You might also like
- Hypertension in Children and Adolescents: New PerspectivesFrom EverandHypertension in Children and Adolescents: New PerspectivesEmpar LurbeNo ratings yet
- Hypertension During PregnancyDocument9 pagesHypertension During PregnancyNera MayaditaNo ratings yet
- Preeclampsia/Eclampsia: An Insight Into The Dilemma of Treatment by The AnesthesiologistDocument10 pagesPreeclampsia/Eclampsia: An Insight Into The Dilemma of Treatment by The AnesthesiologistAnonymous kltUTaNo ratings yet
- Hypertensive Disorders of PregnancyDocument10 pagesHypertensive Disorders of PregnancyKrishna G Duran AguilarNo ratings yet
- Best Practices For Managing Postpartum HypertensionDocument10 pagesBest Practices For Managing Postpartum HypertensionYhogerlys LucenaNo ratings yet
- Managing Post Partum HypertensionDocument10 pagesManaging Post Partum HypertensionDendyNo ratings yet
- 10.1007@s11906 020 01058 WDocument11 pages10.1007@s11906 020 01058 WMauricio Lopez MejiaNo ratings yet
- Trastornos Hipertensivos Del EmbarazoDocument10 pagesTrastornos Hipertensivos Del EmbarazoAnelGarciaNo ratings yet
- Hypertension in Pregnancy: Diagnosis and ManagementDocument10 pagesHypertension in Pregnancy: Diagnosis and ManagementDinorah MarcelaNo ratings yet
- Pi Is 0002937820312837Document13 pagesPi Is 0002937820312837Manuel MagañaNo ratings yet
- J Am Heart Assoc 2014 NannaDocument19 pagesJ Am Heart Assoc 2014 NannaBagus Wanda HabibullahNo ratings yet
- Pregnancy Induced Hypertension PIH BeyonDocument2 pagesPregnancy Induced Hypertension PIH Beyonvictorubong404No ratings yet
- Trastornos HIPERTENSIVOSDocument14 pagesTrastornos HIPERTENSIVOSIvan CastellanosNo ratings yet
- Differentiating Between Gestational and Chronic Hyper-Tension An Explorative StudyDocument6 pagesDifferentiating Between Gestational and Chronic Hyper-Tension An Explorative StudyVera Gardasevic MitrovicNo ratings yet
- Desorden Hipertensivo en El EmbarazoDocument12 pagesDesorden Hipertensivo en El EmbarazoAntonio AlonsoNo ratings yet
- Emergencias HAS en EmbarazoDocument13 pagesEmergencias HAS en EmbarazoLuis Soriano MitraNo ratings yet
- Hipertension en El EmbarazoDocument12 pagesHipertension en El EmbarazofsitoNo ratings yet
- Chronic Hypertension in Pregnancy: Clinical PracticeDocument8 pagesChronic Hypertension in Pregnancy: Clinical PracticeemmoyNo ratings yet
- Preeclampsia, A New Perspective in 2011: M S S M. S - SDocument10 pagesPreeclampsia, A New Perspective in 2011: M S S M. S - SharyatikennitaNo ratings yet
- Chronic Hypertension in Pregnancy: Clinical PracticeDocument8 pagesChronic Hypertension in Pregnancy: Clinical PracticecornelNo ratings yet
- Preeclampsia and EclampsiaDocument7 pagesPreeclampsia and Eclampsiagail_gulmaticoNo ratings yet
- Hypertension in Pregnancy Vest2014 PDFDocument11 pagesHypertension in Pregnancy Vest2014 PDFjuan perezNo ratings yet
- New Aspects in The Pathophysiology of Preeclampsia: Clinical ScienceDocument27 pagesNew Aspects in The Pathophysiology of Preeclampsia: Clinical Sciencenaumee100% (2)
- Dines 2020 ACKD Hypertensive Disorders of PregnancyDocument9 pagesDines 2020 ACKD Hypertensive Disorders of PregnancyBCR ABLNo ratings yet
- JAH3 10 E018155Document22 pagesJAH3 10 E018155Priscilla AdetiNo ratings yet
- Cardiac Diastolic Function After Recovery From Pre-EclampsiaDocument6 pagesCardiac Diastolic Function After Recovery From Pre-EclampsiaLannydchandraNo ratings yet
- D2 Hormones-211Document37 pagesD2 Hormones-211ari naNo ratings yet
- GHTNDocument6 pagesGHTNDelavemia RostianiNo ratings yet
- Desrodenes Hiptertensivos Del EmbarazoDocument8 pagesDesrodenes Hiptertensivos Del EmbarazoLuis Hernan Guerrero LoaizaNo ratings yet
- IntroductionDocument8 pagesIntroductionpuspaNo ratings yet
- Pregnancy in WomenDocument7 pagesPregnancy in WomenAlika MaharaniNo ratings yet
- Hypertension in PregnancyDocument5 pagesHypertension in PregnancyVammy Beverly ValentineNo ratings yet
- Diagnosis and Management of PreeclampsiaDocument9 pagesDiagnosis and Management of PreeclampsiaEka YogaNo ratings yet
- Summary of The NHLBI Working Group On Research On Hypertension During PregnancyDocument9 pagesSummary of The NHLBI Working Group On Research On Hypertension During PregnancycarlosarmijoNo ratings yet
- Valvular Heart Disease Management in PregnancyDocument13 pagesValvular Heart Disease Management in PregnancyGlenn Alend Wowor GlennNo ratings yet
- Modern management of postnatal hypertensionDocument6 pagesModern management of postnatal hypertensionRegina MeliaNo ratings yet
- Etiology and Management of Postpartum Hypertension-PreeclampsiaDocument9 pagesEtiology and Management of Postpartum Hypertension-PreeclampsiaJoviantoReynoldAndikaHidayatNo ratings yet
- The Management of Hypertension in Women Planning For PregnancyDocument10 pagesThe Management of Hypertension in Women Planning For PregnancyRadinal PrayitnoNo ratings yet
- Pregnancy and Cardiovascular DiseaseDocument14 pagesPregnancy and Cardiovascular DiseaseDuy Nguyen CongNo ratings yet
- AHA HypertensionDocument6 pagesAHA HypertensionTry Zetyo WibowoNo ratings yet
- Circimaging. 2021Document13 pagesCircimaging. 2021Alejandra PinillaNo ratings yet
- Association Between Heart Disease in Pregnancy With Cardiac EventsDocument7 pagesAssociation Between Heart Disease in Pregnancy With Cardiac EventsAsri Mukti NantaNo ratings yet
- Effect of Early Onset Preeclampsia On Cardiovascular Risk in The Fifth Decade of Life - 2017 - American Journal of Obstetrics and Gynecology PDFDocument7 pagesEffect of Early Onset Preeclampsia On Cardiovascular Risk in The Fifth Decade of Life - 2017 - American Journal of Obstetrics and Gynecology PDFfujimeisterNo ratings yet
- 2016 Chronic Hypertension in PregnancyDocument13 pages2016 Chronic Hypertension in PregnancydkasisNo ratings yet
- Kahn 1998Document3 pagesKahn 1998Sheila Regina TizaNo ratings yet
- Cardiovascular Disease and Hypertensive Disorders of PregnancyDocument2 pagesCardiovascular Disease and Hypertensive Disorders of Pregnancyyanco pajaroNo ratings yet
- PREECLAMPSIADocument14 pagesPREECLAMPSIAFabiolaGodoyNo ratings yet
- Cek PlagiarismDocument9 pagesCek PlagiarismzzooooeeeeeeNo ratings yet
- Maternal Hemodynamics: A Method To Classify Hypertensive Disorders of PregnancyDocument23 pagesMaternal Hemodynamics: A Method To Classify Hypertensive Disorders of PregnancyaulianmediansyahNo ratings yet
- BJOG - 2020 - Perry - Maternal Haemodynamic Function Differs in Pre Eclampsia When It Is Associated With ADocument9 pagesBJOG - 2020 - Perry - Maternal Haemodynamic Function Differs in Pre Eclampsia When It Is Associated With AHanifa W PNo ratings yet
- Pregnancy-Related Hypertension: Subdept. of Obstetrics & Gynecology Dr. Ramelan Indonesian Naval Hospital SurabayaDocument33 pagesPregnancy-Related Hypertension: Subdept. of Obstetrics & Gynecology Dr. Ramelan Indonesian Naval Hospital SurabayaSurya Nirmala DewiNo ratings yet
- Keywords: Pre-Eclampsia, Diagnosis, Risk Factors, Complications, Management, AnesthesiaDocument14 pagesKeywords: Pre-Eclampsia, Diagnosis, Risk Factors, Complications, Management, AnesthesiaAyu W. AnggreniNo ratings yet
- Preeclampsia - Clinical Features and Diagnosis - UpToDateDocument38 pagesPreeclampsia - Clinical Features and Diagnosis - UpToDateSlayerNo ratings yet
- Cardiac Disease in PregnancyDocument19 pagesCardiac Disease in PregnancyCarolina Orjuela Camargo0% (1)
- Management Postpartum Hyperten PreeclampsiaDocument6 pagesManagement Postpartum Hyperten Preeclampsiaade_liaNo ratings yet
- Journal Reading - Cardiac in PregnancyDocument9 pagesJournal Reading - Cardiac in PregnancyDimes Atika PermanasariNo ratings yet
- Pregnancy Induced Hypertension Case StudyDocument54 pagesPregnancy Induced Hypertension Case Studysupernurse02No ratings yet
- Hypertension and Management: Preeclampsia: Pathophysiology and The Maternal-Fetal RiskDocument5 pagesHypertension and Management: Preeclampsia: Pathophysiology and The Maternal-Fetal RiskMarest AskynaNo ratings yet
- Etiology and Management of Postpartum Hypertension-PreeclampsiaDocument6 pagesEtiology and Management of Postpartum Hypertension-Preeclampsiasaidbenmokhtar3960No ratings yet
- Management of HypertensionDocument6 pagesManagement of HypertensionRioNo ratings yet
- Role Play Moving Patient From Bed To WheelchairDocument2 pagesRole Play Moving Patient From Bed To WheelchairDevina RahmaNo ratings yet
- OSCE Checklist Peripheral Vascular ExaminationDocument2 pagesOSCE Checklist Peripheral Vascular ExaminationKerlida SantosNo ratings yet
- DVLA Regulations For Patients With ICDs-July2015 - WebDocument2 pagesDVLA Regulations For Patients With ICDs-July2015 - WebomarNo ratings yet
- NMC CBT Mock Test 6Document14 pagesNMC CBT Mock Test 6Charles Osiako100% (1)
- George Rooks - Can't Stop TalkingDocument57 pagesGeorge Rooks - Can't Stop TalkingSergio AngeloroNo ratings yet
- Nursing Care Plan For Doppler Scan and Stress TestingDocument10 pagesNursing Care Plan For Doppler Scan and Stress TestingAmy Rose AbuevaNo ratings yet
- Dte-1 Lab RecordDocument85 pagesDte-1 Lab Recordpraveena raviNo ratings yet
- Neuromonitoring in Critically Ill Patients.9Document18 pagesNeuromonitoring in Critically Ill Patients.9Israel Villalba FonsecaNo ratings yet
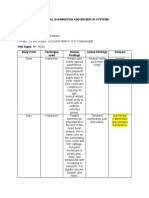
- Physical Exam Review of Systems Finds Underweight Teen with Pitted TeethDocument4 pagesPhysical Exam Review of Systems Finds Underweight Teen with Pitted TeethMark Nel NuñezNo ratings yet
- AERO144 Info 1Document3 pagesAERO144 Info 173wNo ratings yet
- Mitral Regurgitation: Jacqueline Suk Danik,, and Bernard E. BulwerDocument30 pagesMitral Regurgitation: Jacqueline Suk Danik,, and Bernard E. Bulwerhawk.man8No ratings yet
- Should Norepinephrine, Rather Than PhenylephrineDocument8 pagesShould Norepinephrine, Rather Than PhenylephrineDiego Andres Rojas TejadaNo ratings yet
- Kunwor Bishal Neuro Case 1Document12 pagesKunwor Bishal Neuro Case 1Bishal JB KunworNo ratings yet
- Electrophysiological Foundations of Cardiac Arrhythmias - A Bridge Between Basic Mechanisms and Clinical Electrophysiology (PDFDrive)Document689 pagesElectrophysiological Foundations of Cardiac Arrhythmias - A Bridge Between Basic Mechanisms and Clinical Electrophysiology (PDFDrive)drdpkrimsNo ratings yet
- Cutaneous Circulation: DR Pushpa Lata Sachan Associate Professor CIMS&H, LucknowDocument19 pagesCutaneous Circulation: DR Pushpa Lata Sachan Associate Professor CIMS&H, LucknowNishankumar JhaNo ratings yet
- AHA ACLS Megacode ScenariosDocument6 pagesAHA ACLS Megacode ScenariosVitor Hugo G Correia86% (7)
- ALS Provider Course: European Resuscitation Council (ERC) & Egyptian Resuscitation Council (EGRC)Document3 pagesALS Provider Course: European Resuscitation Council (ERC) & Egyptian Resuscitation Council (EGRC)Amr OthmanNo ratings yet
- Peripheral Vascular Disease Arteries NHSDocument10 pagesPeripheral Vascular Disease Arteries NHSAdahl HetheringtonNo ratings yet
- Terapia Multimodal Con Vasopresores en Shock Septico 2023Document11 pagesTerapia Multimodal Con Vasopresores en Shock Septico 2023CESAR AUGUSTO AUCCACUSI RODRIGUEZNo ratings yet
- Mec-1200 VetDocument2 pagesMec-1200 VetVinsmoke SanjiNo ratings yet
- Case Study About Hypertension With Electrolyte Imbalance Part 3Document2 pagesCase Study About Hypertension With Electrolyte Imbalance Part 3THE NURSING CORNERS100% (1)
- Lec Activity11 and 13 Blood Blood VesselDocument2 pagesLec Activity11 and 13 Blood Blood Vesselapple BananaNo ratings yet
- Venous Thromboembolism DiseaseDocument49 pagesVenous Thromboembolism DiseaseNiko YuandikaNo ratings yet
- Examination of PlacentaDocument2 pagesExamination of PlacentaAnju MargaretNo ratings yet
- EKG/ECG Study GuideDocument13 pagesEKG/ECG Study GuideSherree HayesNo ratings yet
- A Case Study of Hypertensive Cardiovascular Disease (HCVD) : School of Nursing and MidwiferyDocument13 pagesA Case Study of Hypertensive Cardiovascular Disease (HCVD) : School of Nursing and Midwiferyhsiria100% (2)
- PED001-M2FEM - Dialoma (Activity 1)Document7 pagesPED001-M2FEM - Dialoma (Activity 1)Ching DialomaNo ratings yet
- Heart - Anatomy and FunctionDocument13 pagesHeart - Anatomy and FunctionAlok KumarNo ratings yet
- Policy For Resuscitation TrainingDocument54 pagesPolicy For Resuscitation TrainingSyed Mohamad Amirul SyafiqNo ratings yet
- FAPC Exercise PhysioDocument2 pagesFAPC Exercise Physiom65ytmtqxmNo ratings yet
- LIT: Life Ignition Tools: Use Nature's Playbook to Energize Your Brain, Spark Ideas, and Ignite ActionFrom EverandLIT: Life Ignition Tools: Use Nature's Playbook to Energize Your Brain, Spark Ideas, and Ignite ActionRating: 4 out of 5 stars4/5 (402)
- The Age of Magical Overthinking: Notes on Modern IrrationalityFrom EverandThe Age of Magical Overthinking: Notes on Modern IrrationalityRating: 4 out of 5 stars4/5 (14)
- Summary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedFrom EverandSummary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedRating: 5 out of 5 stars5/5 (78)
- Why We Die: The New Science of Aging and the Quest for ImmortalityFrom EverandWhy We Die: The New Science of Aging and the Quest for ImmortalityRating: 3.5 out of 5 stars3.5/5 (2)
- Raising Mentally Strong Kids: How to Combine the Power of Neuroscience with Love and Logic to Grow Confident, Kind, Responsible, and Resilient Children and Young AdultsFrom EverandRaising Mentally Strong Kids: How to Combine the Power of Neuroscience with Love and Logic to Grow Confident, Kind, Responsible, and Resilient Children and Young AdultsRating: 5 out of 5 stars5/5 (1)
- By the Time You Read This: The Space between Cheslie's Smile and Mental Illness—Her Story in Her Own WordsFrom EverandBy the Time You Read This: The Space between Cheslie's Smile and Mental Illness—Her Story in Her Own WordsNo ratings yet
- Raising Good Humans: A Mindful Guide to Breaking the Cycle of Reactive Parenting and Raising Kind, Confident KidsFrom EverandRaising Good Humans: A Mindful Guide to Breaking the Cycle of Reactive Parenting and Raising Kind, Confident KidsRating: 4.5 out of 5 stars4.5/5 (169)
- Think This, Not That: 12 Mindshifts to Breakthrough Limiting Beliefs and Become Who You Were Born to BeFrom EverandThink This, Not That: 12 Mindshifts to Breakthrough Limiting Beliefs and Become Who You Were Born to BeNo ratings yet
- Techniques Exercises And Tricks For Memory ImprovementFrom EverandTechniques Exercises And Tricks For Memory ImprovementRating: 4.5 out of 5 stars4.5/5 (40)
- Outlive: The Science and Art of Longevity by Peter Attia: Key Takeaways, Summary & AnalysisFrom EverandOutlive: The Science and Art of Longevity by Peter Attia: Key Takeaways, Summary & AnalysisRating: 4 out of 5 stars4/5 (1)
- The Obesity Code: Unlocking the Secrets of Weight LossFrom EverandThe Obesity Code: Unlocking the Secrets of Weight LossRating: 5 out of 5 stars5/5 (4)
- The Ritual Effect: From Habit to Ritual, Harness the Surprising Power of Everyday ActionsFrom EverandThe Ritual Effect: From Habit to Ritual, Harness the Surprising Power of Everyday ActionsRating: 3.5 out of 5 stars3.5/5 (3)
- Summary: Outlive: The Science and Art of Longevity by Peter Attia MD, With Bill Gifford: Key Takeaways, Summary & AnalysisFrom EverandSummary: Outlive: The Science and Art of Longevity by Peter Attia MD, With Bill Gifford: Key Takeaways, Summary & AnalysisRating: 4.5 out of 5 stars4.5/5 (42)
- The Ultimate Guide To Memory Improvement TechniquesFrom EverandThe Ultimate Guide To Memory Improvement TechniquesRating: 5 out of 5 stars5/5 (34)
- Roxane Gay & Everand Originals: My Year of Psychedelics: Lessons on Better LivingFrom EverandRoxane Gay & Everand Originals: My Year of Psychedelics: Lessons on Better LivingRating: 5 out of 5 stars5/5 (5)
- The Happiness Trap: How to Stop Struggling and Start LivingFrom EverandThe Happiness Trap: How to Stop Struggling and Start LivingRating: 4 out of 5 stars4/5 (1)
- Dark Psychology & Manipulation: Discover How To Analyze People and Master Human Behaviour Using Emotional Influence Techniques, Body Language Secrets, Covert NLP, Speed Reading, and Hypnosis.From EverandDark Psychology & Manipulation: Discover How To Analyze People and Master Human Behaviour Using Emotional Influence Techniques, Body Language Secrets, Covert NLP, Speed Reading, and Hypnosis.Rating: 4.5 out of 5 stars4.5/5 (110)
- The Garden Within: Where the War with Your Emotions Ends and Your Most Powerful Life BeginsFrom EverandThe Garden Within: Where the War with Your Emotions Ends and Your Most Powerful Life BeginsNo ratings yet
- Mindset by Carol S. Dweck - Book Summary: The New Psychology of SuccessFrom EverandMindset by Carol S. Dweck - Book Summary: The New Psychology of SuccessRating: 4.5 out of 5 stars4.5/5 (327)
- The Courage Habit: How to Accept Your Fears, Release the Past, and Live Your Courageous LifeFrom EverandThe Courage Habit: How to Accept Your Fears, Release the Past, and Live Your Courageous LifeRating: 4.5 out of 5 stars4.5/5 (253)
- Roxane Gay & Everand Originals: My Year of Psychedelics: Lessons on Better LivingFrom EverandRoxane Gay & Everand Originals: My Year of Psychedelics: Lessons on Better LivingRating: 3.5 out of 5 stars3.5/5 (33)
- Daniel Kahneman's "Thinking Fast and Slow": A Macat AnalysisFrom EverandDaniel Kahneman's "Thinking Fast and Slow": A Macat AnalysisRating: 3.5 out of 5 stars3.5/5 (130)
- Summary: It Didn't Start with You: How Inherited Family Trauma Shapes Who We Are and How to End the Cycle By Mark Wolynn: Key Takeaways, Summary & AnalysisFrom EverandSummary: It Didn't Start with You: How Inherited Family Trauma Shapes Who We Are and How to End the Cycle By Mark Wolynn: Key Takeaways, Summary & AnalysisRating: 5 out of 5 stars5/5 (3)