You might also like
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Plazomicin: A New Aminoglycoside in The Fight Against Antimicrobial ResistanceDocument15 pagesPlazomicin: A New Aminoglycoside in The Fight Against Antimicrobial ResistancePHARMBITNo ratings yet
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5806)
- Semisynthetic AminoglycosidesDocument18 pagesSemisynthetic AminoglycosidesPHARMBITNo ratings yet
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Maintenance of Classroom 19012023Document2 pagesMaintenance of Classroom 19012023PHARMBITNo ratings yet
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Library ProgramDocument1 pageLibrary ProgramPHARMBITNo ratings yet
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (589)
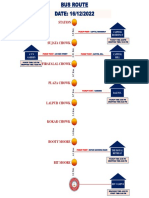
- Route MapDocument3 pagesRoute MapPHARMBITNo ratings yet
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Histoplasma CapsulatumDocument15 pagesHistoplasma CapsulatumLois DanielleNo ratings yet
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (897)
- Dr. S.K. Haldar's Lectures On Industrial Health For AFIH Students - Occu. Lung Dis Asbestosis Silicosis ByssinosisDocument26 pagesDr. S.K. Haldar's Lectures On Industrial Health For AFIH Students - Occu. Lung Dis Asbestosis Silicosis ByssinosisDr. Prakash Kulkarni100% (2)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (401)
- Prado TrialDocument23 pagesPrado TrialBas FrietmanNo ratings yet
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- Antiphospholipid Syndrome A Review PDFDocument9 pagesAntiphospholipid Syndrome A Review PDFDiah Puspita RiniNo ratings yet
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- PeritonitisDocument8 pagesPeritonitismuhammad ridwanNo ratings yet
- Recovery From Temporomandibular Joint Dysfunction: An Overview of Different Physiotherapy ApproachesDocument6 pagesRecovery From Temporomandibular Joint Dysfunction: An Overview of Different Physiotherapy ApproachesSports JournalNo ratings yet
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (345)
- MCN QuestionsDocument15 pagesMCN QuestionsJanika GalindezNo ratings yet
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- Anh Văn Y4Document25 pagesAnh Văn Y4Nhất DuyNo ratings yet
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (842)
- SleDocument41 pagesSleAulya ArchuletaNo ratings yet
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- Aerosol TherapyDocument86 pagesAerosol TherapyReka AgnesNo ratings yet
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- 73-Article Text-213-1-10-20180820Document5 pages73-Article Text-213-1-10-20180820Putri HaniahNo ratings yet
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Fourth Year B SC Nursing Obstetric and Gynaecological Nursing Obstetric NursingDocument35 pagesFourth Year B SC Nursing Obstetric and Gynaecological Nursing Obstetric Nursingsandeepv080% (1)
- Ampicillin Sodium (Polypen)Document3 pagesAmpicillin Sodium (Polypen)Charlene Serino JavierNo ratings yet
- NCP MaternalDocument3 pagesNCP MaternalArmand CabonitaNo ratings yet
- NEC Societys Probiotics Statement - ShareDocument3 pagesNEC Societys Probiotics Statement - Shareendy tovarNo ratings yet
- Mri BasicsDocument51 pagesMri BasicsChristian Barba YañiquezNo ratings yet
- Pediatric Oncology Calculations & Monitoring Clinical PearlsDocument11 pagesPediatric Oncology Calculations & Monitoring Clinical PearlsTaufik HidayahNo ratings yet
- Medical Device Regulation-USFDADocument38 pagesMedical Device Regulation-USFDAMADDINENI AVANEESHWARNo ratings yet
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1091)
- Explain Why You Chose The Data Set(s) You Did, Who The Target Audience Is and The Purpose For Which They Might Use The DataDocument4 pagesExplain Why You Chose The Data Set(s) You Did, Who The Target Audience Is and The Purpose For Which They Might Use The DatalaronNo ratings yet
- 3 - Karyotyping LabDocument17 pages3 - Karyotyping LabEd HouNo ratings yet
- Thesis 2019Document8 pagesThesis 2019Kim YunaNo ratings yet
- Basic Life SupportDocument3 pagesBasic Life SupportKen ManaloNo ratings yet
- Welcome Letter For FamiliesDocument3 pagesWelcome Letter For FamiliesChild and Family InstituteNo ratings yet
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- NCC MERP Index For Categorizing Medication Errors PDFDocument1 pageNCC MERP Index For Categorizing Medication Errors PDFClaudia NogueiraNo ratings yet
- Radiation Protection Bushong Study GuideDocument6 pagesRadiation Protection Bushong Study GuideAsha6842100% (1)
- Drug Study MMRDocument2 pagesDrug Study MMRErika Marie Calucab100% (2)
- Zoo Dentists - Quiz NATALY YULIET GOMEZ CHAGUA PDFDocument2 pagesZoo Dentists - Quiz NATALY YULIET GOMEZ CHAGUA PDFNATALYYULIETNo ratings yet
- The Top 10 Dysmorphic Syndromes: Keys To Diagnosis/What's HotDocument60 pagesThe Top 10 Dysmorphic Syndromes: Keys To Diagnosis/What's HotTom ChanNo ratings yet
- Hope - 1 Grade 11: Exercise For FitnessDocument12 pagesHope - 1 Grade 11: Exercise For FitnessSonnel CalmaNo ratings yet
- Thesis of Dr. AKM Maruf Raza PDFDocument95 pagesThesis of Dr. AKM Maruf Raza PDFMaruf Raza DarubagiNo ratings yet
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)