You might also like
- Pgi Manimtim - PFC MatrixDocument14 pagesPgi Manimtim - PFC MatrixKim Adarem Joy Manimtim100% (2)
- Final Assessment Soap NoteDocument13 pagesFinal Assessment Soap Noteapi-494643478100% (3)
- Speaking 35 SamplesDocument35 pagesSpeaking 35 SamplesJoanmanabat100% (5)
- Ophthalmology Q&A: Dry Eyes, Conjunctivitis, UveitisDocument29 pagesOphthalmology Q&A: Dry Eyes, Conjunctivitis, UveitisAdebisiNo ratings yet
- Evidence Based Oral MedicineDocument13 pagesEvidence Based Oral MedicineShantanu DixitNo ratings yet
- Module 4 PROBLEM ORIENTED MEDICAL RECORDDocument15 pagesModule 4 PROBLEM ORIENTED MEDICAL RECORDdarius bautistaNo ratings yet
- Branchial Arch SyndromesDocument7 pagesBranchial Arch SyndromesVita Dental PachucaNo ratings yet
- Palliative Care Billing 101Document47 pagesPalliative Care Billing 101mturchianoNo ratings yet
- 510 DiscussionsDocument10 pages510 DiscussionsMavokeNo ratings yet
- Anorexia Nervosa and Anorexic-Like Syndromes in A Population-Based Female Twin SampleDocument8 pagesAnorexia Nervosa and Anorexic-Like Syndromes in A Population-Based Female Twin SampleGianella Toro SánchezNo ratings yet
- At The Crossroads of Gout and Psoriatic Arthritis: "Psout"Document9 pagesAt The Crossroads of Gout and Psoriatic Arthritis: "Psout"ireneardianiNo ratings yet
- Host Modulation TherapyDocument65 pagesHost Modulation TherapyKassim OboghenaNo ratings yet
- Panoramic Radiographs: Technique & Anatomy Review: Continuing EducationDocument20 pagesPanoramic Radiographs: Technique & Anatomy Review: Continuing EducationRay AustraliaNo ratings yet
- Hemodynamic Disorders, Thrombosis, and Shock GWAIDocument102 pagesHemodynamic Disorders, Thrombosis, and Shock GWAIkavindukarunarathnaNo ratings yet
- Chapter Two Tissue InjuryDocument38 pagesChapter Two Tissue Injuryapi-19916399No ratings yet
- Drug Interaction 2Document65 pagesDrug Interaction 2alhader libraryNo ratings yet
- Strategy of The Netherlands in The Field of Rare DiseasesDocument20 pagesStrategy of The Netherlands in The Field of Rare DiseasesGehd JdifkNo ratings yet
- Micro Microbial Mechanisms of Pathogenicity NOTESDocument6 pagesMicro Microbial Mechanisms of Pathogenicity NOTESAriane NobleNo ratings yet
- 2015 - Corneal Abrasions and Corneal Foreign BodieDocument13 pages2015 - Corneal Abrasions and Corneal Foreign BodiePrasetya AnugrahNo ratings yet
- Healing of Oral WoundsDocument38 pagesHealing of Oral WoundsPuspa AdhikariNo ratings yet
- The Endodontic Complexity Assessment Tool - E-CAT - 2021Document11 pagesThe Endodontic Complexity Assessment Tool - E-CAT - 2021bogdimNo ratings yet
- Optical Properties of Human Tissue Thesis - Van Der ZeeDocument302 pagesOptical Properties of Human Tissue Thesis - Van Der Zeepiyush_kavirajNo ratings yet
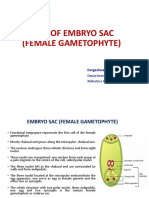
- Types of Embryo SacDocument18 pagesTypes of Embryo SacJemson Khundongbam100% (1)
- GCF FinalDocument76 pagesGCF FinalNishtha BaralNo ratings yet
- Immunology of CancerDocument48 pagesImmunology of CancerNovia Dwi AnggraeniNo ratings yet
- Basics of Light MicrosDocument55 pagesBasics of Light MicrosVivek AnandanNo ratings yet
- OSPE DU MedicineDocument101 pagesOSPE DU MedicinesaifNo ratings yet
- LSM3233 Lecture 1Document43 pagesLSM3233 Lecture 1Prab NathanNo ratings yet
- Princess File - 8 & 10 MarchDocument46 pagesPrincess File - 8 & 10 MarchShawqi ANo ratings yet
- Otomycosis in Western Iran: Clinical and Mycological AspectsDocument5 pagesOtomycosis in Western Iran: Clinical and Mycological AspectsLiz TorresNo ratings yet
- ByssinosisAsbestosis SilicosisDocument44 pagesByssinosisAsbestosis SilicosisMARK ARQUE LACANARIANo ratings yet
- TLR: Toll-Like Receptors Detect PathogensDocument46 pagesTLR: Toll-Like Receptors Detect PathogensHeru HanantoNo ratings yet
- The Information About EDSDocument3 pagesThe Information About EDSAmber100% (1)
- Metabolic Bone DiseaseDocument41 pagesMetabolic Bone DiseaseVenerandaNo ratings yet
- Biotherapy Approaches and Major AgentsDocument33 pagesBiotherapy Approaches and Major AgentsVILLEJO JHOVIALENNo ratings yet
- History Hassan Karar LongDocument125 pagesHistory Hassan Karar LongHamidHassanNo ratings yet
- New Horizons in Osteoporosis Management: Yasser El MiedanyDocument903 pagesNew Horizons in Osteoporosis Management: Yasser El Miedanyglennys carelaNo ratings yet
- Basidiomycota: Characteristics of Club Fungi and Important Rust and Smut DiseasesDocument63 pagesBasidiomycota: Characteristics of Club Fungi and Important Rust and Smut Diseasesmohanapriya.raNo ratings yet
- Giant Cell LesionsDocument33 pagesGiant Cell Lesionslakshmi k sNo ratings yet
- Progressive Myoclonic Epilepsies - Practical Neurology 2015. MalekDocument8 pagesProgressive Myoclonic Epilepsies - Practical Neurology 2015. MalekchintanNo ratings yet
- Renaissance Physicians Guide to Facial Beauty MaximizationDocument31 pagesRenaissance Physicians Guide to Facial Beauty MaximizationKentVilandkaNo ratings yet
- CONNECTIVE TISSUE LEC WEEK 4Document5 pagesCONNECTIVE TISSUE LEC WEEK 4Abigrael TangcoNo ratings yet
- Hansens DiseaseDocument83 pagesHansens DiseaseSajin AlexanderNo ratings yet
- Asteroid HyalosisDocument1 pageAsteroid HyalosishitriscNo ratings yet
- Developmental DisturbanceDocument50 pagesDevelopmental DisturbanceMSH100% (1)
- BotanyDocument98 pagesBotanyMikhail LandichoNo ratings yet
- HEMA LAB QUIZDocument31 pagesHEMA LAB QUIZAngela ReyesNo ratings yet
- Pathology Questions on Infant and Childhood DiseasesDocument6 pagesPathology Questions on Infant and Childhood DiseasesAdrian CaballesNo ratings yet
- OSCE Notes in OtolaryngologyDocument95 pagesOSCE Notes in OtolaryngologyTrial kalley100% (1)
- 40 Mitral Valve and Left Atrial LesionsDocument18 pages40 Mitral Valve and Left Atrial LesionsVictor PazNo ratings yet
- Kuliah EmergensiDocument66 pagesKuliah EmergensiRifqi RamdhaniNo ratings yet
- Histology Slides Made EasyDocument122 pagesHistology Slides Made EasyNour-alhuda Alsheriadah100% (1)
- Comparative Evaluation of Serum High Sensitivity CDocument9 pagesComparative Evaluation of Serum High Sensitivity Catif nawazNo ratings yet
- CEMENTUMDocument80 pagesCEMENTUMReshmaa RajendranNo ratings yet
- Syllabus of Bio-Informatics, PUCCDocument14 pagesSyllabus of Bio-Informatics, PUCCMd MohiuddinNo ratings yet
- Introduction To HistologyDocument32 pagesIntroduction To HistologyPushparaj ShettyNo ratings yet
- Dev Dis ToothDocument92 pagesDev Dis ToothVaishnavi ThatiparthiNo ratings yet
- Cellular Injury, Adaptation and Cellular DeathDocument40 pagesCellular Injury, Adaptation and Cellular DeathSuleiman KikulweNo ratings yet
- Imaging of Musculoskeletal SystemDocument53 pagesImaging of Musculoskeletal SystemSara ManzoorNo ratings yet
- Joints TransesDocument19 pagesJoints TransesskidamarinkNo ratings yet
- Crispr TechniqueDocument16 pagesCrispr TechniqueAmmar Abbas100% (1)
- Vox Sanguin Januari 2021Document139 pagesVox Sanguin Januari 2021rsdarsono labNo ratings yet
- Classification and Treatment of Zygomatic FracturesDocument13 pagesClassification and Treatment of Zygomatic FracturesJeane SuyantoNo ratings yet
- Thetrigeminalnerve Injury: Arshad Kaleem,, Paul Amailuk,, Hisham Hatoum,, Ramzey TursunDocument13 pagesThetrigeminalnerve Injury: Arshad Kaleem,, Paul Amailuk,, Hisham Hatoum,, Ramzey TursunPriyanka SinhaNo ratings yet
- Mycobacteria Slides For Lecture 2021Document70 pagesMycobacteria Slides For Lecture 2021wildoNo ratings yet
- Macleods Clinical Examination 14 EdDocument402 pagesMacleods Clinical Examination 14 Edrasulkhdhir7No ratings yet
- Introduction To General Pathology, Cell InjuryDocument69 pagesIntroduction To General Pathology, Cell InjuryRogony KibetNo ratings yet
- Patient Based PathophysiologyDocument3 pagesPatient Based PathophysiologyJeizel IgnacioNo ratings yet
- Wilson Disease in Children and Young Adults - State of The ArtDocument11 pagesWilson Disease in Children and Young Adults - State of The ArtJosueNo ratings yet
- Obstructive Diseases Cheat SheetDocument5 pagesObstructive Diseases Cheat SheetWiz SamNo ratings yet
- Branches and concepts of pharmacologyDocument15 pagesBranches and concepts of pharmacologyZaira Reine SantosNo ratings yet
- New Laboratory TestsDocument35 pagesNew Laboratory TestsCar SadNo ratings yet
- Mitral Stenosis: Ahmad AdityawarmanDocument81 pagesMitral Stenosis: Ahmad AdityawarmanAhmad AdityawarmanNo ratings yet
- Epi EstimDocument42 pagesEpi EstimBlvcklistNo ratings yet
- Generalized Anxiety DisorderDocument22 pagesGeneralized Anxiety DisorderAsqa KhanNo ratings yet
- Health Information & Basic Medical StatisticsDocument65 pagesHealth Information & Basic Medical StatisticsSaiNo ratings yet
- Chapter08 PDFDocument30 pagesChapter08 PDFEnfermeriaAncamNo ratings yet
- Cor Jesu College, Inc., College of Health Sciences Sto. Rosario, Tres de Mayo, Digos CityDocument6 pagesCor Jesu College, Inc., College of Health Sciences Sto. Rosario, Tres de Mayo, Digos City2BGrp3Plaza, Anna MaeNo ratings yet
- Kaposi SarcomaDocument11 pagesKaposi Sarcomaedgar mandengNo ratings yet
- The Influenza & Parainfluenza VirusesDocument35 pagesThe Influenza & Parainfluenza VirusesRoy D RogerNo ratings yet
- Anemia at Older AgeDocument10 pagesAnemia at Older AgeAbdullah ZuhairNo ratings yet
- Name of Drug Dosage, Route, Frequency and Timing Mechanism of Action Indication Adverse Reactions Special Precautions Nursing ResponsibilitiesDocument2 pagesName of Drug Dosage, Route, Frequency and Timing Mechanism of Action Indication Adverse Reactions Special Precautions Nursing ResponsibilitiesKarl Lourenz DeysolongNo ratings yet
- Krok 19 20 21 - CompressedDocument148 pagesKrok 19 20 21 - CompressedPaulNo ratings yet
- Health-Related Quality of Life ScaleDocument4 pagesHealth-Related Quality of Life ScaleMihaela Cosmina NiculescuNo ratings yet
- Epidemiology of Attention Deficit HyperaDocument7 pagesEpidemiology of Attention Deficit HyperaJessica WathierNo ratings yet
- 11 ImmunityDocument5 pages11 ImmunityTina EtoileNo ratings yet
- A Terrible Price' - The Deadly Racial Disparities of Covid-19 in America - The New York TimesDocument14 pagesA Terrible Price' - The Deadly Racial Disparities of Covid-19 in America - The New York TimesJavier BassiNo ratings yet
- 4.3 - Educating Patients, Family, and Health Care Professionals About Foot CareDocument1 page4.3 - Educating Patients, Family, and Health Care Professionals About Foot CareEva Cica SusantiNo ratings yet
- PGI Sarip - Covid 19Document92 pagesPGI Sarip - Covid 19Junayyah Abdullah SaripNo ratings yet
- Disturbances in DigestionDocument2 pagesDisturbances in DigestionAnabelle RicoNo ratings yet