You might also like
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (590)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (842)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5807)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (401)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (897)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1091)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (345)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Assessment of Skin, Hair and NailsDocument65 pagesAssessment of Skin, Hair and NailsVinzii Drt100% (1)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Complementary and Alternative Systems in PsychiatryDocument131 pagesComplementary and Alternative Systems in Psychiatryganeshprabhuvk100% (1)
- Oxford Textbook of Heart Failure Oxford Textbooks in Cardiology Team Ira True PDF 2nbsped 019876622x 9780198766223Document897 pagesOxford Textbook of Heart Failure Oxford Textbooks in Cardiology Team Ira True PDF 2nbsped 019876622x 9780198766223Theerapat Chalerm-MuangNo ratings yet
- NBME Shelf Exam Sample Questions - OB GYNDocument6 pagesNBME Shelf Exam Sample Questions - OB GYNNehal LakdawalaNo ratings yet
- Pass Critical Care Endocrine Frcem ResourcesDocument41 pagesPass Critical Care Endocrine Frcem ResourcesYoussef SaadNo ratings yet
- BGSD Health IssuesDocument3 pagesBGSD Health IssuesSemi FatimaNo ratings yet
- ConjungtivitaDocument85 pagesConjungtivitaFatrisNo ratings yet
- Edit NG Drug StudyDocument35 pagesEdit NG Drug StudyAlleinad BarracasNo ratings yet
- Vibrio Cholerae That Causes CholeraDocument15 pagesVibrio Cholerae That Causes CholerayslovillanuevaNo ratings yet
- Autism As A Natural Human Variation Reflections OnDocument12 pagesAutism As A Natural Human Variation Reflections OnEnio AmekhaniaNo ratings yet
- Corona Virus PreventionDocument30 pagesCorona Virus PreventionSajad PkNo ratings yet
- Oncology TestDocument32 pagesOncology TestPhilip Gene II MalacasNo ratings yet
- 2017 Understanding-Nystagmus v04Document48 pages2017 Understanding-Nystagmus v04Stephanie AureliaNo ratings yet
- Physical Examination Till October 2017Document15 pagesPhysical Examination Till October 2017qurbanNo ratings yet
- Task 5 Sicknesses and Deseases, CWDocument6 pagesTask 5 Sicknesses and Deseases, CW2212070147 INEZ HILERY ARITONANGNo ratings yet
- The Research of Hepatitis B and Hepatitis B VaccineDocument2 pagesThe Research of Hepatitis B and Hepatitis B VaccineJerry DNo ratings yet
- Group 7 PPT COVID 19Document11 pagesGroup 7 PPT COVID 19CORCEGA JR. ARTURONo ratings yet
- National Strategic Framework For Chronic Conditions PpointDocument11 pagesNational Strategic Framework For Chronic Conditions PpointDempsey PrattNo ratings yet
- Akwa Ibom State Strategic Health Development Plan 2010-2015Document89 pagesAkwa Ibom State Strategic Health Development Plan 2010-2015Das ConsultNo ratings yet
- Congenital Anatomic AnomaliesDocument12 pagesCongenital Anatomic Anomaliesmahparah_mumtazNo ratings yet
- Screening Cancer Ibd PDFDocument8 pagesScreening Cancer Ibd PDFm_manuela2002No ratings yet
- Panic Disorder and Agoraphobia Nature and Clinical Description of The DisorderDocument5 pagesPanic Disorder and Agoraphobia Nature and Clinical Description of The DisorderAngelica Mae LimosNo ratings yet
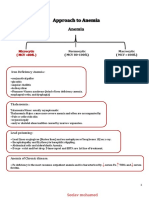
- Approach To AnemiaDocument4 pagesApproach To AnemiapNo ratings yet
- Covid PosterDocument1 pageCovid Posterarslan MaqboolNo ratings yet
- Palliative Care Guiding Principles and ResourcesDocument1 pagePalliative Care Guiding Principles and ResourcesJully TNo ratings yet
- SFA Therapeutics 12 Minute Overview Presentation 30 November 2021Document35 pagesSFA Therapeutics 12 Minute Overview Presentation 30 November 2021Ira SpectorNo ratings yet
- Final Module For THC 102 Risk Management01Document42 pagesFinal Module For THC 102 Risk Management01Alvie Mae Tecson ParaguyaNo ratings yet
- Gulati 2020Document14 pagesGulati 2020Anisha MDNo ratings yet
- New SyllabusDocument5 pagesNew SyllabusPrathamNo ratings yet
- Common Abbreviations For The Patient Note USMLE Step 2CSDocument1 pageCommon Abbreviations For The Patient Note USMLE Step 2CSTiondi francisNo ratings yet