You might also like
- Perinatal Manual of Southwestern OntarioDocument6 pagesPerinatal Manual of Southwestern OntarioƦя de GuzмѧN100% (1)
- EORCAPS 2016-Part 1Document540 pagesEORCAPS 2016-Part 1Swamynadh Gandhi Reddi100% (1)
- Endologix ELGX Updated Investor PresentationDocument18 pagesEndologix ELGX Updated Investor PresentationmedtechyNo ratings yet
- Va L4 VempDocument27 pagesVa L4 VempAfrina AzmiNo ratings yet
- Веб-страница 2Document1 pageВеб-страница 2Zalina IvanovaNo ratings yet
- Pelvic Pain - Easy 5 Step Ultrasound EvaluationDocument1 pagePelvic Pain - Easy 5 Step Ultrasound EvaluationFungai MuganhuNo ratings yet
- Cystic Kidney Diseases A Case Based Approach: ADPKD Pathogenesis Cystic PhenotypeDocument12 pagesCystic Kidney Diseases A Case Based Approach: ADPKD Pathogenesis Cystic PhenotypeMoaz TajammalNo ratings yet
- Ws12 Orthopaedic ExaminationDocument18 pagesWs12 Orthopaedic ExaminationEsther BNo ratings yet
- 876knee Disorders - 4Document19 pages876knee Disorders - 4Umut YücelNo ratings yet
- Lower Extremity PainDocument16 pagesLower Extremity PainRizki Ananda AladinNo ratings yet
- Splints in OrthodonticsDocument2 pagesSplints in Orthodonticsritu somaniNo ratings yet
- Scoliosis: Hotumese: Berkembang Dalam TantanganDocument17 pagesScoliosis: Hotumese: Berkembang Dalam TantanganNam LeeNo ratings yet
- Diagnosis in Orthodontics - Part IIIDocument38 pagesDiagnosis in Orthodontics - Part IIIkaran patelNo ratings yet
- Week 14. Spinal Cord InjuryDocument1 pageWeek 14. Spinal Cord InjuryMary Joy RoqueNo ratings yet
- Emergenze Addome RXDocument9 pagesEmergenze Addome RXBrovazzo PieroNo ratings yet
- Case Presentation 1Document4 pagesCase Presentation 1api-448765847No ratings yet
- Examination of Lacrimal ApparatusDocument16 pagesExamination of Lacrimal ApparatusSRAVYA M VNo ratings yet
- Examination of Lacrimal ApparatusDocument16 pagesExamination of Lacrimal ApparatusDr Sravya M VNo ratings yet
- Finals Ophthalmology Quizzes (Md2024)Document32 pagesFinals Ophthalmology Quizzes (Md2024)Jack Ortega PuruggananNo ratings yet
- Head Neck Osteology PDF Handout (Anatomy Decoded YouTube) PDFDocument22 pagesHead Neck Osteology PDF Handout (Anatomy Decoded YouTube) PDFNijam UdeenNo ratings yet
- TR HugesDocument91 pagesTR HugesVASUDEV SINGH SENGARNo ratings yet
- Examination: Short History Positioning of The PatientDocument1 pageExamination: Short History Positioning of The PatientAshan BopitiyaNo ratings yet
- Spine 1 Physical Exam of The SpineDocument39 pagesSpine 1 Physical Exam of The SpinePraneeth KumarNo ratings yet
- Paediatric Neurology For Emergency DeptDocument5 pagesPaediatric Neurology For Emergency Deptmalaz197No ratings yet
- Tonometry Dan PacymetriDocument9 pagesTonometry Dan PacymetriGusti Zidni FahmiNo ratings yet
- MATERI SESI 4.1 - MAR DR - HeryDocument9 pagesMATERI SESI 4.1 - MAR DR - HerydewiswahyuNo ratings yet
- Different Departments of HospitalDocument13 pagesDifferent Departments of HospitalMUKESH SUNDARARAJANNo ratings yet
- Industrial Scanners Catalog EN LTR 201506BDocument32 pagesIndustrial Scanners Catalog EN LTR 201506BDennis ChaiNo ratings yet
- HA Lec ReportDocument29 pagesHA Lec ReportRhelina MinNo ratings yet
- Getting The Most From Your Biopsies: Operator ArtifactDocument9 pagesGetting The Most From Your Biopsies: Operator ArtifactIsak ShatikaNo ratings yet
- Onli NE Case Study: I Ntroducti ON Departments - Zoni NGDocument1 pageOnli NE Case Study: I Ntroducti ON Departments - Zoni NGAnubhav KumarNo ratings yet
- Home Care RN Skills ChecklistDocument2 pagesHome Care RN Skills ChecklistGloryJaneNo ratings yet
- Orthopedic MRI (2017)Document211 pagesOrthopedic MRI (2017)Andy KidNo ratings yet
- (S. Abbate) Ear Acupuncture Prescriptions and Techniques PDFDocument8 pages(S. Abbate) Ear Acupuncture Prescriptions and Techniques PDFVenom VerdinNo ratings yet
- ATLS SkillsDocument4 pagesATLS SkillsGregahSisvanto100% (1)
- Tumors of The Head and NeckDocument5 pagesTumors of The Head and NeckMiguel CuevasNo ratings yet
- EMF Handouts Kathryn Welch MDDocument16 pagesEMF Handouts Kathryn Welch MDkomlanihou_890233161No ratings yet
- Seizures and EpilepsyDocument3 pagesSeizures and Epilepsyjoshua_villangcaNo ratings yet
- Acute Thyroid Thyroiditis Sub-Acute / Granulomatous / de Quevains's Thyroiditis Chronic / Hashimoto's Thyroiditis Fibrosing / Reidel's ThyroiditisDocument2 pagesAcute Thyroid Thyroiditis Sub-Acute / Granulomatous / de Quevains's Thyroiditis Chronic / Hashimoto's Thyroiditis Fibrosing / Reidel's ThyroiditisZuhra JabeenNo ratings yet
- Management of Grafts and Flaps PDFDocument10 pagesManagement of Grafts and Flaps PDFFiranglaniNo ratings yet
- IVT Using Infusion PumpDocument28 pagesIVT Using Infusion PumpPAOLA LUZ CRUZNo ratings yet
- Cleft Lip & Palate & Cosmetic Surgery: You GotDocument10 pagesCleft Lip & Palate & Cosmetic Surgery: You GotHa Jae kyeongNo ratings yet
- 19 Salivary GlandsDocument14 pages19 Salivary GlandsIsak Isak IsakNo ratings yet
- 1 - UTD Overhead-Protocols-2020Document5 pages1 - UTD Overhead-Protocols-2020enricNo ratings yet
- Oral Bad HabitDocument8 pagesOral Bad HabitDikiBagusNo ratings yet
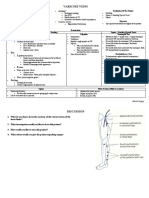
- Varicose Veins: Short History Positioning of The PatientDocument2 pagesVaricose Veins: Short History Positioning of The PatientAshan BopitiyaNo ratings yet
- N - Perineal Lac FINAL 6-Up PDFDocument5 pagesN - Perineal Lac FINAL 6-Up PDFAnisah MahmudahNo ratings yet
- HA LEC - Module 5Document22 pagesHA LEC - Module 5JAN CAMILLE LENONNo ratings yet
- Head To Toe AssessmentDocument2 pagesHead To Toe Assessmentisapatrick8126No ratings yet
- Dr. Amrita Aggarwal 1Document93 pagesDr. Amrita Aggarwal 1Pujal NayakNo ratings yet
- GI Reviewer (Updated)Document17 pagesGI Reviewer (Updated)HNo ratings yet
- LE Hip3 Intertrochanteric FracturesDocument71 pagesLE Hip3 Intertrochanteric Fracturest85yp7yv2vNo ratings yet
- Breast Cancer - Kristien JavinaDocument76 pagesBreast Cancer - Kristien JavinaKMNo ratings yet
- Adult Idiopathic Scoliosis: Prof. Dr. D. AntonescuDocument28 pagesAdult Idiopathic Scoliosis: Prof. Dr. D. AntonescuTraian UrsuNo ratings yet
- (MAPE00S) 35545-iUBT429 Unit Specification v1Document12 pages(MAPE00S) 35545-iUBT429 Unit Specification v1Chante PillayNo ratings yet
- Practical Tasks Kidneys Lesson PlanDocument4 pagesPractical Tasks Kidneys Lesson PlandfsdsfsdNo ratings yet
- Endografts For The Treatment of Abdominal Aortic ADocument15 pagesEndografts For The Treatment of Abdominal Aortic AAhmed MohammedNo ratings yet
- Proximal Abdominal EVT SupplementDocument6 pagesProximal Abdominal EVT SupplementAhmed MohammedNo ratings yet
- Cathetersandwires DrVaibhavDocument15 pagesCathetersandwires DrVaibhavAhmed MohammedNo ratings yet
- Ecr 12 1 40Document6 pagesEcr 12 1 40Ahmed MohammedNo ratings yet
- Doacs For VteDocument10 pagesDoacs For VteAhmed MohammedNo ratings yet
- DOAC VTE Treatment April2020Document4 pagesDOAC VTE Treatment April2020Ahmed MohammedNo ratings yet
- Tips and Techniques For Optimal Stent Graft Placement in Angulated Aneurysm NecksDocument6 pagesTips and Techniques For Optimal Stent Graft Placement in Angulated Aneurysm NecksAhmed MohammedNo ratings yet
- FR System - Vs Guage SystemDocument12 pagesFR System - Vs Guage SystemAhmed MohammedNo ratings yet
- Long-Term Follow-Up of Type II Endoleak Embolization Reveals The Need For Close SurveillanceDocument8 pagesLong-Term Follow-Up of Type II Endoleak Embolization Reveals The Need For Close SurveillanceAhmed MohammedNo ratings yet
- VTE Risk Assessment Tool Caprini Score Card Eng 30apr2018Document2 pagesVTE Risk Assessment Tool Caprini Score Card Eng 30apr2018Ahmed MohammedNo ratings yet
- Thromboprohylaxis and DVT in Surgical PRDocument7 pagesThromboprohylaxis and DVT in Surgical PRAhmed MohammedNo ratings yet
- Acute Pain Care PlanDocument2 pagesAcute Pain Care PlanKim Biro Turner86% (37)
- Q A6 - Allocated QuestionsDocument3 pagesQ A6 - Allocated QuestionsadishsewlallNo ratings yet
- Cordially Invite You To: The Tamilnadu DR.M.G.R Medical UniversityDocument4 pagesCordially Invite You To: The Tamilnadu DR.M.G.R Medical UniversityDamothara MuthuNo ratings yet
- PINTAKASING BANAL: Caracol Dance Competition: ObjectivesDocument2 pagesPINTAKASING BANAL: Caracol Dance Competition: ObjectivesJapeth GrayNo ratings yet
- A03 - Mr. Pratap Narayan Jaiswal - (Jaiswal Pathology) Jaiswal Pathology CC, Rajapal Chauraha, Kachehari Road, Pratapgarh, Uttar PradesDocument10 pagesA03 - Mr. Pratap Narayan Jaiswal - (Jaiswal Pathology) Jaiswal Pathology CC, Rajapal Chauraha, Kachehari Road, Pratapgarh, Uttar PradesShubham KhandelwalNo ratings yet
- Rekapitulasi Desember 2021 SipDocument555 pagesRekapitulasi Desember 2021 SipadminIHC cakramedikaNo ratings yet
- SC WD 2 TechnologyHealthConcernsPaper Report 2Document5 pagesSC WD 2 TechnologyHealthConcernsPaper Report 2Joel Lindsay100% (1)
- Clear Aligners, A Milestone in Invisible Orthodontics - A Literature ReviewDocument4 pagesClear Aligners, A Milestone in Invisible Orthodontics - A Literature ReviewInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Factor Influencing Girls Attitude Towards Breast Self-ExaminationDocument5 pagesFactor Influencing Girls Attitude Towards Breast Self-ExaminationIJAR JOURNALNo ratings yet
- Johari WindowDocument1 pageJohari WindowPrashastiNo ratings yet
- Breast ReviewDocument147 pagesBreast Reviewlovelots1234100% (1)
- Syllabus Small Bowel ObstructionDocument4 pagesSyllabus Small Bowel ObstructionHARVEY SELIM0% (1)
- Senior Thesis 2022Document19 pagesSenior Thesis 2022api-608954316No ratings yet
- Baum (2015) The New Public HealthDocument23 pagesBaum (2015) The New Public HealthjamieNo ratings yet
- Patient Medication History Interview: Dr. Vijay B. Lambole Associate Professor, SNLPCP, UmrakhDocument20 pagesPatient Medication History Interview: Dr. Vijay B. Lambole Associate Professor, SNLPCP, Umrakhvijaylambole0% (1)
- Basic Personality InventoryDocument8 pagesBasic Personality InventoryElisa Mae Oranza Gura100% (1)
- Abstract Si RezumatDocument2 pagesAbstract Si RezumatMinodora MilenaNo ratings yet
- The Self-Concept Revisited: or A Theory of A TheoryDocument13 pagesThe Self-Concept Revisited: or A Theory of A TheoryShams JhugrooNo ratings yet
- Family Assessment 2 (Interview)Document5 pagesFamily Assessment 2 (Interview)DIZZA MAE BATURIANONo ratings yet
- Traditional Ancient Egyptian MedicineDocument10 pagesTraditional Ancient Egyptian MedicinebazediNo ratings yet
- DR AP - BREATHING TECHNIQUES (2020v2)Document11 pagesDR AP - BREATHING TECHNIQUES (2020v2)Dr Adele PelteretNo ratings yet
- DVT And/or PE Treatment Dosage For Tinzaparin (Innohep®)Document1 pageDVT And/or PE Treatment Dosage For Tinzaparin (Innohep®)Kok Hui DiongNo ratings yet
- Traditional Chinese Medicine in Taiwan 2021-7-6Document23 pagesTraditional Chinese Medicine in Taiwan 2021-7-6yandi permanaNo ratings yet
- NAP4 Summary SheetDocument1 pageNAP4 Summary SheetAnonymous w4lLoMd7No ratings yet
- Body Piercing and Tattoos: A Survey On Young Adults ' Knowledge of The Risks and Practices in Body ArtDocument8 pagesBody Piercing and Tattoos: A Survey On Young Adults ' Knowledge of The Risks and Practices in Body ArtIliana StrahilovaNo ratings yet
- Journal of Interventional Medicine: Yanli Wang, Guohao Huang, Tian Jiang, Xinwei HanDocument5 pagesJournal of Interventional Medicine: Yanli Wang, Guohao Huang, Tian Jiang, Xinwei HanDzulRizkaNo ratings yet
- May 15, 2023 - AssignmentDocument6 pagesMay 15, 2023 - AssignmentMARY FORTUNE MAE RAMONESNo ratings yet
- 4th Week Final ManagementDocument25 pages4th Week Final ManagementJAN LYKA RESURRECCIONNo ratings yet
- Colourism in Asia PacificDocument5 pagesColourism in Asia PacificFozan AhmedNo ratings yet
- Disaster Victim Identification (Dvi)Document20 pagesDisaster Victim Identification (Dvi)gennysuwandiNo ratings yet