You might also like
- Pediatrics: Compilation of Tables From Topnotch Pedia HandoutDocument6 pagesPediatrics: Compilation of Tables From Topnotch Pedia HandoutCielo Lomibao0% (1)
- RS ARI-Common Cold - PPT 93Document57 pagesRS ARI-Common Cold - PPT 93Dr.P.NatarajanNo ratings yet
- Pediatric Respiratory Cases: DR Hodan S. Ahmed, Department of Pediatrics and Child Health, Amoud Medical School, AUDocument24 pagesPediatric Respiratory Cases: DR Hodan S. Ahmed, Department of Pediatrics and Child Health, Amoud Medical School, AUmukhtar abddiNo ratings yet
- ENT Mnemonics 1Document13 pagesENT Mnemonics 1Riham Mohye Eldeen Mohammed88% (8)
- Covid 19 Daily Screening QuestionnaireDocument1 pageCovid 19 Daily Screening Questionnairezichara jumawanNo ratings yet
- COVID-19 DECLARATION FORM HCW Version 4 2021 (BI) NewDocument1 pageCOVID-19 DECLARATION FORM HCW Version 4 2021 (BI) NewNorliza Che DaudNo ratings yet
- Screening FormDocument2 pagesScreening FormMarie I. RosalesNo ratings yet
- Health Declaration Checklist SchoolDocument1 pageHealth Declaration Checklist SchoolClaire OrogoNo ratings yet
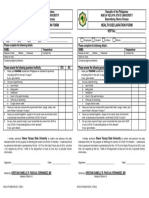
- YES NO YES NO: Date & Time: Name: Office Contact No.: Temperature: Date & Time: Name: Office Contact No.: TemperatureDocument2 pagesYES NO YES NO: Date & Time: Name: Office Contact No.: Temperature: Date & Time: Name: Office Contact No.: TemperatureYanna AbarquezNo ratings yet
- Office of The Vice President For OperationsDocument3 pagesOffice of The Vice President For OperationsJimMarkGasparCabanisasNo ratings yet
- Production Operator Production Operator Production Operator Solar Philippines Solar Philippines Solar PhilippinesDocument2 pagesProduction Operator Production Operator Production Operator Solar Philippines Solar Philippines Solar PhilippinesChristine Joy MatundanNo ratings yet
- Visitor Health QuestionerDocument1 pageVisitor Health QuestionerM FarhanNo ratings yet
- ISO Health ChecklistDocument1 pageISO Health ChecklistRonnel SaludezNo ratings yet
- Health Declaration Form: Respondent InformationDocument2 pagesHealth Declaration Form: Respondent Informationmyzzle mendarosNo ratings yet
- Health Dec New 1Document1 pageHealth Dec New 1RusselNo ratings yet
- HDF Entrance Oct 2022Document2 pagesHDF Entrance Oct 2022Lovly YeshyyNo ratings yet
- Health Dec New 1Document1 pageHealth Dec New 1Mary Rose RagasaNo ratings yet
- Health Decleration FormDocument1 pageHealth Decleration FormGabrile GUIOGUIONo ratings yet
- SMI COVID-19 Health Survey Form - RevisedDocument2 pagesSMI COVID-19 Health Survey Form - RevisedJess Rey Q. BaranNo ratings yet
- Health Declaration Form F2FDocument1 pageHealth Declaration Form F2FLizette Janiya SumantingNo ratings yet
- For More Information: Stay Home Stay SafeDocument2 pagesFor More Information: Stay Home Stay SafeDenver SignabenNo ratings yet
- SPMU FormDocument3 pagesSPMU FormHershey Ramos SabinoNo ratings yet
- 1st COT KlaiDocument6 pages1st COT KlaiJessica SebastianNo ratings yet
- Health FormDocument1 pageHealth Formnoera angel montemayorNo ratings yet
- Covid 19 Activity BookDocument11 pagesCovid 19 Activity BookGio GalarzaNo ratings yet
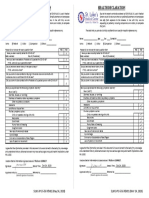
- Health Declaration: Teresita L. Jalandoni Provincial HospitalDocument2 pagesHealth Declaration: Teresita L. Jalandoni Provincial HospitalPrincess Faniega SugatonNo ratings yet
- Student School Flow Chart - 0918Document1 pageStudent School Flow Chart - 0918Taylor MoffittNo ratings yet
- Kaye-Anne Mangaring Powerpoint Presentation.Document21 pagesKaye-Anne Mangaring Powerpoint Presentation.kaye-Anne MangaringNo ratings yet
- Covid Employee Assessment FormDocument2 pagesCovid Employee Assessment FormSaniata Mae CorpuzNo ratings yet
- Screening Tool ColourDocument1 pageScreening Tool ColourMuhammad RamlanNo ratings yet
- Medical Examination Report (Aidil Fit)Document2 pagesMedical Examination Report (Aidil Fit)Husni WahyudiNo ratings yet
- HDF Students-Only A4Document2 pagesHDF Students-Only A4Trina PamaranNo ratings yet
- Health Declaration FormDocument2 pagesHealth Declaration FormResame ArochaNo ratings yet
- Health Declaration FormDocument2 pagesHealth Declaration FormRandy OpadiaNo ratings yet
- Health Declaration Form Health Declaration Form: Temperature: - TemperatureDocument1 pageHealth Declaration Form Health Declaration Form: Temperature: - TemperaturePrincess Ann MagbuhosNo ratings yet
- Inocencio School Student Health Declaration SheetDocument2 pagesInocencio School Student Health Declaration SheetCrunchy Fried RiceNo ratings yet
- Health DeclarationDocument2 pagesHealth DeclarationViktor Mikhael Roch BarbaNo ratings yet
- School Health Declaration Survey Form A4Document1 pageSchool Health Declaration Survey Form A4Clarizze AnnNo ratings yet
- Covid Info 2022 JanDocument10 pagesCovid Info 2022 JanIzzammil IzzuanNo ratings yet
- Covid Info 2022 JanDocument10 pagesCovid Info 2022 JanGunabathy SubramaniamNo ratings yet
- Experiment 2Document4 pagesExperiment 2Jenny Vhie S. VinagreraNo ratings yet
- Health Declaration FormDocument1 pageHealth Declaration Formedward mirandilla miranda jr.No ratings yet
- Health Declaration Health Declaration: YES NO YES NODocument1 pageHealth Declaration Health Declaration: YES NO YES NOmike tandocNo ratings yet
- What Is COVID-19?: Observe-Exercise 1Document7 pagesWhat Is COVID-19?: Observe-Exercise 1Brayan Guzmán JesúsNo ratings yet
- School Health DeclarationDocument3 pagesSchool Health DeclarationRuchie CardenoNo ratings yet
- Health Declaration Health Declaration: YES NO YES NODocument1 pageHealth Declaration Health Declaration: YES NO YES NOMagnificat filesNo ratings yet
- English As A Foreign Language: Teacher: Jos Cellphone: 990151662 Student: Grade: SectionDocument5 pagesEnglish As A Foreign Language: Teacher: Jos Cellphone: 990151662 Student: Grade: SectionTeachers J Learning EnglishNo ratings yet
- COVID-19 Screening Tool For Public Health and Health Links-Info SantéDocument27 pagesCOVID-19 Screening Tool For Public Health and Health Links-Info SantéTsania KusumawardaniNo ratings yet
- University of Northern Philippines: Health Declaration FormDocument1 pageUniversity of Northern Philippines: Health Declaration FormMelrhean Grace Denga-eyNo ratings yet
- SLMC Health Declaration FormDocument1 pageSLMC Health Declaration FormNikkiNo ratings yet
- Health Checklist Health Checklist: Temperature: Time Taken: Temperature: Time TakenDocument1 pageHealth Checklist Health Checklist: Temperature: Time Taken: Temperature: Time TakenHelen Paragas Solivar AranetaNo ratings yet
- Republic of The Philippines Department of Education Republic of The Philippines Department of EducationDocument1 pageRepublic of The Philippines Department of Education Republic of The Philippines Department of EducationElma Joyce BatuyongNo ratings yet
- Health Declaration Form-1-1Document2 pagesHealth Declaration Form-1-1Jimmy LaguraNo ratings yet
- Covid in EnglishDocument1 pageCovid in EnglishJoel Barrera QuispeNo ratings yet
- Covid 19 QuestionnaireDocument2 pagesCovid 19 QuestionnaireChristine De Villa-RagudoNo ratings yet
- Qr5IfQqx - Test - Permit 2023 03 11 PDFDocument2 pagesQr5IfQqx - Test - Permit 2023 03 11 PDFKevin Brian TulinganNo ratings yet
- Danielle Ali - Teaching Plan PowerpointDocument18 pagesDanielle Ali - Teaching Plan PowerpointDanielle Naomi (Danny)No ratings yet
- House of Representatives: Republic of The PhilippinesDocument2 pagesHouse of Representatives: Republic of The PhilippinesAlvin CerezoNo ratings yet
- Health ChecklistDocument1 pageHealth ChecklistMelba BarcelNo ratings yet
- Health Survey OfficeDocument2 pagesHealth Survey OfficeLara Denise BreizNo ratings yet
- Health Declaration With Covid VaccinationDocument1 pageHealth Declaration With Covid Vaccinationchiaruuh tNo ratings yet
- Health Declaration Form Health Declaration Form: Symptoms (Simtomas) YES NO Symptoms (Simtomas) YES NODocument2 pagesHealth Declaration Form Health Declaration Form: Symptoms (Simtomas) YES NO Symptoms (Simtomas) YES NOALFIE BARRERANo ratings yet
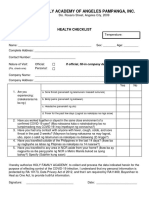
- Holy Family Academy of Angeles Pampanga, Inc.: Health ChecklistDocument1 pageHoly Family Academy of Angeles Pampanga, Inc.: Health ChecklistKarlNo ratings yet
- Math7 Q1 WW1-Version-5Document4 pagesMath7 Q1 WW1-Version-5Thatskie CajoteNo ratings yet
- 124th Flag Day Narrative ReportDocument2 pages124th Flag Day Narrative ReportThatskie CajoteNo ratings yet
- Muhammed Ali JinnahDocument1 pageMuhammed Ali JinnahThatskie CajoteNo ratings yet
- Poster Making ContestDocument1 pagePoster Making ContestThatskie CajoteNo ratings yet
- Contents of The Rle Written RequirementsDocument7 pagesContents of The Rle Written RequirementsElla RetizaNo ratings yet
- All Substitutes: For Informational Purposes Only. Consult A Doctor Before Taking Any MedicinesDocument3 pagesAll Substitutes: For Informational Purposes Only. Consult A Doctor Before Taking Any Medicinesvishakha AGRAWALNo ratings yet
- Vocabulary - Medications 2 - Mode - Report - Unit 2 - Lesson 4 - L5 G2 2021B - MyEnglishLabDocument2 pagesVocabulary - Medications 2 - Mode - Report - Unit 2 - Lesson 4 - L5 G2 2021B - MyEnglishLabAlejandra RomeroNo ratings yet
- 7 - Class 7Document81 pages7 - Class 7Zum BiiNo ratings yet
- Recurrent SnezzingDocument7 pagesRecurrent Snezzingrahulsinghroy17025No ratings yet
- Lesson Plan On RhinitisDocument15 pagesLesson Plan On Rhinitiskiran mahal100% (4)
- Common ColdDocument6 pagesCommon ColdRAM SOFTWARENo ratings yet
- 2nd Grading Science ReviewerDocument10 pages2nd Grading Science ReviewerEn CyNo ratings yet
- English For Hospital StaffDocument6 pagesEnglish For Hospital StaffВолодимир ТатарінNo ratings yet
- Buku Panduan CSL 3 ProtectedDocument15 pagesBuku Panduan CSL 3 ProtectedayuNo ratings yet
- Impinged Upon Adults Relationships With OthersDocument27 pagesImpinged Upon Adults Relationships With OthersЕлена КолядаNo ratings yet
- Disorders of The Nose and Paranasal SinusesDocument50 pagesDisorders of The Nose and Paranasal Sinusesphew1234567890No ratings yet
- Sino-Nasal Outcome Test (SNOT-22) Questionnaire: Patient's Name Date DOBDocument2 pagesSino-Nasal Outcome Test (SNOT-22) Questionnaire: Patient's Name Date DOBIchsanJuliansyahNo ratings yet
- 20 Prospectus RepertoryDocument54 pages20 Prospectus RepertoryjakNo ratings yet
- Rhinitis2008 Treatment GuidelinesDocument84 pagesRhinitis2008 Treatment Guidelinesdarkreign86No ratings yet
- Symptoms of Nasal PolypsDocument5 pagesSymptoms of Nasal Polypspratik hamalNo ratings yet
- Ent ExaminationDocument46 pagesEnt Examinationepic sound everNo ratings yet
- Understanding of Rhinosinusitis: Complication and Implication of Rhinosinusitis Daily PracticeDocument43 pagesUnderstanding of Rhinosinusitis: Complication and Implication of Rhinosinusitis Daily PracticeYunita Indah PalupiNo ratings yet
- Canine Kennel Cough Fact SheetDocument1 pageCanine Kennel Cough Fact Sheetdianarbk otuNo ratings yet
- Health & Fitness Vocabulary: Key DefinitionsDocument7 pagesHealth & Fitness Vocabulary: Key DefinitionsTeaching StuffNo ratings yet
- Upper Airway DisordersDocument25 pagesUpper Airway DisordersIliana EsquivelNo ratings yet
- Bacterial Sinusitis in Children: AcuteDocument11 pagesBacterial Sinusitis in Children: AcutefriscahalimNo ratings yet
- MCQ Ent 2023-24-1Document37 pagesMCQ Ent 2023-24-1Mani MozhiNo ratings yet
- Allergic PDFDocument17 pagesAllergic PDFSiska HarapanNo ratings yet
- Ent Cases MCQDocument10 pagesEnt Cases MCQDr-Firas Nayf Al-Thawabia100% (1)
- Case Presentation PDFDocument59 pagesCase Presentation PDFMark EvangelioNo ratings yet