You might also like
- Articol 2Document6 pagesArticol 2Silviu Iulian FilipiucNo ratings yet
- ECG Scoring For The Evaluation of Therapy Naive Cancer Patients To Predict CardiotoxicityDocument11 pagesECG Scoring For The Evaluation of Therapy Naive Cancer Patients To Predict CardiotoxicityjuanpbagurNo ratings yet
- Structural and Functional Cardiac Changes in Myotonic Dystrophy Type 1: A Cardiovascular Magnetic Resonance StudyDocument7 pagesStructural and Functional Cardiac Changes in Myotonic Dystrophy Type 1: A Cardiovascular Magnetic Resonance StudyRhirin JiehhNo ratings yet
- Takutsubo SyndromeDocument17 pagesTakutsubo Syndromerizqina ajraNo ratings yet
- Manual Aspiration Thrombectomy in Acute Myocardial Infarction: A Clinical ExperienceDocument9 pagesManual Aspiration Thrombectomy in Acute Myocardial Infarction: A Clinical ExperienceArdiana FirdausNo ratings yet
- Heart 2Document10 pagesHeart 2Nag Mallesh RaoNo ratings yet
- Joa3 12534Document7 pagesJoa3 12534chasia chaselNo ratings yet
- Cetin 2016Document10 pagesCetin 2016Della Puspita SariNo ratings yet
- Biomarker Discovery in Cardio-Oncology.Document8 pagesBiomarker Discovery in Cardio-Oncology.Ștefan SpînuNo ratings yet
- 1 s2.0 S1083879111002916 MainDocument8 pages1 s2.0 S1083879111002916 MainNunungTriwahyuniNo ratings yet
- Ni Hms 725829Document19 pagesNi Hms 725829SabariaNo ratings yet
- Mri and Serum High Sensitivity C Reactive Protein Predict Long Term Mortality in Non Ischaemic CardiomyopathyDocument9 pagesMri and Serum High Sensitivity C Reactive Protein Predict Long Term Mortality in Non Ischaemic Cardiomyopathyingrid da silvaNo ratings yet
- hr2008109 PDFDocument10 pageshr2008109 PDFKumarsai DurusojuNo ratings yet
- Cardiotoxicidad en CáncerDocument11 pagesCardiotoxicidad en CáncerMIGUEL MORENONo ratings yet
- Impact of Optimal Medical Therapy On 10-Year Mortality After Coronary RevascularizationDocument12 pagesImpact of Optimal Medical Therapy On 10-Year Mortality After Coronary RevascularizationsarahNo ratings yet
- Thesis Acute Coronary SyndromeDocument8 pagesThesis Acute Coronary Syndromeaflpcdwfunzfed100% (2)
- Cardiac Troponins For The Diagnosis of Acute Myocardial Infarction in Chronic Kidney Disease PDFDocument24 pagesCardiac Troponins For The Diagnosis of Acute Myocardial Infarction in Chronic Kidney Disease PDFDaniel Hernando Rodriguez PeraltaNo ratings yet
- Jurnal 1Document10 pagesJurnal 1fitri juliantiNo ratings yet
- Long-Term Survival in Patients With Non-Small Cell Lung CancerDocument7 pagesLong-Term Survival in Patients With Non-Small Cell Lung CancerMrBuu2012No ratings yet
- Jurnal 2 FikriDocument36 pagesJurnal 2 FikriwarptenNo ratings yet
- The Year in Cardiology 2015Document13 pagesThe Year in Cardiology 2015SyafniYuliaSistriNo ratings yet
- Role of Exercise Treadmill Testing in The Assessment of Coronary Microvascular Disease - LopezDocument10 pagesRole of Exercise Treadmill Testing in The Assessment of Coronary Microvascular Disease - LopezM. PurnomoNo ratings yet
- Stenoza MitralaDocument7 pagesStenoza MitralaVerginia OnofreiNo ratings yet
- Factores para FNRDocument10 pagesFactores para FNRPOMYNo ratings yet
- Eht 104Document9 pagesEht 104MAX ANTHONY SALAMANCA HILASACANo ratings yet
- Clinchem 2013 203778 FullDocument9 pagesClinchem 2013 203778 FullHarnadi WonogiriNo ratings yet
- Madit CRTNEJMseot 09Document10 pagesMadit CRTNEJMseot 09binh doNo ratings yet
- Dogan 2012Document7 pagesDogan 2012Davy JonesNo ratings yet
- Native t1 MappingDocument10 pagesNative t1 MappingRaiyanNo ratings yet
- Fmed 09 799310Document4 pagesFmed 09 799310Chris Chavez CollazosNo ratings yet
- Optimal Medical Therapy vs. Percutaneous Coronary Intervention For Patients With Coronary Chronic Total OcclusionDocument7 pagesOptimal Medical Therapy vs. Percutaneous Coronary Intervention For Patients With Coronary Chronic Total OcclusionsarahNo ratings yet
- Biomedicines 10 02407 v2Document13 pagesBiomedicines 10 02407 v2akinaNo ratings yet
- BSC Summary 2018 ESC GuidelinesDocument11 pagesBSC Summary 2018 ESC GuidelinesHesbon MomanyiNo ratings yet
- Left Ventricular Dysfunction Predicted by Early Troponin I Release After High-Dose ChemotherapyDocument6 pagesLeft Ventricular Dysfunction Predicted by Early Troponin I Release After High-Dose ChemotherapydeyaNo ratings yet
- Ijcc 4 098Document9 pagesIjcc 4 098ASIK1144No ratings yet
- Detection of Myocardial Infraction Monisha C M - 17bei0092: Select, Vit VelloreDocument8 pagesDetection of Myocardial Infraction Monisha C M - 17bei0092: Select, Vit VelloresubramanianNo ratings yet
- AINES e Clinical OutcomesDocument23 pagesAINES e Clinical Outcomesdiogofc123No ratings yet
- Tumor Necrosis Factor Inhibitors in Patients With Takayasu Arteritis: Experience From A Referral Center With Long-Term FollowupDocument5 pagesTumor Necrosis Factor Inhibitors in Patients With Takayasu Arteritis: Experience From A Referral Center With Long-Term FollowupMikhail PisarevNo ratings yet
- CTperfusion TeoreticDocument7 pagesCTperfusion TeoreticarthaaaaaNo ratings yet
- Diagnostics: Cardiac Resynchronization Therapy in Non-Ischemic Cardiomyopathy: Role of Multimodality ImagingDocument15 pagesDiagnostics: Cardiac Resynchronization Therapy in Non-Ischemic Cardiomyopathy: Role of Multimodality Imagingmarsim92No ratings yet
- Qualitative and Quantitative Comparison of Tgrappa and Tsense Real Time Cine Techniques During Deep BreathingDocument316 pagesQualitative and Quantitative Comparison of Tgrappa and Tsense Real Time Cine Techniques During Deep BreathingRadhaRajasekaranNo ratings yet
- Pi Is 0002870312001767Document9 pagesPi Is 0002870312001767Carlos Delgado AchiNo ratings yet
- Varma - Cardio Oncology SM121917Document12 pagesVarma - Cardio Oncology SM121917Gabriela Araya MedranoNo ratings yet
- ESCAPE Study - JAMA 2005Document9 pagesESCAPE Study - JAMA 2005MICHAEL AMARILLO CORREANo ratings yet
- Essential Guide to Diagnosing and Treating Ischemic StrokeDocument21 pagesEssential Guide to Diagnosing and Treating Ischemic Strokekuchaibaru90No ratings yet
- Biomarkers in Acute Coronary SyndromesDocument29 pagesBiomarkers in Acute Coronary SyndromesCatherine MorrisNo ratings yet
- Correlation of Systemic Inflammatory Status & Cardiac Myonecrosis in Patients Undergoing Percutaneoues Coronary InterventionDocument76 pagesCorrelation of Systemic Inflammatory Status & Cardiac Myonecrosis in Patients Undergoing Percutaneoues Coronary InterventionHusna AhamedNo ratings yet
- DIABreinstadler2017 17Document28 pagesDIABreinstadler2017 17marsim92No ratings yet
- 2013 - STEMI - Future Strategies - LancetDocument14 pages2013 - STEMI - Future Strategies - LancetMichail PapafaklisNo ratings yet
- International Journal of Neurology and Neurotherapy Ijnn 2 030Document2 pagesInternational Journal of Neurology and Neurotherapy Ijnn 2 030Anis Rita PratiwiNo ratings yet
- MINOCA STEMI Manuscript 0Document19 pagesMINOCA STEMI Manuscript 0wellaNo ratings yet
- Bu Wiwin 1cDocument6 pagesBu Wiwin 1cDinny Fitriani FullNo ratings yet
- Diab 6Document6 pagesDiab 6marsim92No ratings yet
- RRC Art-2Document16 pagesRRC Art-2TanyaDonciuNo ratings yet
- TilemahDocument7 pagesTilemahAndreea TudurachiNo ratings yet
- Anthracycline and Trastuzumab-Induced Cardiotoxicity in Breast CancerDocument11 pagesAnthracycline and Trastuzumab-Induced Cardiotoxicity in Breast CancertaniasolisNo ratings yet
- EMPA REG OUTCOME The Cardiologist S Point 2017 The American Journal of MedDocument6 pagesEMPA REG OUTCOME The Cardiologist S Point 2017 The American Journal of MedAlina PopaNo ratings yet
- Increasingly Sensitive Assays For Cardiac TroponinsDocument8 pagesIncreasingly Sensitive Assays For Cardiac TroponinsAbel Espinoza MedallaNo ratings yet
- Cancer Therapy-Induced Cardiotoxicity-A Metabolic Perspective On Pathogenesis, Diagnosis and TherapyDocument19 pagesCancer Therapy-Induced Cardiotoxicity-A Metabolic Perspective On Pathogenesis, Diagnosis and TherapyIsabelle ParahybaNo ratings yet
- 2.nam Et Al-2021-Retrospective Obs-Clinical Impact of BP Variability in Covid and HypertensionDocument9 pages2.nam Et Al-2021-Retrospective Obs-Clinical Impact of BP Variability in Covid and HypertensionHi GamingNo ratings yet
- 1 s2.0 S2213007121000289 MainDocument4 pages1 s2.0 S2213007121000289 MainHi GamingNo ratings yet
- 1.ka Li Et Al-2021-Retrospective Obs-Day by Day BP Variability in Hospitalized Covid19Document6 pages1.ka Li Et Al-2021-Retrospective Obs-Day by Day BP Variability in Hospitalized Covid19Hi GamingNo ratings yet
- Pareyra-2022-Retrospective Cohort-RETAKO Registry AntiPlatelet at Discharge and Long Term Prognosis TTSDocument9 pagesPareyra-2022-Retrospective Cohort-RETAKO Registry AntiPlatelet at Discharge and Long Term Prognosis TTSHi GamingNo ratings yet
- 1.galie Et al-2002-RCT-Beraprost in Patients PAHDocument7 pages1.galie Et al-2002-RCT-Beraprost in Patients PAHHi GamingNo ratings yet
- 3.Dias-2015-RETROSPECTIVE COHORT-Antiplatelet Therapy in TakotsuboDocument6 pages3.Dias-2015-RETROSPECTIVE COHORT-Antiplatelet Therapy in TakotsuboHi GamingNo ratings yet
- 2.Yayehd-2016-COHORT-OFSETT STUDY Management of Takotsubo in FranceDocument9 pages2.Yayehd-2016-COHORT-OFSETT STUDY Management of Takotsubo in FranceHi GamingNo ratings yet
- AlternatorDocument3 pagesAlternatorVatsal PatelNo ratings yet
- A Generation of Contradictions-Unlocking Gen Z 2022 China FocusDocument25 pagesA Generation of Contradictions-Unlocking Gen Z 2022 China FocusCindy Xidan XiaoNo ratings yet
- Inspection and Test Plan Steel Sheet Pile DriDocument6 pagesInspection and Test Plan Steel Sheet Pile DriSofda Imela100% (1)
- Thermal Physics A Lecture NotesDocument35 pagesThermal Physics A Lecture Notescarlo mtongiNo ratings yet
- Ce Brochure 20july16Document76 pagesCe Brochure 20july16Yogesh SharmaNo ratings yet
- A Rail-To-Rail Constant Gain Buffered Op-Amp For Real Time Video ApplicationsDocument8 pagesA Rail-To-Rail Constant Gain Buffered Op-Amp For Real Time Video Applicationskvpk_vlsiNo ratings yet
- 2020.07.31 Marchese Declaration With ExhibitsDocument103 pages2020.07.31 Marchese Declaration With Exhibitsheather valenzuelaNo ratings yet
- Api RP 2a WSD 1pdf - CompressDocument1 pageApi RP 2a WSD 1pdf - CompressRamesh SelvarajNo ratings yet
- Manual PDFDocument9 pagesManual PDFRuth ResuelloNo ratings yet
- European Journal of Internal MedicineDocument4 pagesEuropean Journal of Internal Medicinesamer battatNo ratings yet
- DTS-00750 Mast Maintenance ManualDocument12 pagesDTS-00750 Mast Maintenance Manualsertecs polNo ratings yet
- Definition and Scope of Public FinanceDocument2 pagesDefinition and Scope of Public FinanceArfiya MubeenNo ratings yet
- Chemical ReactionDocument13 pagesChemical ReactionSujit LawareNo ratings yet
- DaburDocument3 pagesDaburchiru94No ratings yet
- Engr2227 Apr03Document10 pagesEngr2227 Apr03Mohamed AlqaisiNo ratings yet
- A Primer On Financial Time Series AnalysisDocument93 pagesA Primer On Financial Time Series AnalysisKM AgritechNo ratings yet
- G7-UNIT - I. (Module - 1 (Week 1 - 3 (Microscopy & Levels of Org.)Document8 pagesG7-UNIT - I. (Module - 1 (Week 1 - 3 (Microscopy & Levels of Org.)Margie Gabo Janoras - DaitolNo ratings yet
- Taylor Introms11GE PPT 03Document40 pagesTaylor Introms11GE PPT 03hddankerNo ratings yet
- X-Ray Generator Communication User's Manual - V1.80 L-IE-4211Document66 pagesX-Ray Generator Communication User's Manual - V1.80 L-IE-4211Marcos Peñaranda TintayaNo ratings yet
- KJR 20 880 PDFDocument14 pagesKJR 20 880 PDFNam LeNo ratings yet
- MNCs-consider-career-development-policyDocument2 pagesMNCs-consider-career-development-policySubhro MukherjeeNo ratings yet
- Rock Support Optimization in Himalayan TunnelsDocument7 pagesRock Support Optimization in Himalayan TunnelsHarold TaylorNo ratings yet
- Inner Unit EstimateDocument35 pagesInner Unit EstimateMir MoNo ratings yet
- BOOK-Deva-Oracle MaterialDocument177 pagesBOOK-Deva-Oracle MaterialPAVANN TNo ratings yet
- Sand Compaction MethodDocument124 pagesSand Compaction Methodisaych33ze100% (1)
- Science MELCsDocument42 pagesScience MELCsRanjell Allain TorresNo ratings yet
- St. Francis de Sales Sr. Sec. School, Gangapur CityDocument12 pagesSt. Francis de Sales Sr. Sec. School, Gangapur CityArtificial GammerNo ratings yet
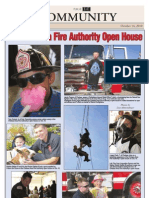
- CAFA Open House HighlightsDocument1 pageCAFA Open House HighlightsDaniel LaiNo ratings yet
- Osda Solar Module - Installation ManualDocument21 pagesOsda Solar Module - Installation ManualIOZEF1No ratings yet
- From Memphis To KingstonDocument19 pagesFrom Memphis To KingstonCarlos QuirogaNo ratings yet