You might also like
- Respiratory Tract InfectionsDocument1 pageRespiratory Tract InfectionsShannon RamsumairNo ratings yet
- CroupDocument20 pagesCroupFariezuan HamidNo ratings yet
- Pedia Rotation CroupDocument2 pagesPedia Rotation CroupKaren ArandiaNo ratings yet
- Nursing CS CroupDocument1 pageNursing CS Croupreuben kadarajaNo ratings yet
- Two in One Disease: Asthma: Respiratory Disease That Can Have AttackDocument50 pagesTwo in One Disease: Asthma: Respiratory Disease That Can Have AttackkeiylumbantoruanNo ratings yet
- CROUP Concept MapDocument3 pagesCROUP Concept Mapingrid50% (2)
- EMD2 - K8 - Acute Severe Asthma AttackDocument34 pagesEMD2 - K8 - Acute Severe Asthma AttackJessica WijayaNo ratings yet
- NRSG 206 Croup SyndromeDocument3 pagesNRSG 206 Croup SyndromeGirlwithnonameNo ratings yet
- Communicable Diseases Infectious Diseases and Hematologic DrugDocument26 pagesCommunicable Diseases Infectious Diseases and Hematologic DrugAdrian LesiguesNo ratings yet
- CS4 Asthma Drug StudyDocument10 pagesCS4 Asthma Drug StudyAudrie Allyson GabalesNo ratings yet
- Name of Drug Classificatio N Mechanism of Action Indications Contraindication S Adverse Effects Side EffectsDocument7 pagesName of Drug Classificatio N Mechanism of Action Indications Contraindication S Adverse Effects Side EffectsHilario. Hayascent.Reign.M.No ratings yet
- BBB - Respi&gi ReportsDocument11 pagesBBB - Respi&gi ReportsshesahNo ratings yet
- Formal Evaluation of Asthma Exacerbation Severity in The Urgent or Emergency CarDocument3 pagesFormal Evaluation of Asthma Exacerbation Severity in The Urgent or Emergency Carمعاذ الشريفNo ratings yet
- Adventitious Breath SoundsDocument1 pageAdventitious Breath SoundsAbdullah BhattiNo ratings yet
- Management of Asthma Attacks in Childhood AsthmaDocument43 pagesManagement of Asthma Attacks in Childhood AsthmaGilankNo ratings yet
- Pulmonary-Tuberculosis - NCPDocument5 pagesPulmonary-Tuberculosis - NCPMae Therese B. MAGNONo ratings yet
- Medications Before DeliveryDocument5 pagesMedications Before DeliveryCarlyn AguasNo ratings yet
- Cold Vs Flu Vs Allergies Vs Coronavirus PDFDocument1 pageCold Vs Flu Vs Allergies Vs Coronavirus PDFDavid HoreshNo ratings yet
- Certify Baby'S Birth: Body TemperatureDocument9 pagesCertify Baby'S Birth: Body TemperatureJobelle Acena100% (1)
- M2 POST TASK - Scarlet Fever (Stomatitis Scarlatina)Document2 pagesM2 POST TASK - Scarlet Fever (Stomatitis Scarlatina)FRANCHEZKA ANGELICA TANIEGRANo ratings yet
- DRUG STUDY (Shortness of Breath)Document2 pagesDRUG STUDY (Shortness of Breath)Michelle VillanuevaNo ratings yet
- RHINITISDocument3 pagesRHINITISErika Mae Sta. MariaNo ratings yet
- Paediatric Respiratory Assessment Cheat Sheet: by ViaDocument1 pagePaediatric Respiratory Assessment Cheat Sheet: by ViaReihann N. EdresNo ratings yet
- AcuteCoughInChild PDFDocument1 pageAcuteCoughInChild PDFstudzillaNo ratings yet
- Pertusis: - Also Known As TB o oDocument2 pagesPertusis: - Also Known As TB o oKrizle AdazaNo ratings yet
- Asthma 1Document79 pagesAsthma 1DanishMandiNo ratings yet
- Paeds - Bronchiolitis, Pneumonia, PertussisDocument3 pagesPaeds - Bronchiolitis, Pneumonia, PertussisVicnaraj VicNo ratings yet
- Bronchiolitis: See AlsoDocument6 pagesBronchiolitis: See AlsoJuleides De LeonNo ratings yet
- Emergency Causes Signs and Symtomps Management NoteDocument5 pagesEmergency Causes Signs and Symtomps Management NoteAna Victoria JiménezNo ratings yet
- 19penyusunnan Dan Kegunaan LksDocument1 page19penyusunnan Dan Kegunaan LksImam HakamNo ratings yet
- Ent Guidelines New 020616Document15 pagesEnt Guidelines New 020616Osasere EwekaNo ratings yet
- Pathophysiology of PneumoniaDocument2 pagesPathophysiology of PneumoniaJuneNo ratings yet
- Respiratory Sounds: by Oluwaseun OlaiyaDocument16 pagesRespiratory Sounds: by Oluwaseun OlaiyaOlaiya OluwaseunNo ratings yet
- Drug StudyDocument1 pageDrug StudyElisha Faith Sevilla EspineliNo ratings yet
- Table - Respiratory - Bacterial, Viral Fungal InfectionsDocument9 pagesTable - Respiratory - Bacterial, Viral Fungal InfectionsSondos MohammadNo ratings yet
- Finals LecDocument14 pagesFinals LecSheena Patricia ArasulaNo ratings yet
- COVID - Management 14 April 2021Document20 pagesCOVID - Management 14 April 2021Zain ZaidiNo ratings yet
- Drug-Ana 4Document14 pagesDrug-Ana 4Florante AnibanNo ratings yet
- Respiratory PathophysDocument1 pageRespiratory PathophysTori IkeharaNo ratings yet
- Drug StudyDocument5 pagesDrug Studyeizhel8No ratings yet
- DRUG-STUDY-FORMAT-Binangonan Lakeview 3rdDocument2 pagesDRUG-STUDY-FORMAT-Binangonan Lakeview 3rdDianne UlandayNo ratings yet
- Name of DrugDocument5 pagesName of DrugJoann BeriñoNo ratings yet
- Blue and Mint Green Pattern Science Fair BrochureDocument2 pagesBlue and Mint Green Pattern Science Fair BrochureJohn Ray GamboaNo ratings yet
- Cold vs. Flu vs. Allergies vs. COVID-19Document1 pageCold vs. Flu vs. Allergies vs. COVID-19prabuNo ratings yet
- Kuliah AsmaattackDocument43 pagesKuliah AsmaattacksusnariahmadNo ratings yet
- Congenital Anomalies Associated With Stridor - UpToDateDocument2 pagesCongenital Anomalies Associated With Stridor - UpToDateBrillence M SammyNo ratings yet
- Abnormal Lung Sounds v2Document1 pageAbnormal Lung Sounds v2Ynah BellaNo ratings yet
- Drug PresentationDocument4 pagesDrug Presentationchaudharitrushar007No ratings yet
- Equine ReviewerDocument27 pagesEquine ReviewerWenn Marc Catuiran DuceNo ratings yet
- Glossopharyngeal Nerve (IX) : Anatomy 1) Nose LaryngospasmDocument8 pagesGlossopharyngeal Nerve (IX) : Anatomy 1) Nose LaryngospasmSally DoonNo ratings yet
- Inspection Palpation Percussio N Auscult Ation Other Findin Gs InterpretationDocument12 pagesInspection Palpation Percussio N Auscult Ation Other Findin Gs InterpretationLieza Mae LlanosNo ratings yet
- Pathophysiology HemothoraxDocument1 pagePathophysiology HemothoraxCA SavageNo ratings yet
- Drug StudyDocument1 pageDrug StudyKristine Marie YlayaNo ratings yet
- PE - Pulmonary EmbolismDocument1 pagePE - Pulmonary EmbolismvishalmakadiaNo ratings yet
- Drugs Case StudyDocument2 pagesDrugs Case StudyGwen De CastroNo ratings yet
- SPM Record Sticking PicDocument7 pagesSPM Record Sticking PicZaid AhmadNo ratings yet
- Bot Med Final CHARTDocument33 pagesBot Med Final CHARTapi-26938624100% (3)
- Type 1 DiabetesDocument6 pagesType 1 DiabetesKehoe MathsNo ratings yet
- Type 2 DiabetesDocument4 pagesType 2 DiabetesKehoe MathsNo ratings yet
- Type 1 DiabetesDocument5 pagesType 1 DiabetesKehoe MathsNo ratings yet
- ECT 4th Med Lecture 2020Document36 pagesECT 4th Med Lecture 2020Kehoe MathsNo ratings yet
- PSYC 444 Sleep Mechanisms and Behaviour Fall 2021 SyllabusDocument9 pagesPSYC 444 Sleep Mechanisms and Behaviour Fall 2021 SyllabusSunnyNo ratings yet
- Energy Conversion and Management: He Wang, Guofang Gong, Hongbin Zhou, Wei WangDocument10 pagesEnergy Conversion and Management: He Wang, Guofang Gong, Hongbin Zhou, Wei Wangbryan andres mora ramosNo ratings yet
- Heirs of Ypon v. Ricaforte (G.R. No. 198680)Document2 pagesHeirs of Ypon v. Ricaforte (G.R. No. 198680)Hershey Delos SantosNo ratings yet
- MnemonicsDocument1 pageMnemonicscoaneu6No ratings yet
- PBR-005-HandoutC - FillableDocument2 pagesPBR-005-HandoutC - FillableMollyanna StephensNo ratings yet
- Pest Analysis For PadiniDocument13 pagesPest Analysis For PadiniInnocent Diana50% (2)
- MEDDEV 2 - 7 - 1 - Rev4 - enDocument65 pagesMEDDEV 2 - 7 - 1 - Rev4 - enSalvatore CannataNo ratings yet
- Accompanist WebinarDocument17 pagesAccompanist WebinarzramarioNo ratings yet
- MCP9801Document30 pagesMCP9801alvaldez035981100% (1)
- Self Can Be Viewed Into Two Distinct BeingDocument3 pagesSelf Can Be Viewed Into Two Distinct BeingVinabie PunoNo ratings yet
- Computer Based Examination: A Project Report ONDocument7 pagesComputer Based Examination: A Project Report ONSalman RazaNo ratings yet
- Buku Saku Icd 9, RSGM Unair-1Document21 pagesBuku Saku Icd 9, RSGM Unair-1riris roselinaNo ratings yet
- Gibraltar: This Article Is About The British Overseas Territory. For Other Uses, SeeDocument31 pagesGibraltar: This Article Is About The British Overseas Territory. For Other Uses, SeealinaNo ratings yet
- 11th Physics Vol.1 Model Question Paper English MediumDocument3 pages11th Physics Vol.1 Model Question Paper English Mediumsudha venkat yoga vigneshNo ratings yet
- ImagineFX 2018 156 JanuaryDocument116 pagesImagineFX 2018 156 JanuaryResimasc González100% (5)
- Capillary Puncture (Materials and Procedure)Document36 pagesCapillary Puncture (Materials and Procedure)Angelica Camille B. AbaoNo ratings yet
- KPC: Klebsiella Pneumoniae Carbapenemasa, Principal Carbapenemasa en EnterobacteriasDocument9 pagesKPC: Klebsiella Pneumoniae Carbapenemasa, Principal Carbapenemasa en EnterobacteriasGarcia RosaNo ratings yet
- Uh 1Document358 pagesUh 1Marco AlfieriNo ratings yet
- TF-4 Venturi Meter Lab Report Group HDocument10 pagesTF-4 Venturi Meter Lab Report Group HAiman fakriNo ratings yet
- A Case Study On AmeobiasisDocument34 pagesA Case Study On AmeobiasisKhemz Dalde LimNo ratings yet
- Play 100+ Songs With 5 Common Chord Progressions For GuitarDocument1 pagePlay 100+ Songs With 5 Common Chord Progressions For GuitarNestor Cantilang MalinaoNo ratings yet
- KSSR Year 5 Chapter 7 Although SinceDocument2 pagesKSSR Year 5 Chapter 7 Although Sinceloucheng100% (1)
- Main Individual Assignment On Organization Description: Submitted byDocument7 pagesMain Individual Assignment On Organization Description: Submitted byakkksssNo ratings yet
- Past Simple WorksheetsDocument4 pagesPast Simple WorksheetsSumaira KhanNo ratings yet
- SopDocument3 pagesSopKisna Bhurtel0% (1)
- Inventory ManagementDocument46 pagesInventory ManagementASHOK SUTHARNo ratings yet
- Understanding The Consumer Preferences: AcknowledgmentDocument14 pagesUnderstanding The Consumer Preferences: AcknowledgmentfareedahsanNo ratings yet
- Case Study XIIDocument3 pagesCase Study XIIPhoenix The actorNo ratings yet
- BMO0272 Week 2 Workshop SlidesDocument21 pagesBMO0272 Week 2 Workshop Slideskenechi lightNo ratings yet
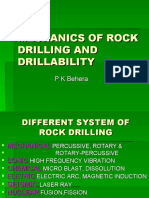
- Rock Drilling and DrillabilityDocument57 pagesRock Drilling and Drillabilitybishal pradhan0% (1)