You might also like
- Clinical Skill ScriptDocument12 pagesClinical Skill Scriptannoying fuckerNo ratings yet
- Physical Exam ChecklistDocument2 pagesPhysical Exam ChecklistRaisah Bint Abdullah100% (5)
- 12 Acup Pts Save LifeDocument7 pages12 Acup Pts Save LifefreimannNo ratings yet
- Complete Physical ExamDocument10 pagesComplete Physical ExamSohayb Abu TabanjehNo ratings yet
- Spine ExaminationDocument30 pagesSpine ExaminationNadia SalwaniNo ratings yet
- UCLA Fundamentals of Clinical Medicine Physical Exam Skills Checklist Student - GroupDocument5 pagesUCLA Fundamentals of Clinical Medicine Physical Exam Skills Checklist Student - GroupAmira AttyaNo ratings yet
- Physical Exam & Interview ChecklistDocument7 pagesPhysical Exam & Interview Checklistjmosser100% (6)
- Doctor-patient physical exam guideDocument2 pagesDoctor-patient physical exam guideAnonymous fj68MsNo ratings yet
- Respiratory Examination GuideDocument4 pagesRespiratory Examination Guiderhea100% (2)
- Chest, Back, Shoulder and Leg Workout RoutineDocument2 pagesChest, Back, Shoulder and Leg Workout Routinebrar352No ratings yet
- Lumbar Spine ExaminationDocument6 pagesLumbar Spine ExaminationSaddam Kanaan100% (1)
- Different Positions Assumed by A Patient During A Physical Examination ProcedureDocument14 pagesDifferent Positions Assumed by A Patient During A Physical Examination ProcedureAziil LiizaNo ratings yet
- Anatomy of The SpineDocument61 pagesAnatomy of The SpineAnonymous 9XDi2Yqa0% (2)
- Shoulder ExaminationDocument4 pagesShoulder ExaminationYS NateNo ratings yet
- Jacobson relaxation techniqueDocument6 pagesJacobson relaxation techniqueJamaicaLabiaga100% (1)
- Examine Cervical Spine Range MotionDocument16 pagesExamine Cervical Spine Range MotionlecturioNo ratings yet
- Physical ExaminationDocument5 pagesPhysical ExaminationAmniAzmi100% (1)
- Head-to-Toe Assessment ChecklistDocument5 pagesHead-to-Toe Assessment ChecklistDianne Dulay VillanuevaNo ratings yet
- Head To Toe Quick Study Guide With NOTESDocument2 pagesHead To Toe Quick Study Guide With NOTESdayana0305No ratings yet
- Neurological Examination of The Limbs TextDocument8 pagesNeurological Examination of The Limbs Textvidur_talrejaNo ratings yet
- Adventist University of The Philippines: Musculoskeletal SystemDocument6 pagesAdventist University of The Philippines: Musculoskeletal SystemAnnie AlbertoNo ratings yet
- Pyshical Examination OrthopaediDocument67 pagesPyshical Examination OrthopaediSheryl ElitaNo ratings yet
- Physical Examination of Spine (TN)Document55 pagesPhysical Examination of Spine (TN)Francesc OktofabregasNo ratings yet
- Excretory System NotesDocument10 pagesExcretory System Noteswama ojha100% (1)
- Pemeriksann Fisis Tulang BelakangDocument78 pagesPemeriksann Fisis Tulang BelakangulfianiNo ratings yet
- Pediatric CVS ExamDocument24 pagesPediatric CVS Examعلي. احمدNo ratings yet
- Final Health Assessment Study GuideDocument11 pagesFinal Health Assessment Study Guideflynnc1No ratings yet
- Session 8and9 Flow of The Exam2008Document3 pagesSession 8and9 Flow of The Exam2008tony_chrisNo ratings yet
- Soap NoteDocument4 pagesSoap NoteMahmoud AlnsourNo ratings yet
- Complete PE Check ListDocument4 pagesComplete PE Check ListgurneeNo ratings yet
- Complete Health AssessmentDocument3 pagesComplete Health AssessmentQueensterNo ratings yet
- Neurological AssessmentDocument76 pagesNeurological Assessmentjcabatit3No ratings yet
- Basic Physical Examination of The Adult: ChecklistDocument3 pagesBasic Physical Examination of The Adult: ChecklistuansettNo ratings yet
- Physical Exam Vital SignsDocument4 pagesPhysical Exam Vital SignsmickeyNo ratings yet
- Physical Exam ChecklistDocument4 pagesPhysical Exam Checklistsharshar09No ratings yet
- ScoliosisDocument8 pagesScoliosisPremnath BalakrishnanNo ratings yet
- Head To Toe Review of SystemsDocument1 pageHead To Toe Review of SystemsSNo ratings yet
- Special Tests: Hand Hygiene &Document2 pagesSpecial Tests: Hand Hygiene &Rida ArifNo ratings yet
- Musculo Neuro Genitalia RectumDocument25 pagesMusculo Neuro Genitalia RectumBiBOYz 143No ratings yet
- Spine 2020Document1 pageSpine 2020fihimeh581No ratings yet
- OSCE HP Procedural Checklist 2019 PDFDocument13 pagesOSCE HP Procedural Checklist 2019 PDFrinkal chavdaNo ratings yet
- Male Exam ScriptDocument7 pagesMale Exam ScriptAnonMeMeMeNo ratings yet
- ASSESSING THE NEUROLOGICAL SYSTEM ChecklistDocument4 pagesASSESSING THE NEUROLOGICAL SYSTEM ChecklistCyril Dayne Marie BaldeNo ratings yet
- The Complete Health Assesment: Putting It All Together: Stikes Syedza Saintika PadangDocument19 pagesThe Complete Health Assesment: Putting It All Together: Stikes Syedza Saintika PadangDaffa MilleniaNo ratings yet
- PE Essential Checklist For OSCE Part 1Document3 pagesPE Essential Checklist For OSCE Part 1Palwasha MalikNo ratings yet
- Subjective Examination and Objective Examination in A Rehab Setting - PhysiotherapyDocument4 pagesSubjective Examination and Objective Examination in A Rehab Setting - PhysiotherapyZ ANo ratings yet
- PT Measurement Practical-2Document28 pagesPT Measurement Practical-2Anthony PatrickNo ratings yet
- Ortho Neuro ExamsDocument0 pagesOrtho Neuro ExamsMaybs Palec Pamplona-ParreñoNo ratings yet
- Spine Exam 2Document44 pagesSpine Exam 2Azmi FarhadiNo ratings yet
- Teknik Anamnesis & Pemeriksaan Fisik Umum (Dr. Rini Bachtiar, SP - PD)Document79 pagesTeknik Anamnesis & Pemeriksaan Fisik Umum (Dr. Rini Bachtiar, SP - PD)nurfatrianiNo ratings yet
- C11 TestingDocument4 pagesC11 TestingHanakoNo ratings yet
- WK 6 Study QsDocument7 pagesWK 6 Study Qsapi-479720222No ratings yet
- Head To Toe AssessmentDocument7 pagesHead To Toe AssessmentShine TorricerNo ratings yet
- OSCE Shoulder Examination: Sunday, May 08, 2011 5:12 PMDocument6 pagesOSCE Shoulder Examination: Sunday, May 08, 2011 5:12 PMproflangaNo ratings yet
- Examination of The Peripheral Neurological SystemDocument2 pagesExamination of The Peripheral Neurological Systemkenners100% (12)
- Head-to-Toe Exam ChecklistDocument5 pagesHead-to-Toe Exam ChecklistIftitah SailyNo ratings yet
- Block 1 Practical 1Document14 pagesBlock 1 Practical 1joe doweNo ratings yet
- The Neurological ExaminationDocument47 pagesThe Neurological ExaminationMichael BonillaNo ratings yet
- Head-to-Toe Assessment ChecklistDocument5 pagesHead-to-Toe Assessment ChecklistGlenn DelarosaNo ratings yet
- 11.musculoskeletalDocument37 pages11.musculoskeletalLaith AsimNo ratings yet
- Paediatric Examination.Document30 pagesPaediatric Examination.Athul IgnatiusNo ratings yet
- Anterior-Posterior Chest Exam PhotoguideDocument9 pagesAnterior-Posterior Chest Exam PhotoguideMark GuirguisNo ratings yet
- OS Control Question List.Document83 pagesOS Control Question List.Jericho von NazarethNo ratings yet
- CDC Definition Active Fitness Daily Tasks VigorDocument3 pagesCDC Definition Active Fitness Daily Tasks VigorMikel MidelNo ratings yet
- Physiology of Thyroid GlandDocument8 pagesPhysiology of Thyroid Glandأياد المشهدانيNo ratings yet
- Danelle Garin Espartero Bsed Science 3-E Answer The Following Questions Briefly But Comprehensively. Use Additional ReferencesDocument7 pagesDanelle Garin Espartero Bsed Science 3-E Answer The Following Questions Briefly But Comprehensively. Use Additional ReferencesDanelleNo ratings yet
- The Kidney DissectionDocument4 pagesThe Kidney DissectionBeverly Carballo - MoguelNo ratings yet
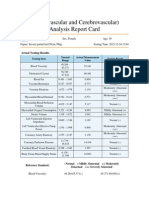
- Cardiovascular and CerebrovascularDocument6 pagesCardiovascular and CerebrovascularJoshelle B. Bancilo0% (1)
- 12th Nursing General EM Book 2020Document336 pages12th Nursing General EM Book 2020Pooja narayananNo ratings yet
- Pages 183 Physiological Psychology MCQ 1Document34 pagesPages 183 Physiological Psychology MCQ 1AdsNo ratings yet
- Adrenal GlandDocument15 pagesAdrenal GlandUnggul YudhaNo ratings yet
- Repertory Big Size James Tyler Kent.05357 - 1Document5 pagesRepertory Big Size James Tyler Kent.05357 - 1chabhadiyaparth008No ratings yet
- 01 Animal TissueDocument8 pages01 Animal TissueRohit SharmaNo ratings yet
- USAR Standard Arm and Hand Signals For Track Vehicle Driving FKG 17-42-2 PDFDocument16 pagesUSAR Standard Arm and Hand Signals For Track Vehicle Driving FKG 17-42-2 PDFfigctoNo ratings yet
- Cranial Nerves TableDocument1 pageCranial Nerves TablePIOZRNo ratings yet
- Lesson TemplateDocument6 pagesLesson TemplateAnonymous 9p23ZapzNo ratings yet
- Clubfoot Ponseti Management, 3rd Edition-1601890028Document32 pagesClubfoot Ponseti Management, 3rd Edition-1601890028Ankur MittalNo ratings yet
- Chapter 24. Sense Organs: ObjectivesDocument25 pagesChapter 24. Sense Organs: ObjectivesFrancisco GonzálezNo ratings yet
- Article 4 - Myobrace PDFDocument8 pagesArticle 4 - Myobrace PDFNaeem MoollaNo ratings yet
- Muscles of MasticationDocument12 pagesMuscles of MasticationGokul VenugopalNo ratings yet
- MakhaarijDocument18 pagesMakhaarijSalia SoumareNo ratings yet
- Heart Dissection Lab Report Guide2Document7 pagesHeart Dissection Lab Report Guide2Dylan FernandezNo ratings yet
- Alternativas A TotalesDocument12 pagesAlternativas A TotalesJuan Jose Stuven RodriguezNo ratings yet
- Final Lesson PlanDocument8 pagesFinal Lesson PlanResa MagusaraNo ratings yet
- Hierarchy of Organization: Associated SLODocument10 pagesHierarchy of Organization: Associated SLOZainne Sarip BandingNo ratings yet
- The Urinary System: Functions, Anatomy, Urine Formation and MicturitionDocument22 pagesThe Urinary System: Functions, Anatomy, Urine Formation and MicturitionHATLERNo ratings yet
- False Localising SignsDocument46 pagesFalse Localising SignsVarun B RenukappaNo ratings yet
- Activity 1Document3 pagesActivity 1Clarin Perez OrdinarioNo ratings yet