You might also like
- Domestic ViolenceDocument40 pagesDomestic Violencepetrescu miaNo ratings yet
- Notes On Psychiatry: TypesDocument17 pagesNotes On Psychiatry: TypesMAY100% (1)
- Template For Athlete 1Document26 pagesTemplate For Athlete 1Florita LagramaNo ratings yet
- 2020 Gallery of AthletesDocument5 pages2020 Gallery of AthletesMaria Elaine De CastroNo ratings yet
- English-Italian Medical TermsDocument12 pagesEnglish-Italian Medical Termsionicaa3No ratings yet
- Updated - NCR e Sports Forms Generator As August 2019Document281 pagesUpdated - NCR e Sports Forms Generator As August 2019Romuel Doydora BituaNo ratings yet
- 3x3 Basketball Secondary Girls Event RecordsDocument5 pages3x3 Basketball Secondary Girls Event RecordsHanzel NietesNo ratings yet
- 1 2 3 4 Last Name First Name Middle Name Coach 1 Manlapaz Ma. Victoria Estrella Assitant Coach 2 Chaperone 3Document48 pages1 2 3 4 Last Name First Name Middle Name Coach 1 Manlapaz Ma. Victoria Estrella Assitant Coach 2 Chaperone 3MhinSirVNo ratings yet
- Regional Meet: Regional Screening ADN Accreditation CommitteeDocument8 pagesRegional Meet: Regional Screening ADN Accreditation CommitteeAlden PaceñoNo ratings yet
- Sample Athletics Records FormsDocument16 pagesSample Athletics Records FormsHalem Laroya LucernasNo ratings yet
- Regional Meet: Regional Screening ADN Accreditation CommitteeDocument7 pagesRegional Meet: Regional Screening ADN Accreditation CommitteeAira Rose Crencia CabaronNo ratings yet
- PSU Application for Practice TeachingDocument1 pagePSU Application for Practice TeachingNoreen PayopayNo ratings yet
- MMHS Ar G-AlleryDocument16 pagesMMHS Ar G-AlleryMyla Rose AcobaNo ratings yet
- Gallery of Athletes LatestDocument4 pagesGallery of Athletes LatestGean AcabalNo ratings yet
- Gallery-of-Athletes - GirlsDocument4 pagesGallery-of-Athletes - Girlsjoselito papaNo ratings yet
- PSU Application for Practice TeachingDocument1 pagePSU Application for Practice TeachingNoreen PayopayNo ratings yet
- Holy Rosary School Student Directory 2022-2023Document4 pagesHoly Rosary School Student Directory 2022-2023Glory Ann DelovioNo ratings yet
- 3x3 GalleryDocument4 pages3x3 GalleryMaricel Ang BajeyoNo ratings yet
- 2023 Photo Gallery Athletics Secondary GirlsDocument12 pages2023 Photo Gallery Athletics Secondary GirlsRyan PurisimaNo ratings yet
- Screening Committee Register: Republic of The Philippines Department of Education Region Ix, Zamboanga PeninsulaDocument21 pagesScreening Committee Register: Republic of The Philippines Department of Education Region Ix, Zamboanga PeninsulaVenna Ross URGNo ratings yet
- CANDA 2024 Athlete Record 093432Document17 pagesCANDA 2024 Athlete Record 093432hannahgracecanda33No ratings yet
- A - Coach RecordDocument1 pageA - Coach Recordgracezel cachuelaNo ratings yet
- 2020 - Gallery of Athletes - FOR SECONDARYDocument6 pages2020 - Gallery of Athletes - FOR SECONDARYJerwin LualhatiNo ratings yet
- Screening Committee Register: Republic of The Philippines Department of Education Region Ix, Zamboanga PeninsulaDocument17 pagesScreening Committee Register: Republic of The Philippines Department of Education Region Ix, Zamboanga PeninsulaMike PerezNo ratings yet
- Local Media1464799490718715655Document4 pagesLocal Media1464799490718715655Kenneth Emerson IgnacioNo ratings yet
- 2020 Gallery of Athletes For TAEKWONDODocument10 pages2020 Gallery of Athletes For TAEKWONDORiza Joy PalomarNo ratings yet
- 2023-Gallery-of-Athletes-Secondary (1)Document4 pages2023-Gallery-of-Athletes-Secondary (1)jcbaybayan.upNo ratings yet
- Input Data Sheet For E-Class Record: Learners' Names Basic InformationDocument24 pagesInput Data Sheet For E-Class Record: Learners' Names Basic InformationBiboyNo ratings yet
- 2024 Athlete Record 1Document18 pages2024 Athlete Record 1BriandelFierroNo ratings yet
- Subacos 2024 - Athlete-Record V3Document20 pagesSubacos 2024 - Athlete-Record V3Nayr ZdahbNo ratings yet
- Laudit, Arnel Z.Document30 pagesLaudit, Arnel Z.Japs De la CruzNo ratings yet
- 2020 Gallery of Athletes For Secondary Edited A4 Final NewDocument5 pages2020 Gallery of Athletes For Secondary Edited A4 Final NewMaricel Ang BajeyoNo ratings yet
- 2020 Gallery of Athletes 1Document7 pages2020 Gallery of Athletes 1May MayaNo ratings yet
- Regional Table Tennis Athlete ProfileDocument7 pagesRegional Table Tennis Athlete ProfileNelma ArnaizNo ratings yet
- 2020 Gallery of AthletesDocument4 pages2020 Gallery of Athletesrobertlouie.delacruzNo ratings yet
- 2020 Gallery of AthletesDocument5 pages2020 Gallery of AthletesRosselle May JumayaoNo ratings yet
- 2ND QUARTER TEST RESULTS FOR GRADE SIX SAPPHIREDocument8 pages2ND QUARTER TEST RESULTS FOR GRADE SIX SAPPHIREPrincis CianoNo ratings yet
- Athletes Glaisa AgbayDocument6 pagesAthletes Glaisa AgbayJerome DesameroNo ratings yet
- Gallery Forms New 1Document2 pagesGallery Forms New 1132844No ratings yet
- 2020 Gallery of Athletes GIRLSDocument5 pages2020 Gallery of Athletes GIRLStarbzyNo ratings yet
- MMGEC - Membership Application Form R8 Gideons v2Document1 pageMMGEC - Membership Application Form R8 Gideons v2AYSA GENEVIERE O.LAPUZNo ratings yet
- 2023 Athlete RecordDocument26 pages2023 Athlete RecordJeferson Eborda RoselNo ratings yet
- 2023 Athlete Record1Document26 pages2023 Athlete Record1daxian.barrettoNo ratings yet
- Template For Athlete 1Document26 pagesTemplate For Athlete 1Florita LagramaNo ratings yet
- Classroom Daily Health Monitoring Tool For Covid-19: Grade 11-ChrysanthemumDocument4 pagesClassroom Daily Health Monitoring Tool For Covid-19: Grade 11-Chrysanthemumkimbeerlyn doromasNo ratings yet
- Ersonal ATA Heet: PerinDocument8 pagesErsonal ATA Heet: PerinbarangayrizalcleanandgreenNo ratings yet
- Climaco, DominicDocument16 pagesClimaco, DominicEllen Bahatan SinahonNo ratings yet
- Athlete RiveraDocument10 pagesAthlete RiveraAvi Auerbach AvilaNo ratings yet
- Elementary Table Tennis Athlete ProfileDocument10 pagesElementary Table Tennis Athlete ProfileAvi Auerbach AvilaNo ratings yet
- Billote, CymarcDocument16 pagesBillote, CymarcEllen Bahatan SinahonNo ratings yet
- Screening Committee Register: Republic of The Philippines Department of Education Region Ix, Zamboanga PeninsulaDocument20 pagesScreening Committee Register: Republic of The Philippines Department of Education Region Ix, Zamboanga Peninsulaofelia ligtasNo ratings yet
- Lastname Firstname M.I: Inclusive Dates Sports Event Athletic Meet Remarks Coaches Division Pess SupervisorDocument9 pagesLastname Firstname M.I: Inclusive Dates Sports Event Athletic Meet Remarks Coaches Division Pess SupervisorAloha Aguilar BrusasNo ratings yet
- 2020 Gallery of AthletesDocument5 pages2020 Gallery of AthletesJulius CandanoNo ratings yet
- Palaro Data Entry ATHLETE ACAINDocument12 pagesPalaro Data Entry ATHLETE ACAINmarina abanNo ratings yet
- Isulan Nhs Jhs Shs Profiling Template BlankDocument48 pagesIsulan Nhs Jhs Shs Profiling Template BlankBenny CalloNo ratings yet
- Pangasinan Schools Division volleyball recordsDocument4 pagesPangasinan Schools Division volleyball recordsJessabelle OnzaNo ratings yet
- Monitoring Tool Contact TimeDocument4 pagesMonitoring Tool Contact TimeLoida Cabus AroNo ratings yet
- 2020 Gallery of AthletesDocument5 pages2020 Gallery of AthletesBryan YasgilNo ratings yet
- 2020 Gallery of AthletesDocument8 pages2020 Gallery of AthletesClint AbantoNo ratings yet
- 2024 Paralympics Screening Form For Paralympics GamesDocument6 pages2024 Paralympics Screening Form For Paralympics Gameschristineirish.catalanNo ratings yet
- Athletes CredentialsDocument22 pagesAthletes CredentialsMael AlimesNo ratings yet
- 2020 Gallery of Athletes For Secondary BoysDocument9 pages2020 Gallery of Athletes For Secondary BoysJoanna Mag-apanNo ratings yet
- Authority To Travel REGINE A. PAGLINAWANDocument9 pagesAuthority To Travel REGINE A. PAGLINAWANChristian James ArenasNo ratings yet
- Starts 23Document12 pagesStarts 23Christian James ArenasNo ratings yet
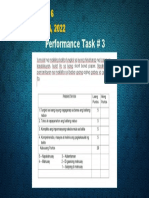
- A.P 6 - Performance Task # 3 June 14, 2022Document1 pageA.P 6 - Performance Task # 3 June 14, 2022Christian James ArenasNo ratings yet
- Brigada Eskwela Kick Off ProgrammeDocument1 pageBrigada Eskwela Kick Off ProgrammeChristian James ArenasNo ratings yet
- Santiago Elementary School 2021-2022 Academic AwardeesDocument22 pagesSantiago Elementary School 2021-2022 Academic AwardeesChristian James ArenasNo ratings yet
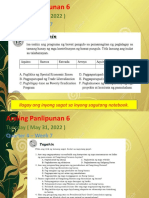
- Araling Panlipunan 6 - Gawain - Week 6 - May 24, 2022Document2 pagesAraling Panlipunan 6 - Gawain - Week 6 - May 24, 2022Christian James ArenasNo ratings yet
- Program For Distribution of Bags Per Grade LevelDocument8 pagesProgram For Distribution of Bags Per Grade LevelChristian James ArenasNo ratings yet
- PSA PSA PSA: Waiting AreaDocument7 pagesPSA PSA PSA: Waiting AreaChristian James ArenasNo ratings yet
- Medication Errors: 12 Questions Patients Should Ask Their Doctors and PharmacistsDocument30 pagesMedication Errors: 12 Questions Patients Should Ask Their Doctors and PharmacistsVero YosaNo ratings yet
- Confusion: Koech KM Fri Feb 12, 2010Document23 pagesConfusion: Koech KM Fri Feb 12, 2010api-50425236No ratings yet
- Bagga NephrologyDocument291 pagesBagga NephrologyAnangsha DattaNo ratings yet
- I. General Primary Health Care Facility Design Information: Research RequirementsDocument24 pagesI. General Primary Health Care Facility Design Information: Research RequirementsJoyce LapuzNo ratings yet
- CV SEO-Optimized CV Title for Dental ProfessionalDocument3 pagesCV SEO-Optimized CV Title for Dental Professionalomran turbiNo ratings yet
- Bathe, Illness, Outpatient, Disability, Discharged, Geriatrics, Increase, Administer, Preventive, TherapyDocument3 pagesBathe, Illness, Outpatient, Disability, Discharged, Geriatrics, Increase, Administer, Preventive, TherapyReka KutasiNo ratings yet
- Reflection Video Why Mrs. X Die MATERNALDocument2 pagesReflection Video Why Mrs. X Die MATERNALQueenzee AsuncionNo ratings yet
- KISI Bahasa InggrisDocument4 pagesKISI Bahasa InggrisVerina HerliyantiNo ratings yet
- Benefits of Computer Use in Health Care Systems PDFDocument3 pagesBenefits of Computer Use in Health Care Systems PDFAnonymous DlESilj50% (4)
- 1.1 Background of The StudyDocument5 pages1.1 Background of The StudySocialist GopalNo ratings yet
- New insights into treating mycoplasma without compromising egg qualityDocument2 pagesNew insights into treating mycoplasma without compromising egg qualityDrivailaNo ratings yet
- PQT Updates Egypt AUG 2018Document41 pagesPQT Updates Egypt AUG 2018KaRiM NassarNo ratings yet
- PyodermaDocument81 pagesPyodermaAtikaNo ratings yet
- PQCNC CMOP/NAS/PFE LS2 McCaffreyDocument23 pagesPQCNC CMOP/NAS/PFE LS2 McCaffreykcochranNo ratings yet
- KarunaGopal Channel6Document8 pagesKarunaGopal Channel6Ramesh GarikapatiNo ratings yet
- Genetic Testing: For Children With Autism Spectrum DisorderDocument12 pagesGenetic Testing: For Children With Autism Spectrum DisorderLalit MittalNo ratings yet
- IBS Guidelines - Cervical Cancer Brachytherapy-3Document14 pagesIBS Guidelines - Cervical Cancer Brachytherapy-3Florina SimniceanuNo ratings yet
- Asoaj MS Id 000539Document3 pagesAsoaj MS Id 000539Minh ChíNo ratings yet
- Krisis HipertensiDocument29 pagesKrisis HipertensiMuarifNo ratings yet
- Adell 1981Document30 pagesAdell 1981Raul CamargoNo ratings yet
- RX Meds 2Document3 pagesRX Meds 2Carla PulgarNo ratings yet
- EXTERNALDocument2 pagesEXTERNALMarissa AsimNo ratings yet
- National Institute of Indian Medical Heritage CatalogueDocument40 pagesNational Institute of Indian Medical Heritage CatalogueTapan Kumar MallickNo ratings yet
- Ovario Poliquístico/Polycystic Ovary SyndromeDocument14 pagesOvario Poliquístico/Polycystic Ovary SyndromeJosé María Lauricella100% (1)
- ChemotherapyDocument11 pagesChemotherapyNedaAbdullahNo ratings yet
- S 000 LBLDocument14 pagesS 000 LBLfaisal abbasNo ratings yet
- INBDEBooster Anesthetics Cheat SheetDocument1 pageINBDEBooster Anesthetics Cheat SheetSashwat SathishNo ratings yet