primary Health Care: Comprehensive First-Level CareDocument3 pagesPrimary Health Care: Comprehensive First-Level CareHannan AliNo ratings yet
- Health Care Delivery in IndiaDocument35 pagesHealth Care Delivery in IndiaKrishnaveni MurugeshNo ratings yet
- Palliative Care Under Ayushman Bharat Pradhan Mantri Jan Arogya Yojana (AB Pm-Jay)Document22 pagesPalliative Care Under Ayushman Bharat Pradhan Mantri Jan Arogya Yojana (AB Pm-Jay)mohit bhallaNo ratings yet
- Ayushman Bharat:: Comprehensive Primary Health Care Through Health and Wellness CentersDocument96 pagesAyushman Bharat:: Comprehensive Primary Health Care Through Health and Wellness CentersSiva SaranNo ratings yet
- Health and Family Welfare-Writeup - 0Document11 pagesHealth and Family Welfare-Writeup - 0Manpreet KaurNo ratings yet
- REVIEW OF NATIONAL HEALTH MISSION & SDGSDocument114 pagesREVIEW OF NATIONAL HEALTH MISSION & SDGSGargi pandeyNo ratings yet
- Ayushman Bharat: Comprehensive Primary Health CareDocument96 pagesAyushman Bharat: Comprehensive Primary Health CareAADITYESHWAR SINGH DEONo ratings yet
- Updated Indian Public Health Standards for Primary Health CentersDocument135 pagesUpdated Indian Public Health Standards for Primary Health CentersmanojvimalNo ratings yet
- National Rural Health MissionDocument37 pagesNational Rural Health MissionSanjeev SinghNo ratings yet
- India's Community Health Care Delivery SystemDocument39 pagesIndia's Community Health Care Delivery SystemangayarkanniNo ratings yet
- Essay-3 HealthcareDocument21 pagesEssay-3 HealthcareShretima AgrawalNo ratings yet
- 010 Primary Health CareDocument21 pages010 Primary Health CareMohd Amar Rahymee AnuarNo ratings yet
- Lecture 1 - History of Health Care Sys in MalaysiaDocument42 pagesLecture 1 - History of Health Care Sys in MalaysiaFatimah Azzahra KamarudinNo ratings yet
- Primary Health Care and ChipsDocument29 pagesPrimary Health Care and Chipsdorcas100% (1)
- Primary Health Care OverviewDocument58 pagesPrimary Health Care OverviewMjd ObiedNo ratings yet
- National Rural Health MissionDocument3 pagesNational Rural Health MissionAbhi PatelNo ratings yet
- National Rural Health MissionDocument3 pagesNational Rural Health Missionbasha trimuNo ratings yet
- Critical Review of NITIDocument5 pagesCritical Review of NITIPiyush SinghNo ratings yet
- Detailed Brief of NPHCEDocument6 pagesDetailed Brief of NPHCEMETALX 100No ratings yet
- Unit 1 Public Health: Definition and Concept: Dr. Rajesh Agrawal Associate Professor, MBICEMDocument15 pagesUnit 1 Public Health: Definition and Concept: Dr. Rajesh Agrawal Associate Professor, MBICEMshrutiNo ratings yet
- Public Health Sector by AbhishekDocument12 pagesPublic Health Sector by AbhishekfdxgfdgbfbhNo ratings yet
- 44-Article Text-775-1-10-20140406Document10 pages44-Article Text-775-1-10-20140406breastcancer.globaleventsNo ratings yet
- The Human Resource For Health Situation in Zambia: Deficit and MaldistributionDocument11 pagesThe Human Resource For Health Situation in Zambia: Deficit and MaldistributionChimbwe PhiriNo ratings yet
- NPCDCS Final Operational GuidelinesDocument78 pagesNPCDCS Final Operational GuidelinesTitiksha KannureNo ratings yet
- CHN Complete NotesDocument237 pagesCHN Complete NotesMelody B. Miguel100% (1)
- CHN 1health Care Delivery 3rd PartDocument40 pagesCHN 1health Care Delivery 3rd PartMicaNo ratings yet
- Community Health Nursing (Part 1)Document19 pagesCommunity Health Nursing (Part 1)bekbekk cabahugNo ratings yet
- Oral Health Care Delivery Systems in India An OverviewDocument8 pagesOral Health Care Delivery Systems in India An OverviewAparnaBNairNo ratings yet
- Chapter 6: Primary Health Care Learning ObjectivesDocument7 pagesChapter 6: Primary Health Care Learning ObjectivesLawrence Ryan DaugNo ratings yet
- Health Care Delivery Concerns in IndiaDocument43 pagesHealth Care Delivery Concerns in IndiaSaji Sadanandan50% (4)
- Framework On Integrated People Centred Health ServicesDocument12 pagesFramework On Integrated People Centred Health Servicesaperfectcircle7978No ratings yet
- Traditional and Complementary Medicine in Primary Health CareDocument16 pagesTraditional and Complementary Medicine in Primary Health CareNAYSHA LIZBETH ADCO HUARCAYANo ratings yet
- Primary Health Care (PHC)Document36 pagesPrimary Health Care (PHC)Shad Rahman100% (1)
- Public Health in IndiaDocument41 pagesPublic Health in Indiasachin parmarNo ratings yet
- National Health Policies and Community HealthcareDocument14 pagesNational Health Policies and Community Healthcareatharva sawantNo ratings yet
- Primary Health Care Awareness Faqs - 4Document3 pagesPrimary Health Care Awareness Faqs - 4billyelikanahNo ratings yet
- Aliaga National High School, Aliaga DistrictDocument55 pagesAliaga National High School, Aliaga DistrictSaira Dela Rosa MallariNo ratings yet
- Government Health Schemes for Marginalized Groups in MaharashtraDocument6 pagesGovernment Health Schemes for Marginalized Groups in MaharashtraRavindra BankarNo ratings yet
- Concept of PHCDocument43 pagesConcept of PHCVantrigaru Veeresh Bangi93% (14)
- Communicable DiseasesDocument24 pagesCommunicable DiseasesNur HamraNo ratings yet
- Public Health Nursing: Scope and Standards of PracticeFrom EverandPublic Health Nursing: Scope and Standards of PracticeRating: 5 out of 5 stars5/5 (1)
- An Analysis on Mental Health Issues among IndividualsDocument6 pagesAn Analysis on Mental Health Issues among IndividualsInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Harnessing Open Innovation for Translating Global Languages into Indian LanuagesDocument7 pagesHarnessing Open Innovation for Translating Global Languages into Indian LanuagesInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Diabetic Retinopathy Stage Detection Using CNN and Inception V3Document9 pagesDiabetic Retinopathy Stage Detection Using CNN and Inception V3International Journal of Innovative Science and Research TechnologyNo ratings yet
- Investigating Factors Influencing Employee Absenteeism: A Case Study of Secondary Schools in MuscatDocument16 pagesInvestigating Factors Influencing Employee Absenteeism: A Case Study of Secondary Schools in MuscatInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Exploring the Molecular Docking Interactions between the Polyherbal Formulation Ibadhychooranam and Human Aldose Reductase Enzyme as a Novel Approach for Investigating its Potential Efficacy in Management of CataractDocument7 pagesExploring the Molecular Docking Interactions between the Polyherbal Formulation Ibadhychooranam and Human Aldose Reductase Enzyme as a Novel Approach for Investigating its Potential Efficacy in Management of CataractInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- The Making of Object Recognition Eyeglasses for the Visually Impaired using Image AIDocument6 pagesThe Making of Object Recognition Eyeglasses for the Visually Impaired using Image AIInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- The Relationship between Teacher Reflective Practice and Students Engagement in the Public Elementary SchoolDocument31 pagesThe Relationship between Teacher Reflective Practice and Students Engagement in the Public Elementary SchoolInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Dense Wavelength Division Multiplexing (DWDM) in IT Networks: A Leap Beyond Synchronous Digital Hierarchy (SDH)Document2 pagesDense Wavelength Division Multiplexing (DWDM) in IT Networks: A Leap Beyond Synchronous Digital Hierarchy (SDH)International Journal of Innovative Science and Research TechnologyNo ratings yet
- Comparatively Design and Analyze Elevated Rectangular Water Reservoir with and without Bracing for Different Stagging HeightDocument4 pagesComparatively Design and Analyze Elevated Rectangular Water Reservoir with and without Bracing for Different Stagging HeightInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- The Impact of Digital Marketing Dimensions on Customer SatisfactionDocument6 pagesThe Impact of Digital Marketing Dimensions on Customer SatisfactionInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Electro-Optics Properties of Intact Cocoa Beans based on Near Infrared TechnologyDocument7 pagesElectro-Optics Properties of Intact Cocoa Beans based on Near Infrared TechnologyInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Formulation and Evaluation of Poly Herbal Body ScrubDocument6 pagesFormulation and Evaluation of Poly Herbal Body ScrubInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Advancing Healthcare Predictions: Harnessing Machine Learning for Accurate Health Index PrognosisDocument8 pagesAdvancing Healthcare Predictions: Harnessing Machine Learning for Accurate Health Index PrognosisInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- The Utilization of Date Palm (Phoenix dactylifera) Leaf Fiber as a Main Component in Making an Improvised Water FilterDocument11 pagesThe Utilization of Date Palm (Phoenix dactylifera) Leaf Fiber as a Main Component in Making an Improvised Water FilterInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Cyberbullying: Legal and Ethical Implications, Challenges and Opportunities for Policy DevelopmentDocument7 pagesCyberbullying: Legal and Ethical Implications, Challenges and Opportunities for Policy DevelopmentInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Auto Encoder Driven Hybrid Pipelines for Image Deblurring using NAFNETDocument6 pagesAuto Encoder Driven Hybrid Pipelines for Image Deblurring using NAFNETInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Terracing as an Old-Style Scheme of Soil Water Preservation in Djingliya-Mandara Mountains- CameroonDocument14 pagesTerracing as an Old-Style Scheme of Soil Water Preservation in Djingliya-Mandara Mountains- CameroonInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- A Survey of the Plastic Waste used in Paving BlocksDocument4 pagesA Survey of the Plastic Waste used in Paving BlocksInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Hepatic Portovenous Gas in a Young MaleDocument2 pagesHepatic Portovenous Gas in a Young MaleInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Design, Development and Evaluation of Methi-Shikakai Herbal ShampooDocument8 pagesDesign, Development and Evaluation of Methi-Shikakai Herbal ShampooInternational Journal of Innovative Science and Research Technology100% (3)
- Explorning the Role of Machine Learning in Enhancing Cloud SecurityDocument5 pagesExplorning the Role of Machine Learning in Enhancing Cloud SecurityInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- A Review: Pink Eye Outbreak in IndiaDocument3 pagesA Review: Pink Eye Outbreak in IndiaInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Automatic Power Factor ControllerDocument4 pagesAutomatic Power Factor ControllerInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Review of Biomechanics in Footwear Design and Development: An Exploration of Key Concepts and InnovationsDocument5 pagesReview of Biomechanics in Footwear Design and Development: An Exploration of Key Concepts and InnovationsInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Mobile Distractions among Adolescents: Impact on Learning in the Aftermath of COVID-19 in IndiaDocument2 pagesMobile Distractions among Adolescents: Impact on Learning in the Aftermath of COVID-19 in IndiaInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Studying the Situation and Proposing Some Basic Solutions to Improve Psychological Harmony Between Managerial Staff and Students of Medical Universities in Hanoi AreaDocument5 pagesStudying the Situation and Proposing Some Basic Solutions to Improve Psychological Harmony Between Managerial Staff and Students of Medical Universities in Hanoi AreaInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Navigating Digitalization: AHP Insights for SMEs' Strategic TransformationDocument11 pagesNavigating Digitalization: AHP Insights for SMEs' Strategic TransformationInternational Journal of Innovative Science and Research Technology100% (1)
- Drug Dosage Control System Using Reinforcement LearningDocument8 pagesDrug Dosage Control System Using Reinforcement LearningInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- The Effect of Time Variables as Predictors of Senior Secondary School Students' Mathematical Performance Department of Mathematics Education Freetown PolytechnicDocument7 pagesThe Effect of Time Variables as Predictors of Senior Secondary School Students' Mathematical Performance Department of Mathematics Education Freetown PolytechnicInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Formation of New Technology in Automated Highway System in Peripheral HighwayDocument6 pagesFormation of New Technology in Automated Highway System in Peripheral HighwayInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Excel ICU Logbook V1.6Document23 pagesExcel ICU Logbook V1.6aboshima739No ratings yet
- Gerund Infinitive Reduction 3Document1 pageGerund Infinitive Reduction 3Sefa KocaturkNo ratings yet
- Half Marathon Training Schedule in 12 WeeksDocument2 pagesHalf Marathon Training Schedule in 12 WeeksTose MomentNo ratings yet
- Golden Pearls of Gynecology and Obstetrics by DR Nadeem SHBDocument10 pagesGolden Pearls of Gynecology and Obstetrics by DR Nadeem SHBusamaNo ratings yet
- Neurologia Croatica CROCAD 2020Document96 pagesNeurologia Croatica CROCAD 2020Goran SimicNo ratings yet
- REVALIDA COMPRE HEMA2LAB MIXING STUDIES UnivSantoTomasDocument4 pagesREVALIDA COMPRE HEMA2LAB MIXING STUDIES UnivSantoTomasJemimah CainoyNo ratings yet
- IS1.14 Humidification Brochure INT Issue3 WebDocument24 pagesIS1.14 Humidification Brochure INT Issue3 WebHundalHarmanNo ratings yet
- Detailed Lesson Plan I. Objectives ProcedureDocument5 pagesDetailed Lesson Plan I. Objectives ProcedureAngelaNo ratings yet
- Model Analysis 1 / Orthodontic Courses by Indian Dental AcademyDocument36 pagesModel Analysis 1 / Orthodontic Courses by Indian Dental Academyindian dental academyNo ratings yet
- Spine TricksDocument345 pagesSpine Trickslacho124No ratings yet
- Name: Mendones, Aldritz John Class Code: NSTP 1 7005B Date Submitted: December 08, 2022Document3 pagesName: Mendones, Aldritz John Class Code: NSTP 1 7005B Date Submitted: December 08, 2022RenzNo ratings yet
- CHN - Community Health Nursing - Lecture 1 (Prelim)Document4 pagesCHN - Community Health Nursing - Lecture 1 (Prelim)Akasha FrostmourneNo ratings yet
- (ENG) Huntleigh-BD4000 - BrochureDocument4 pages(ENG) Huntleigh-BD4000 - BrochureValentina Giraldo BetancourtNo ratings yet
- Bai Tap On Kiem Tra 1 Tiet Lan 1 - Anh 10 (Moi)Document7 pagesBai Tap On Kiem Tra 1 Tiet Lan 1 - Anh 10 (Moi)Tú Tuyền LêNo ratings yet
- JFamCommunityMed262113-1349692 034456Document5 pagesJFamCommunityMed262113-1349692 034456Putri Zatalini SabilaNo ratings yet
- HA-RLE-WS # 6 Assessing PainDocument3 pagesHA-RLE-WS # 6 Assessing PainJULIE ANNE CORTEZNo ratings yet
- Internship Journal Week 4Document2 pagesInternship Journal Week 4api-609630655No ratings yet
- Work-Life BalanceDocument21 pagesWork-Life BalancePimpinit UdomsompongNo ratings yet
- Erik Erikson - Powerpoint .Educ 22Document47 pagesErik Erikson - Powerpoint .Educ 22gwendarleneNo ratings yet
- Technical Commentary Standard Plan B-10.20: For Catch Basin Type 2Document3 pagesTechnical Commentary Standard Plan B-10.20: For Catch Basin Type 2Sabina ShresthaNo ratings yet
- DDocument2 pagesDAstika Ulfah IzzatiNo ratings yet
- Study Protocol For A Randomized Controlled Trial To Test For Preventive Effects of Diabetic Foot Ulceration by Telemedicine That Includes Sensor-Equipped Insoles Combined With Photo DocumentationDocument12 pagesStudy Protocol For A Randomized Controlled Trial To Test For Preventive Effects of Diabetic Foot Ulceration by Telemedicine That Includes Sensor-Equipped Insoles Combined With Photo DocumentationAna GalvãoNo ratings yet
- Leadership That Get Results PPT (FINAL)Document11 pagesLeadership That Get Results PPT (FINAL)vicky gaikwadNo ratings yet
- Maslach Burnout Toolkit For Medical Personnel Intro SheetDocument1 pageMaslach Burnout Toolkit For Medical Personnel Intro SheetMyint ZuNo ratings yet
- CryogenicsDocument5 pagesCryogenicsapi-502533045No ratings yet
- Module 5 Lesson 2 - DiscoveriesDocument2 pagesModule 5 Lesson 2 - Discoveriesdeez nutsNo ratings yet
- Daily Pattern of Energy Distribution and Weight LossDocument6 pagesDaily Pattern of Energy Distribution and Weight LossAldehydeNo ratings yet
- Psychological AssessmentDocument46 pagesPsychological Assessmentyubarajbro9104No ratings yet
- Seminar ReportDocument31 pagesSeminar ReportBitNo ratings yet
- 2019 Clinical Performance of Direct Anterior Composite Restorations A Systematic Literature Review and Critical AppraisalDocument19 pages2019 Clinical Performance of Direct Anterior Composite Restorations A Systematic Literature Review and Critical Appraisalmaroun ghalebNo ratings yet