You might also like
- Share Wave Dispersion in Cronic Liver Disease From Physical Principles To Clinical UsfulnesDocument17 pagesShare Wave Dispersion in Cronic Liver Disease From Physical Principles To Clinical UsfulnesValentina IorgaNo ratings yet
- Therapeutic Endoscopic UltrasoundFrom EverandTherapeutic Endoscopic UltrasoundEvangelos KalaitzakisNo ratings yet
- 10 1002@jmri 26716Document18 pages10 1002@jmri 26716kinexNo ratings yet
- Dialysis Access ManagementFrom EverandDialysis Access ManagementSteven WuNo ratings yet
- Ultrasound or MR Elastography of Liver: Which One Shall I Use?Document6 pagesUltrasound or MR Elastography of Liver: Which One Shall I Use?Ancuta FeierNo ratings yet
- Contrast-Enhanced Ultrasound Imaging of Hepatic NeoplasmsFrom EverandContrast-Enhanced Ultrasound Imaging of Hepatic NeoplasmsWen-Ping WangNo ratings yet
- Medicina: Diagnostic Performance of Contrast-Enhanced Ultrasound (CEUS) in The Evaluation of Solid Renal MassesDocument8 pagesMedicina: Diagnostic Performance of Contrast-Enhanced Ultrasound (CEUS) in The Evaluation of Solid Renal MassesAgamNo ratings yet
- 1 s2.0 S0301562922004707 MainDocument9 pages1 s2.0 S0301562922004707 MainMarie-Helene Roy CardinalNo ratings yet
- Radiology: World Journal ofDocument17 pagesRadiology: World Journal ofAgamNo ratings yet
- Spleen Stiffness-Spleen Size-To-platelet Ratio RiskDocument6 pagesSpleen Stiffness-Spleen Size-To-platelet Ratio RiskValentina IorgaNo ratings yet
- BJR 85 1029Document9 pagesBJR 85 1029Anna MariaNo ratings yet
- Shearwave 17 12 11Document10 pagesShearwave 17 12 11Saritza MoleroNo ratings yet
- Ren 2024 Phys. Med. Biol. 69 025009Document15 pagesRen 2024 Phys. Med. Biol. 69 025009r496889996No ratings yet
- Repeatability of Shear Wave Elastography in LiverDocument16 pagesRepeatability of Shear Wave Elastography in LiverSaritza MoleroNo ratings yet
- Diagnostic Efficacy of Contrast-Enhanced Ultrasound For Small Renal MassesDocument6 pagesDiagnostic Efficacy of Contrast-Enhanced Ultrasound For Small Renal MassesAgamNo ratings yet
- Ishihara2018 Barret JaponesDocument9 pagesIshihara2018 Barret JaponesBety Puma PauccaraNo ratings yet
- Point Shear Wave Elastography of The Spleen in Predicting The Presence of Esophageal Varices in Cirrhosis: Liver Stiffness vs. Spleen StiffnessDocument7 pagesPoint Shear Wave Elastography of The Spleen in Predicting The Presence of Esophageal Varices in Cirrhosis: Liver Stiffness vs. Spleen StiffnessPriyan royNo ratings yet
- Evaluation of Liver Stiffness Measurments by Means of 2d SWE For Diagnosis VEDocument10 pagesEvaluation of Liver Stiffness Measurments by Means of 2d SWE For Diagnosis VEValentina IorgaNo ratings yet
- Accuracy of 2D and Point Shear Wave Elastography-Based Measurment For Diagnossi of Esophageal Varices A Systemic Review and Meta AnalisisDocument11 pagesAccuracy of 2D and Point Shear Wave Elastography-Based Measurment For Diagnossi of Esophageal Varices A Systemic Review and Meta AnalisisValentina IorgaNo ratings yet
- Texf Eu 2011 00600366 2Document8 pagesTexf Eu 2011 00600366 2JS57No ratings yet
- Endoscopic OCT With Forward-Looking Prob PDFDocument15 pagesEndoscopic OCT With Forward-Looking Prob PDFDrágus EmőkeNo ratings yet
- Missale2021 Article ValidationOfTheEuropeanLaryngoDocument13 pagesMissale2021 Article ValidationOfTheEuropeanLaryngosibel yıldırımNo ratings yet
- Wo-Dimensional Shear Wave Elastography PredictsDocument13 pagesWo-Dimensional Shear Wave Elastography PredictsValentina IorgaNo ratings yet
- Background: Open Access Original Article DOI: 10.7759/cureus.10987Document5 pagesBackground: Open Access Original Article DOI: 10.7759/cureus.10987hengkyNo ratings yet
- Jmi 006 044003Document11 pagesJmi 006 044003kaythinzarphuNo ratings yet
- Choice of Surgical Methods in Patients With Urinary Stone DiseaseDocument6 pagesChoice of Surgical Methods in Patients With Urinary Stone DiseaseCentral Asian StudiesNo ratings yet
- Liver Fibrosis With Two-Dimensional US Shear-Wave Elastography in Participants With Chronic Hepatitis B A Prospective Multicenter StudyDocument9 pagesLiver Fibrosis With Two-Dimensional US Shear-Wave Elastography in Participants With Chronic Hepatitis B A Prospective Multicenter StudynanNo ratings yet
- UEG Journal - 2017 - Iglesias Garcia - Differential Diagnosis of Solid Pancreatic Masses Contrast Enhanced HarmonicDocument11 pagesUEG Journal - 2017 - Iglesias Garcia - Differential Diagnosis of Solid Pancreatic Masses Contrast Enhanced HarmonicMahesh KadamNo ratings yet
- Evaluation of Focal Hepatic Lesions by Using Ultrasound EvaluationDocument2 pagesEvaluation of Focal Hepatic Lesions by Using Ultrasound EvaluationNaufal LutfiNo ratings yet
- Jcen 22 2 78Document7 pagesJcen 22 2 78Aik NoeraNo ratings yet
- 2 D SWE DD Fibrosis Non Fibrosis - 240416 - 190701Document6 pages2 D SWE DD Fibrosis Non Fibrosis - 240416 - 190701bella friscaamaliaNo ratings yet
- ACR Appropriateness Criteria Acute Onset FlankDocument7 pagesACR Appropriateness Criteria Acute Onset FlankcubirojasNo ratings yet
- Contrast-Enhanced Ultrasonography of Hepatocellular Carcinoma: Correlation Between Quantitative Parameters and Histological GradingDocument9 pagesContrast-Enhanced Ultrasonography of Hepatocellular Carcinoma: Correlation Between Quantitative Parameters and Histological GradingUp TayyuNo ratings yet
- Interobserver and Intraobserver Variability in The Radiological Assessment of Sialolithiasis Using Cone Beam Computed TomographyDocument5 pagesInterobserver and Intraobserver Variability in The Radiological Assessment of Sialolithiasis Using Cone Beam Computed TomographydaruNo ratings yet
- Schwartz2002 PDFDocument7 pagesSchwartz2002 PDFnova sorayaNo ratings yet
- Digestive and Liver DiseaseDocument12 pagesDigestive and Liver DiseasevickyarmasrudNo ratings yet
- Accuracy of Core Needle Biopsy For The Diagnosis of Osteosarcoma - A Retrospective Analysis of 73 PatientsDocument5 pagesAccuracy of Core Needle Biopsy For The Diagnosis of Osteosarcoma - A Retrospective Analysis of 73 Patientschenth3r3No ratings yet
- 2015 PDFDocument4 pages2015 PDFJose M. GuerreroNo ratings yet
- 2015 PDFDocument4 pages2015 PDFJose M. GuerreroNo ratings yet
- Quantitative Comparison of Transient Elastography (TE), Shear Wave Elastography (SWE) and Liver Biopsy Results of Patients With Chronic Liver DiseaseDocument4 pagesQuantitative Comparison of Transient Elastography (TE), Shear Wave Elastography (SWE) and Liver Biopsy Results of Patients With Chronic Liver DiseaseJose M. GuerreroNo ratings yet
- Mucinous Cystic Neoplasm of Liver - Peeling Sign Mitigates A Diagnostic ConundrumDocument8 pagesMucinous Cystic Neoplasm of Liver - Peeling Sign Mitigates A Diagnostic ConundrumIJAR JOURNALNo ratings yet
- Biswas2014 PDFDocument7 pagesBiswas2014 PDFDhruv MahajanNo ratings yet
- Ultrasound Imaging of The AbdomenDocument224 pagesUltrasound Imaging of The AbdomenAsztalos Attila100% (9)
- Artikel MBT Flowrate DCEMRIDocument9 pagesArtikel MBT Flowrate DCEMRILucas ParretNo ratings yet
- Radiotherapy and OncologyDocument14 pagesRadiotherapy and OncologyJavier RodríguezNo ratings yet
- The Role of Bosniak ClassificationDocument6 pagesThe Role of Bosniak ClassificationraduNo ratings yet
- Microvascular Doppler Ultrasound in Children With Acute PyelonephritisDocument7 pagesMicrovascular Doppler Ultrasound in Children With Acute PyelonephritisAinunnisa MansurNo ratings yet
- (545. JAMP - Sushrit) 633-636 FinalDocument4 pages(545. JAMP - Sushrit) 633-636 FinalDinda SaviraNo ratings yet
- US Elastography in Liver Frulio DX Interv Im 2013Document20 pagesUS Elastography in Liver Frulio DX Interv Im 2013gatoflacoNo ratings yet
- Ca Gastrico y Endoscopia 2Document10 pagesCa Gastrico y Endoscopia 2Israael JuuareezNo ratings yet
- 1 s2.0 S0378603X16300997 MainDocument9 pages1 s2.0 S0378603X16300997 MaintaufikolingNo ratings yet
- 1530 Jul 27Document6 pages1530 Jul 27kelvin amahNo ratings yet
- Contribution of Endoscopic Ultrasound in Pancreatic MassesDocument6 pagesContribution of Endoscopic Ultrasound in Pancreatic MassesIJAR JOURNALNo ratings yet
- Elasto Viena JaDocument5 pagesElasto Viena JailyaNo ratings yet
- Dual-Energy CT Characteristics of Colon and Rectal Cancer Allows Differentiation From Stool by Dual-Source CTDocument6 pagesDual-Energy CT Characteristics of Colon and Rectal Cancer Allows Differentiation From Stool by Dual-Source CTRyana Fitriana IINo ratings yet
- Automatic Semantic Segmentation of Kidney Cysts in MR Images of Patients Affected by Autosomal Dominant Polycystic Kidney DiseaseDocument9 pagesAutomatic Semantic Segmentation of Kidney Cysts in MR Images of Patients Affected by Autosomal Dominant Polycystic Kidney DiseaseSonia Akter 1064No ratings yet
- Ni Wayan Dwi NovitaDocument6 pagesNi Wayan Dwi NovitaDwi ZirobeNo ratings yet
- Possibilities of MRI Diagnostics of Focal Liver DefeatsDocument8 pagesPossibilities of MRI Diagnostics of Focal Liver DefeatsCentral Asian StudiesNo ratings yet
- Liver FibrosisDocument10 pagesLiver FibrosisDavidNo ratings yet
- Pubid 1576378494Document13 pagesPubid 1576378494Teodor CabelNo ratings yet
- Chen 2008Document3 pagesChen 2008Teodor CabelNo ratings yet
- Hepatic Shear Wave ElastographyDocument2 pagesHepatic Shear Wave ElastographyTeodor CabelNo ratings yet
- ARFI Cut-Off Values and Significance of Standard Deviation For Liver Fibrosis Staging in Patients With Chronic Liver DiseaseDocument7 pagesARFI Cut-Off Values and Significance of Standard Deviation For Liver Fibrosis Staging in Patients With Chronic Liver DiseaseTeodor CabelNo ratings yet
- Monster Scales and Modes - by Dave CelentanoDocument48 pagesMonster Scales and Modes - by Dave CelentanoTeodor CabelNo ratings yet
- John Mayer - Slow Dancing in A Burning RoomDocument3 pagesJohn Mayer - Slow Dancing in A Burning RoomTeodor CabelNo ratings yet
- Autoimmunity Reviews: Maximiliano Javier Jiménez-Dalmaroni, M. Eric Gerswhin, Iannis E. AdamopoulosDocument8 pagesAutoimmunity Reviews: Maximiliano Javier Jiménez-Dalmaroni, M. Eric Gerswhin, Iannis E. AdamopoulosTeodor CabelNo ratings yet
- Working in A Group EssayDocument4 pagesWorking in A Group Essayjvscmacaf100% (2)
- Measuring Basic Observations: OSCE ChecklistDocument2 pagesMeasuring Basic Observations: OSCE Checklistahmad50% (4)
- Consent in Gaming FillableDocument1 pageConsent in Gaming FillableChuck Barnard100% (1)
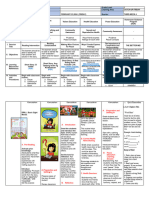
- DLL Catch Up Friday Week 4Document16 pagesDLL Catch Up Friday Week 4Maryanne Labaso93% (27)
- Principles of Adult Learning DocumentDocument41 pagesPrinciples of Adult Learning Documentحشيمة الروحNo ratings yet
- Brain Multimodal Monitoring in PortoDocument30 pagesBrain Multimodal Monitoring in PortoCeleste DiasNo ratings yet
- Current Trends in Nursing AdministrationDocument50 pagesCurrent Trends in Nursing AdministrationGeorge Michael LimNo ratings yet
- Anti-Lock Braking System (ABS) For Trucks ... - Meritor WABCO PDFDocument112 pagesAnti-Lock Braking System (ABS) For Trucks ... - Meritor WABCO PDFEudis PinedaNo ratings yet
- Emily Skye - 30 Day Ab Shred PDFDocument100 pagesEmily Skye - 30 Day Ab Shred PDFalaa bachacha100% (1)
- Template For Co Ntingency Planning DivisionDocument21 pagesTemplate For Co Ntingency Planning Divisionelizer encarnacionNo ratings yet
- Med Surg 1Document14 pagesMed Surg 1Wendera T. S CooperNo ratings yet
- Covid 19 Daily Reporting DasDocument6 pagesCovid 19 Daily Reporting DasRuhayati88gmail.com EyeshieldNo ratings yet
- Am Medicine - Com 210815 m77Document596 pagesAm Medicine - Com 210815 m77Cai Velasco Decena100% (16)
- FilariaDocument85 pagesFilariaRajkishor YadavNo ratings yet
- Letter - For - Students - 1ST - Year - Programmes (Gu)Document2 pagesLetter - For - Students - 1ST - Year - Programmes (Gu)Ayush SinghNo ratings yet
- Epidemiology and Pathogenesis of Benign Prostatic Hyperplasia - UpToDateDocument9 pagesEpidemiology and Pathogenesis of Benign Prostatic Hyperplasia - UpToDateFeer VillarrealNo ratings yet
- Beatriz Colomina X Ray Architecture Lars Muller (001 045)Document45 pagesBeatriz Colomina X Ray Architecture Lars Muller (001 045)SABUESO FINANCIERONo ratings yet
- Sleep Diary InstructionsDocument1 pageSleep Diary InstructionsyewwNo ratings yet
- Secondary - Report Card Comment CodesDocument2 pagesSecondary - Report Card Comment CodesRICHARD SARDON LEONNo ratings yet
- Es Compleat Coolant Eg Premix - MSDS - Lt16587aDocument6 pagesEs Compleat Coolant Eg Premix - MSDS - Lt16587aCesar G.No ratings yet
- 7627 23679 1 PBDocument7 pages7627 23679 1 PBRiska AmaliaNo ratings yet
- Farid Pharmacology FinalDocument12 pagesFarid Pharmacology FinalFariedfrd0% (1)
- Biografija: DR - Sc. Mirza MoranjkićDocument2 pagesBiografija: DR - Sc. Mirza MoranjkićEnis HuskanovicNo ratings yet
- Hand Notes On Questions FramingDocument16 pagesHand Notes On Questions FramingNOORUDDINNo ratings yet
- Pulse Diagnosis - CONCISE WORKBOOKDocument21 pagesPulse Diagnosis - CONCISE WORKBOOKVishnu Prabhu SivasubramaniamNo ratings yet
- Englishcrumbs c2 LevelDocument101 pagesEnglishcrumbs c2 Leveleslerjinar1No ratings yet
- Reading Program Terminal Report-2020Document2 pagesReading Program Terminal Report-2020roselyn galinatoNo ratings yet
- DERMOID CYST FINAL NaDocument56 pagesDERMOID CYST FINAL NaRhobic ManansalaNo ratings yet
- Mcat Power Practice Learningexpress PDFDocument244 pagesMcat Power Practice Learningexpress PDFMamoNo ratings yet
- SAG - Emergency Medical Services NC II (Amended 2013)Document5 pagesSAG - Emergency Medical Services NC II (Amended 2013)Jaypz DelNo ratings yet
- The Obesity Code: Unlocking the Secrets of Weight LossFrom EverandThe Obesity Code: Unlocking the Secrets of Weight LossRating: 4 out of 5 stars4/5 (6)
- The Age of Magical Overthinking: Notes on Modern IrrationalityFrom EverandThe Age of Magical Overthinking: Notes on Modern IrrationalityRating: 4 out of 5 stars4/5 (28)
- By the Time You Read This: The Space between Cheslie's Smile and Mental Illness—Her Story in Her Own WordsFrom EverandBy the Time You Read This: The Space between Cheslie's Smile and Mental Illness—Her Story in Her Own WordsNo ratings yet
- Think This, Not That: 12 Mindshifts to Breakthrough Limiting Beliefs and Become Who You Were Born to BeFrom EverandThink This, Not That: 12 Mindshifts to Breakthrough Limiting Beliefs and Become Who You Were Born to BeRating: 2 out of 5 stars2/5 (1)
- ADHD is Awesome: A Guide to (Mostly) Thriving with ADHDFrom EverandADHD is Awesome: A Guide to (Mostly) Thriving with ADHDRating: 5 out of 5 stars5/5 (2)
- LIT: Life Ignition Tools: Use Nature's Playbook to Energize Your Brain, Spark Ideas, and Ignite ActionFrom EverandLIT: Life Ignition Tools: Use Nature's Playbook to Energize Your Brain, Spark Ideas, and Ignite ActionRating: 4 out of 5 stars4/5 (404)
- Raising Mentally Strong Kids: How to Combine the Power of Neuroscience with Love and Logic to Grow Confident, Kind, Responsible, and Resilient Children and Young AdultsFrom EverandRaising Mentally Strong Kids: How to Combine the Power of Neuroscience with Love and Logic to Grow Confident, Kind, Responsible, and Resilient Children and Young AdultsRating: 5 out of 5 stars5/5 (1)
- Summary: Outlive: The Science and Art of Longevity by Peter Attia MD, With Bill Gifford: Key Takeaways, Summary & AnalysisFrom EverandSummary: Outlive: The Science and Art of Longevity by Peter Attia MD, With Bill Gifford: Key Takeaways, Summary & AnalysisRating: 4.5 out of 5 stars4.5/5 (42)
- Summary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedFrom EverandSummary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedRating: 5 out of 5 stars5/5 (81)
- The Ritual Effect: From Habit to Ritual, Harness the Surprising Power of Everyday ActionsFrom EverandThe Ritual Effect: From Habit to Ritual, Harness the Surprising Power of Everyday ActionsRating: 3.5 out of 5 stars3.5/5 (3)
- Outlive: The Science and Art of Longevity by Peter Attia: Key Takeaways, Summary & AnalysisFrom EverandOutlive: The Science and Art of Longevity by Peter Attia: Key Takeaways, Summary & AnalysisRating: 4 out of 5 stars4/5 (1)
- Why We Die: The New Science of Aging and the Quest for ImmortalityFrom EverandWhy We Die: The New Science of Aging and the Quest for ImmortalityRating: 4 out of 5 stars4/5 (3)
- The Body Keeps the Score by Bessel Van der Kolk, M.D. - Book Summary: Brain, Mind, and Body in the Healing of TraumaFrom EverandThe Body Keeps the Score by Bessel Van der Kolk, M.D. - Book Summary: Brain, Mind, and Body in the Healing of TraumaRating: 4.5 out of 5 stars4.5/5 (266)
- Sleep Stories for Adults: Overcome Insomnia and Find a Peaceful AwakeningFrom EverandSleep Stories for Adults: Overcome Insomnia and Find a Peaceful AwakeningRating: 4 out of 5 stars4/5 (3)
- Love Life: How to Raise Your Standards, Find Your Person, and Live Happily (No Matter What)From EverandLove Life: How to Raise Your Standards, Find Your Person, and Live Happily (No Matter What)No ratings yet
- When the Body Says No by Gabor Maté: Key Takeaways, Summary & AnalysisFrom EverandWhen the Body Says No by Gabor Maté: Key Takeaways, Summary & AnalysisRating: 3.5 out of 5 stars3.5/5 (2)
- Gut: the new and revised Sunday Times bestsellerFrom EverandGut: the new and revised Sunday Times bestsellerRating: 4 out of 5 stars4/5 (392)
- Cult, A Love Story: Ten Years Inside a Canadian Cult and the Subsequent Long Road of RecoveryFrom EverandCult, A Love Story: Ten Years Inside a Canadian Cult and the Subsequent Long Road of RecoveryRating: 4 out of 5 stars4/5 (44)
- Dark Psychology & Manipulation: Discover How To Analyze People and Master Human Behaviour Using Emotional Influence Techniques, Body Language Secrets, Covert NLP, Speed Reading, and Hypnosis.From EverandDark Psychology & Manipulation: Discover How To Analyze People and Master Human Behaviour Using Emotional Influence Techniques, Body Language Secrets, Covert NLP, Speed Reading, and Hypnosis.Rating: 4.5 out of 5 stars4.5/5 (110)
- The Marshmallow Test: Mastering Self-ControlFrom EverandThe Marshmallow Test: Mastering Self-ControlRating: 4.5 out of 5 stars4.5/5 (58)
- Mindset by Carol S. Dweck - Book Summary: The New Psychology of SuccessFrom EverandMindset by Carol S. Dweck - Book Summary: The New Psychology of SuccessRating: 4.5 out of 5 stars4.5/5 (328)
- Dark Psychology: Learn To Influence Anyone Using Mind Control, Manipulation And Deception With Secret Techniques Of Dark Persuasion, Undetected Mind Control, Mind Games, Hypnotism And BrainwashingFrom EverandDark Psychology: Learn To Influence Anyone Using Mind Control, Manipulation And Deception With Secret Techniques Of Dark Persuasion, Undetected Mind Control, Mind Games, Hypnotism And BrainwashingRating: 4 out of 5 stars4/5 (1138)
- Troubled: A Memoir of Foster Care, Family, and Social ClassFrom EverandTroubled: A Memoir of Foster Care, Family, and Social ClassRating: 4.5 out of 5 stars4.5/5 (26)