You might also like
- Brain CT Essentials: Alexander Mamourian, MDDocument223 pagesBrain CT Essentials: Alexander Mamourian, MDCoding NinjaNo ratings yet
- CT Scan BasicsDocument28 pagesCT Scan BasicsPauline BurgosNo ratings yet
- Gastrointestinal Quiz AnswersDocument5 pagesGastrointestinal Quiz AnswersFranciskhokhyx III100% (5)
- Head CT ScanDocument84 pagesHead CT ScanAbegail IbañezNo ratings yet
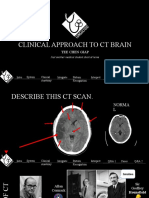
- Clinical Approach To CT BrainDocument34 pagesClinical Approach To CT BrainXiaoThoong LohNo ratings yet
- How To Read A Head CT ScanDocument60 pagesHow To Read A Head CT ScanPompomNo ratings yet
- How To Read A Head CT ScanDocument34 pagesHow To Read A Head CT ScanBoby ArisofianNo ratings yet
- Reading CT Scan of Human BrainDocument12 pagesReading CT Scan of Human BrainSumit RoyNo ratings yet
- Cara Membaca CTDocument61 pagesCara Membaca CTDio Alexander100% (1)
- Intro Head CTDocument34 pagesIntro Head CTbahar hoseiniNo ratings yet
- CKD Discharge Plan FINALDocument4 pagesCKD Discharge Plan FINALSienaNo ratings yet
- Case Study Hospital FormatDocument3 pagesCase Study Hospital Formatsenyorakath0% (1)
- NCP RHDocument3 pagesNCP RHKirstie Durano Goc-ong0% (1)
- NCP Decrease Cardiac OutputDocument2 pagesNCP Decrease Cardiac OutputAnonymous 2hJKVrNo ratings yet
- PRADEEP'S - Brain TumorDocument32 pagesPRADEEP'S - Brain TumorPRADEEPNo ratings yet
- Basic Neuroimaging (CT and MRI)Document56 pagesBasic Neuroimaging (CT and MRI)Dave Cronin100% (3)
- 5 Radiology CT Scan and MRIDocument9 pages5 Radiology CT Scan and MRIAbegail IbañezNo ratings yet
- Stroke SOL HandoutsDocument17 pagesStroke SOL HandoutsKeightNo ratings yet
- Radiological Anatomy of Normal CT Brain: Dr. Piyush Ojha DM Resident Department of Neurology Govt Medical College, KotaDocument33 pagesRadiological Anatomy of Normal CT Brain: Dr. Piyush Ojha DM Resident Department of Neurology Govt Medical College, KotaAbegail IbañezNo ratings yet
- Sample RadioDocument6 pagesSample RadioAbhishek SikarwarNo ratings yet
- Computed Tomography (CT), S. Computed Axial Tomography (CAT)Document11 pagesComputed Tomography (CT), S. Computed Axial Tomography (CAT)Waqas HaleemNo ratings yet
- Week 5 Skull and Brain (Basic Imaging ProtocolsDocument30 pagesWeek 5 Skull and Brain (Basic Imaging ProtocolsAbbas OmerNo ratings yet
- Cta Poster PresentationDocument1 pageCta Poster PresentationsreejithNo ratings yet
- Blood Can Be Very Bad (Perron Ich Acep 2005 Peds Course (1) )Document15 pagesBlood Can Be Very Bad (Perron Ich Acep 2005 Peds Course (1) )Moileon2011No ratings yet
- Brain ImagingDocument41 pagesBrain ImagingJose ErrazurizNo ratings yet
- Clinpract 11 00018Document7 pagesClinpract 11 00018Johnny CshNo ratings yet
- Presented By:: CC Abegail IbañezDocument42 pagesPresented By:: CC Abegail IbañezAbegail IbañezNo ratings yet
- RadioDocument62 pagesRadioimran khanNo ratings yet
- 5 Paranasal Sinus VariantsDocument6 pages5 Paranasal Sinus VariantsMatheusDorigattiSoldatelliNo ratings yet
- Brain AnatomyDocument9 pagesBrain Anatomymustafa mohammedNo ratings yet
- Sectional Anatomy Sectional AnatomyDocument34 pagesSectional Anatomy Sectional Anatomysyafiqa abdullahNo ratings yet
- Isuog: Detailed First-Trimester ExaminationDocument2 pagesIsuog: Detailed First-Trimester ExaminationhugoNo ratings yet
- Medical Imaging Modalities An Introduction: Stephan Scheidegger, 2016Document91 pagesMedical Imaging Modalities An Introduction: Stephan Scheidegger, 2016SharenceRuthEthelTerteNo ratings yet
- Vibe - January - 2024 - RadiologyDocument90 pagesVibe - January - 2024 - Radiologysneharam43No ratings yet
- Neuro Image 2008Document70 pagesNeuro Image 2008api-3784483100% (1)
- DFSGDFGDFDocument60 pagesDFSGDFGDFMada Dwi HariNo ratings yet
- Emergency Radiology: The Basics: Rathachai Kaewlai, MDDocument41 pagesEmergency Radiology: The Basics: Rathachai Kaewlai, MDsafitrie_liaNo ratings yet
- Acute Ischaemic Stroke: Recent Advances in Reperfusion TreatmentDocument11 pagesAcute Ischaemic Stroke: Recent Advances in Reperfusion TreatmentJose MartinezNo ratings yet
- CT Imaging 2019 Lyl v01 2Document72 pagesCT Imaging 2019 Lyl v01 2Ірина КарапутнаNo ratings yet
- FanbeamDocument5 pagesFanbeamAngela VacaNo ratings yet
- Intracranial Hemorrhage: Bleeding Inside The Skull. All: AcuteDocument8 pagesIntracranial Hemorrhage: Bleeding Inside The Skull. All: AcuteRitesh SharmaNo ratings yet
- CVD CSDTDocument3 pagesCVD CSDTrazeebhasssanNo ratings yet
- Subarachnoid Hemorrhage: Beyond Aneurysm: How To Manage?Document24 pagesSubarachnoid Hemorrhage: Beyond Aneurysm: How To Manage?heruNo ratings yet
- Cambodia Tut CT SinusespdfDocument5 pagesCambodia Tut CT SinusespdfDaniNo ratings yet
- Figures 8.1 Through 8.5 Represent 5 Patients Who Presented With Focal Neurological Deficits and Acute Change in Mental StatusDocument18 pagesFigures 8.1 Through 8.5 Represent 5 Patients Who Presented With Focal Neurological Deficits and Acute Change in Mental StatusNinaNo ratings yet
- CBD - DR Anna - DaraDocument10 pagesCBD - DR Anna - DaraAulia Putri ANo ratings yet
- 1 s2.0 S2666225620300385 Main PDFDocument7 pages1 s2.0 S2666225620300385 Main PDFwapeNo ratings yet
- Introduction To Medical ImagingDocument21 pagesIntroduction To Medical ImagingnuraliahNo ratings yet
- 8-Cerebral Venous Thrombosis Presented With.9Document4 pages8-Cerebral Venous Thrombosis Presented With.9abdeali hazariNo ratings yet
- S - Lession of The Infratemporal Fossa and Parapharyngeal Region, Congenital and Developmental Anomalies - RGDocument38 pagesS - Lession of The Infratemporal Fossa and Parapharyngeal Region, Congenital and Developmental Anomalies - RGanon_744980746No ratings yet
- MRI Spot Sign: Gadolinium Contrast Extravasation in An Expanding Intracerebral Hematoma On MRIDocument3 pagesMRI Spot Sign: Gadolinium Contrast Extravasation in An Expanding Intracerebral Hematoma On MRIPando RaitaNo ratings yet
- Inflammatory and Infectious Intracranial CystsDocument46 pagesInflammatory and Infectious Intracranial CystsZyad DoskiNo ratings yet
- San 12193Document6 pagesSan 12193Karla BFNo ratings yet
- Head Spine and Cerebral Vessels CTDocument50 pagesHead Spine and Cerebral Vessels CTMayNo ratings yet
- 3d Print CERNICA DANIEL PDFDocument1 page3d Print CERNICA DANIEL PDFSTOCARE DATENo ratings yet
- Proximal Humerus Fracture With Rotatotary Cuff InjuryDocument6 pagesProximal Humerus Fracture With Rotatotary Cuff Injuryhemanarasimha gandikotaNo ratings yet
- Y3. Introduction To Medical Imaging. Part 1Document42 pagesY3. Introduction To Medical Imaging. Part 1AishwariyaaAngelinaStephenNo ratings yet
- Imaging of Traumatic Intracranial HemorrhageDocument8 pagesImaging of Traumatic Intracranial HemorrhageSariRahmaYentiNo ratings yet
- IntroductionDocument60 pagesIntroductionKoushal Sharma, JammuNo ratings yet
- Central Nervous System Revised 2017.9Document107 pagesCentral Nervous System Revised 2017.9Steven OngNo ratings yet
- ECSTACY Final ReportingDocument15 pagesECSTACY Final ReportingCHRISTIAN RAY ALPAS PASILIAONo ratings yet
- Biology Investigatory Project: Samiksha Subhashish SarkarDocument35 pagesBiology Investigatory Project: Samiksha Subhashish SarkarSamiksha SarkarNo ratings yet
- IntussusceptionDocument2 pagesIntussusceptionAireen Mae P. NapigkitNo ratings yet
- Drug FeaturesDocument9 pagesDrug FeaturesLeah Claudia de OcampoNo ratings yet
- Worm Infestations 1Document18 pagesWorm Infestations 1Beta UserNo ratings yet
- Updates On Management of Gastric CancerDocument9 pagesUpdates On Management of Gastric CancerestherNo ratings yet
- Mycobacterial Culture: Presented by Pacôme Achimi, PHD Cermel-Tb Lab/GabonDocument44 pagesMycobacterial Culture: Presented by Pacôme Achimi, PHD Cermel-Tb Lab/GabonABHINABA GUPTANo ratings yet
- Aaa Gastrectomy NCP FinalDocument13 pagesAaa Gastrectomy NCP Finallexzaf100% (1)
- Serological Diagnosis of Infectious DiseasesDocument38 pagesSerological Diagnosis of Infectious DiseasesPurple basketNo ratings yet
- Pyloric StenosisDocument14 pagesPyloric StenosisbahtiarhabibiNo ratings yet
- Basic First AID: NSTP - CwtsDocument15 pagesBasic First AID: NSTP - CwtsBernadette Meriño MarchaNo ratings yet
- 2020.02.11 New Hospital Order Format Feb 14-23Document4 pages2020.02.11 New Hospital Order Format Feb 14-23Stib BrionesNo ratings yet
- Articles of FARRINGTON, HarveyDocument14 pagesArticles of FARRINGTON, HarveyMuhammad Ata Ul MustafaNo ratings yet
- A Patient's Guide To Adhesive CapsulitisDocument6 pagesA Patient's Guide To Adhesive Capsulitisamal sehat100% (1)
- Congenital Cytomegalovirus Infection Management and OutcomeDocument20 pagesCongenital Cytomegalovirus Infection Management and Outcomegomitas21No ratings yet
- DashBoard Health SampleDocument1 pageDashBoard Health SampleAliChana1No ratings yet
- Formula For Calculating The IV Flow RateDocument16 pagesFormula For Calculating The IV Flow Rateblythe RiveroNo ratings yet
- Liver TransplantationDocument17 pagesLiver Transplantationa_m_elsheemy1931No ratings yet
- Malaria Rapid Diagnostic Tests (RDTS)Document37 pagesMalaria Rapid Diagnostic Tests (RDTS)MegbaruNo ratings yet
- NCP GeriaDocument6 pagesNCP GeriaKeanu ArcillaNo ratings yet
- Oral Halitosis: Definitions: Breath Malodor, Defined As Foul or Offensive Odor of Expired Air, May BeDocument7 pagesOral Halitosis: Definitions: Breath Malodor, Defined As Foul or Offensive Odor of Expired Air, May BeSnowNo ratings yet
- Dilatation & Curettage: DR Ayswarya NarayanDocument19 pagesDilatation & Curettage: DR Ayswarya NarayanPrajwal Kp0% (1)
- Assess Appropriateness For Clinical Condition. Heart Rate Typically 50/min If BradyarrhythmiaDocument1 pageAssess Appropriateness For Clinical Condition. Heart Rate Typically 50/min If BradyarrhythmiaatikaNo ratings yet
- 2017 PTMAZEiftDocument4 pages2017 PTMAZEiftAnindya DeNo ratings yet