You might also like
- Laryngopharyngeal and Gastroesophageal Reflux: A Comprehensive Guide to Diagnosis, Treatment, and Diet-Based ApproachesFrom EverandLaryngopharyngeal and Gastroesophageal Reflux: A Comprehensive Guide to Diagnosis, Treatment, and Diet-Based ApproachesCraig H. ZalvanNo ratings yet
- The Prevention and Treatment of Disease with a Plant-Based Diet Volume 2: Evidence-based articles to guide the physicianFrom EverandThe Prevention and Treatment of Disease with a Plant-Based Diet Volume 2: Evidence-based articles to guide the physicianNo ratings yet
- Functional Dyspepsia: Advances in Diagnosis and Therapy: ReviewDocument9 pagesFunctional Dyspepsia: Advances in Diagnosis and Therapy: Reviewjenny puentesNo ratings yet
- Organic Versus Functional: DyspepsiaDocument16 pagesOrganic Versus Functional: DyspepsiahelenaNo ratings yet
- CTC Gerd FinalDocument36 pagesCTC Gerd FinaljaipreyraNo ratings yet
- Functional DyspepsiaDocument4 pagesFunctional DyspepsiaEasy Orient DewantariNo ratings yet
- Kasar Pkmrs BBBDocument5 pagesKasar Pkmrs BBBIriamana Liasyarah MarudinNo ratings yet
- Robinson 2016Document20 pagesRobinson 2016sadiqNo ratings yet
- Update On The Evaluation and Management of Functional DyspepsiaDocument7 pagesUpdate On The Evaluation and Management of Functional DyspepsiaDenuna EnjanaNo ratings yet
- Current Diagnosis and Management of Suspected Reflux Symptoms Refractory to PPI TherapyDocument9 pagesCurrent Diagnosis and Management of Suspected Reflux Symptoms Refractory to PPI TherapyMuhammad Wim AdhitamaNo ratings yet
- Increasing Awareness of Gastro-Esophageal Reflux Disease in Adult Patients at A Primary Care Clinic 1Document16 pagesIncreasing Awareness of Gastro-Esophageal Reflux Disease in Adult Patients at A Primary Care Clinic 1TinaHoNo ratings yet
- Camille Ri 2012Document20 pagesCamille Ri 2012Jose Lopez FuentesNo ratings yet
- William, Update On Approaches To Patients With Dyspepsia and Functional DyspepsiaDocument6 pagesWilliam, Update On Approaches To Patients With Dyspepsia and Functional DyspepsiaRevalitha PutriNo ratings yet
- Research Article: Low Prevalence of Clinically Significant Endoscopic Findings in Outpatients With DyspepsiaDocument7 pagesResearch Article: Low Prevalence of Clinically Significant Endoscopic Findings in Outpatients With DyspepsiaKurnia pralisaNo ratings yet
- DyspepsiaDocument7 pagesDyspepsiaFa'iz HeryotoNo ratings yet
- Irritable Bowel Syndrome and Other Functional Gastrointestinal DisordersDocument3 pagesIrritable Bowel Syndrome and Other Functional Gastrointestinal DisordersdavpierNo ratings yet
- Ajg 2012 Gastroparesis, Management of PDFDocument20 pagesAjg 2012 Gastroparesis, Management of PDFrisewfNo ratings yet
- Algoritma GerdDocument14 pagesAlgoritma GerdRivaldi ArdiansyahNo ratings yet
- Gastroesophageal Reflux Disease Control of Symptoms, Prevention of ComplicationsDocument9 pagesGastroesophageal Reflux Disease Control of Symptoms, Prevention of ComplicationsTiurma SibaraniNo ratings yet
- Changing Trends in Peptic Ulcer Prevalence in A Tertiary Care Setting in The PhilippinesDocument3 pagesChanging Trends in Peptic Ulcer Prevalence in A Tertiary Care Setting in The PhilippinesRumelle ReyesNo ratings yet
- Diagnosis and Management of Functional HeartburnDocument9 pagesDiagnosis and Management of Functional Heartburnal ghiffari muhammad rayhanNo ratings yet
- Review: Epidemiology, Mechanisms, and Management of Diabetic GastroparesisDocument8 pagesReview: Epidemiology, Mechanisms, and Management of Diabetic GastroparesisIrma KurniawatiNo ratings yet
- Richter 2017Document10 pagesRichter 2017Rachel RiosNo ratings yet
- Review Article Helicobacter Pylori Infection: Dyspepsia: When and How To Test ForDocument10 pagesReview Article Helicobacter Pylori Infection: Dyspepsia: When and How To Test ForAyu Trisna PutriNo ratings yet
- Clinical Review: DyspepsiaDocument5 pagesClinical Review: Dyspepsiajenny puentesNo ratings yet
- Gastrointestinal Disorders in DiabetesDocument20 pagesGastrointestinal Disorders in Diabetesdoctor327810No ratings yet
- Gastroesophagean Reflux DiseaseDocument13 pagesGastroesophagean Reflux Diseasedenisa malinaNo ratings yet
- Erge NejmDocument10 pagesErge Nejmliz salcedoNo ratings yet
- Chronic Dyspepsia GuidelineDocument8 pagesChronic Dyspepsia Guidelinenainggolan Debora15No ratings yet
- GI & Hepatobiliary Disorders DiscussionDocument4 pagesGI & Hepatobiliary Disorders DiscussionDaniel “Riungi” MbaabuNo ratings yet
- Nejmcp 2114026Document10 pagesNejmcp 2114026Engin AltınkayaNo ratings yet
- Hubungan Pola Makan Terhadap Kejadian Dispepsia Di RSUD Meuraxa Kota Banda AcehDocument8 pagesHubungan Pola Makan Terhadap Kejadian Dispepsia Di RSUD Meuraxa Kota Banda AcehjustisiaNo ratings yet
- Nejmcp 2114026Document10 pagesNejmcp 2114026Cristina Adriana PopaNo ratings yet
- The Clinical Management of Gastroesophageal Reflux DiseaseDocument12 pagesThe Clinical Management of Gastroesophageal Reflux DiseaseMahmoud SamiNo ratings yet
- Recurrent Abdominal Pain: C.H. SprayDocument5 pagesRecurrent Abdominal Pain: C.H. SprayVilarTdNo ratings yet
- Laporan Jaga DispepsiaDocument4 pagesLaporan Jaga DispepsiaTeguh YukiNo ratings yet
- Functional Dyspepsia: Review ArticleDocument11 pagesFunctional Dyspepsia: Review Articlejenny puentesNo ratings yet
- Functional Dyspepsia Review: Symptoms, Evaluation, TreatmentDocument9 pagesFunctional Dyspepsia Review: Symptoms, Evaluation, TreatmentMarsya Yulinesia LoppiesNo ratings yet
- Referensi 1 PDFDocument4 pagesReferensi 1 PDFYusmiatiNo ratings yet
- 1 Problemas de Motilidad GIDocument13 pages1 Problemas de Motilidad GIFlor De LotoNo ratings yet
- Pathophysiology of Functional Dyspepsia: ReviewDocument6 pagesPathophysiology of Functional Dyspepsia: ReviewTobi JulfiartoNo ratings yet
- Dyspepsia PDFDocument14 pagesDyspepsia PDFCdma Nastiti FatimahNo ratings yet
- Refeeding Syndrome: Practice GapDocument10 pagesRefeeding Syndrome: Practice GapEva AstriaNo ratings yet
- Ibs JurnalDocument11 pagesIbs JurnalimuhammadfahmiNo ratings yet
- Pilichiewicz 2009Document6 pagesPilichiewicz 2009Stella KwanNo ratings yet
- The Management of Polycystic Ovary Syndrome: Vincenza Bruni, Metella Dei, Valentina Pontello, and Paolo VangelistiDocument15 pagesThe Management of Polycystic Ovary Syndrome: Vincenza Bruni, Metella Dei, Valentina Pontello, and Paolo VangelistiDaniela UrreaNo ratings yet
- New Articles in This Journal Are Licensed Under A Creative Commons Attribution 4.0 United States LicenseDocument16 pagesNew Articles in This Journal Are Licensed Under A Creative Commons Attribution 4.0 United States Licenseandi hajrahNo ratings yet
- Plenary 2B Group 13Document132 pagesPlenary 2B Group 13Obet Agung 天No ratings yet
- Dyspepsia ReviewDocument13 pagesDyspepsia ReviewalbertrianthoNo ratings yet
- Diet IBS PDFDocument31 pagesDiet IBS PDFIesanu MaraNo ratings yet
- Zreflujo en Gestación 2008Document14 pagesZreflujo en Gestación 2008j hdezNo ratings yet
- Case File GERDDocument9 pagesCase File GERDMutiara Shifa100% (1)
- The Diagnosis and Treatment of Functional DyspepsiaDocument20 pagesThe Diagnosis and Treatment of Functional Dyspepsia• Ridlo FebriansyahNonPrivacyNo ratings yet
- Aliment Pharmacol Ther - 2004 - ChangDocument9 pagesAliment Pharmacol Ther - 2004 - ChangCynthia SuarezNo ratings yet
- 2359 3yf997 Aem 59 2 0129 - 2Document8 pages2359 3yf997 Aem 59 2 0129 - 2Muhammad Wim AdhitamaNo ratings yet
- Approach To Uninvestigated DyspepsiaDocument18 pagesApproach To Uninvestigated DyspepsiaAshish SatyalNo ratings yet
- PCOS and Metabolic SyndromeDocument21 pagesPCOS and Metabolic SyndromeHAVIZ YUADNo ratings yet
- 8 Nausea and Vomiting, Diarrhea, Constipation (Pedrosa)Document27 pages8 Nausea and Vomiting, Diarrhea, Constipation (Pedrosa)JEHAN HADJIUSMANNo ratings yet
- Pathophysiology of Functional Dyspepsia: ReviewDocument6 pagesPathophysiology of Functional Dyspepsia: ReviewRaisa AlifiaNo ratings yet
- ACG Guideline GERD March 2013Document21 pagesACG Guideline GERD March 2013Arri KurniawanNo ratings yet
- An Tibi OtikDocument11 pagesAn Tibi Otiknainggolan Debora15No ratings yet
- Managing dyspepsia with declining H. pyloriDocument71 pagesManaging dyspepsia with declining H. pylorinainggolan Debora15No ratings yet
- Dyspepsia AIPDocument6 pagesDyspepsia AIPIulia NiculaeNo ratings yet
- GatroDocument48 pagesGatronainggolan Debora15No ratings yet
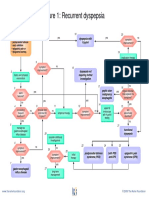
- Recurrent DyspepsiaDocument10 pagesRecurrent Dyspepsianainggolan Debora15No ratings yet
- Irritable Bowel Syndrome: Risk FactorsDocument2 pagesIrritable Bowel Syndrome: Risk Factorsnainggolan Debora15No ratings yet
- Chronic Dyspepsia GuidelineDocument8 pagesChronic Dyspepsia Guidelinenainggolan Debora15No ratings yet
- Manajemen DipepsiaDocument154 pagesManajemen Dipepsianainggolan Debora15No ratings yet
- DispepsiaDocument3 pagesDispepsianainggolan Debora15No ratings yet
- Guillain Barre 3Document6 pagesGuillain Barre 3YON LEANDRO VILLAMIL ROJASNo ratings yet
- Barney's Great Adventure - Barney Wiki - WikiaDocument2 pagesBarney's Great Adventure - Barney Wiki - WikiachefchadsmithNo ratings yet
- Owner S Manual Subaru LegacyDocument20 pagesOwner S Manual Subaru LegacyLexBgNo ratings yet
- Encore 700 Diaphragm Pump 1Document12 pagesEncore 700 Diaphragm Pump 1bagurtoNo ratings yet
- 9701 w09 QP 41Document20 pages9701 w09 QP 41Hubbak KhanNo ratings yet
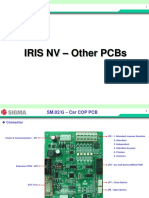
- 07 IRIS NV PCB OtherDocument15 pages07 IRIS NV PCB OtherArnaldo cordovaNo ratings yet
- Fit For WashingDocument85 pagesFit For WashingIyaka YoeNo ratings yet
- Astm D2467-2013Document8 pagesAstm D2467-2013Renato CorrêaNo ratings yet
- Chap 5. Beam Analysis and Design PDFDocument61 pagesChap 5. Beam Analysis and Design PDFRafael Joshua LedesmaNo ratings yet
- Postmodern EthicsDocument1 pagePostmodern Ethicsgeorge elerickNo ratings yet
- Textiles and Clothing SustaninabilityDocument134 pagesTextiles and Clothing Sustaninabilitydike100% (1)
- SPC英文版教材Document83 pagesSPC英文版教材bing cai100% (2)
- Giddings & Lewis Sect08 HydDocument24 pagesGiddings & Lewis Sect08 HydAngel AdautaNo ratings yet
- OrlDocument186 pagesOrlMuli MaroshiNo ratings yet
- Permeability Test Constant Head MethodDocument10 pagesPermeability Test Constant Head MethodLouise LuyNo ratings yet
- Interpuls Novinki 2014Document64 pagesInterpuls Novinki 2014BaklanovaSVNo ratings yet
- Sponge BobDocument4 pagesSponge BobchabriesNo ratings yet
- IQ 250/260 Transducer Quick Start GuideDocument2 pagesIQ 250/260 Transducer Quick Start GuideJoséEmmanuelCasasMunguíaNo ratings yet
- Pneumatic Pruning Equipment American Arborist Supplies, Tree Care, Climbing EquipmentDocument1 pagePneumatic Pruning Equipment American Arborist Supplies, Tree Care, Climbing EquipmentSalman JoNo ratings yet
- Gen Ed Answer Key (A)Document7 pagesGen Ed Answer Key (A)Antonette Escarpe TorcinoNo ratings yet
- 1992SGSDesignersGuidetoPowerProductsApplicationManual2Ed 1182713547Document1,298 pages1992SGSDesignersGuidetoPowerProductsApplicationManual2Ed 1182713547analog changeNo ratings yet
- Essay - DnaDocument2 pagesEssay - Dnaapi-243852896No ratings yet
- Simulation of bitumen upgrading processes modelling and optimisationDocument6 pagesSimulation of bitumen upgrading processes modelling and optimisationDonato MontroneNo ratings yet
- Understanding The Nature of ReligionDocument41 pagesUnderstanding The Nature of Religioneden l. abadNo ratings yet
- RCS England Trainees Guide To A Quality Improvement Project 2021Document17 pagesRCS England Trainees Guide To A Quality Improvement Project 2021Wee K WeiNo ratings yet
- Jigoku Shoujo Eikyuu No SonzaiDocument166 pagesJigoku Shoujo Eikyuu No Sonzaiapi-224188021No ratings yet
- Spesifikasi Siemens MRI AERA 1,5 TDocument2 pagesSpesifikasi Siemens MRI AERA 1,5 TDr.gendjutNo ratings yet
- Mechatronics Test Questions Set - 1Document13 pagesMechatronics Test Questions Set - 1ChippyVijayanNo ratings yet
- Preliminary Evaluation On Vegetative of Rambutan (Nephelium Lappaceum) in Sandy Tin-Tailing SoilDocument7 pagesPreliminary Evaluation On Vegetative of Rambutan (Nephelium Lappaceum) in Sandy Tin-Tailing SoilAJAST JournalNo ratings yet
- Cheese Yoghurt and Ripening Cultures Reference Chart May 2020Document7 pagesCheese Yoghurt and Ripening Cultures Reference Chart May 2020AbitNo ratings yet