You might also like
- Fast Facts: Perioperative Pain: Effective management has numerous benefitsFrom EverandFast Facts: Perioperative Pain: Effective management has numerous benefitsNo ratings yet
- A Simple Guide to Neuralgia and Related Nerve DisordersFrom EverandA Simple Guide to Neuralgia and Related Nerve DisordersRating: 5 out of 5 stars5/5 (5)
- Pain in Parkinson's Disease: Blair Ford, MDDocument6 pagesPain in Parkinson's Disease: Blair Ford, MDMaria RamosNo ratings yet
- WEISSPNEDocument4 pagesWEISSPNELauraNo ratings yet
- NantesDiagnosticCriteria For Pudendal NeuralgiaDocument5 pagesNantesDiagnosticCriteria For Pudendal NeuralgiaTeresa BeckNo ratings yet
- Advances in Neuropathic Pain: Diagnosis, Mechanisms, and Treatment RecommendationsDocument11 pagesAdvances in Neuropathic Pain: Diagnosis, Mechanisms, and Treatment Recommendationsgamesh waran gantaNo ratings yet
- Nerve Nerve Nerve Nerve Entrapment Entrapment Syndromes (Nes) Syndromes (Nes)Document52 pagesNerve Nerve Nerve Nerve Entrapment Entrapment Syndromes (Nes) Syndromes (Nes)teshaleNo ratings yet
- Neurophatic PainDocument4 pagesNeurophatic PainicoanamareNo ratings yet
- SPINAL PAIN Diagnostic TriageDocument29 pagesSPINAL PAIN Diagnostic Triagenurul ulyaniNo ratings yet
- MOD014 Nyeri KankerDocument23 pagesMOD014 Nyeri KankerMien Dwi CahyaniNo ratings yet
- Neuropathic PainDocument13 pagesNeuropathic Paintita_leo2No ratings yet
- Brixfinnerup 2013Document12 pagesBrixfinnerup 2013Amany AlnajjarNo ratings yet
- Managing Difficult Cancer Pain: A Stepwise ApproachDocument9 pagesManaging Difficult Cancer Pain: A Stepwise ApproachRina WahyuniNo ratings yet
- Managing Neuropathic PainDocument10 pagesManaging Neuropathic PainAgusBhakti100% (1)
- Chest Pain: Brett E. Fenster, - Teofilo L. Lee-Chiong, JR., - G.F. Gebhart, - Richard A. MatthayDocument15 pagesChest Pain: Brett E. Fenster, - Teofilo L. Lee-Chiong, JR., - G.F. Gebhart, - Richard A. MatthayAsdffdsaNo ratings yet
- Dor NeuropaticaDocument4 pagesDor NeuropaticaRoderley ReisNo ratings yet
- Scanned CamScanner Mixed Pain Concept Chronic Low Back PainDocument18 pagesScanned CamScanner Mixed Pain Concept Chronic Low Back PainMiliza MayangNo ratings yet
- Mari Zita Spa OnDocument57 pagesMari Zita Spa OnMarty BrownNo ratings yet
- Pain Control in Operative DentistryDocument174 pagesPain Control in Operative DentistryNADEEM SHAIKNo ratings yet
- Pain Management Guide for PharmD StudentsDocument30 pagesPain Management Guide for PharmD Studentsstephanie gayetaNo ratings yet
- 2.5 NotesDocument7 pages2.5 NotesKenneth MelchorNo ratings yet
- Paediatrics Pain ManagementDocument9 pagesPaediatrics Pain Managementfuka priesleyNo ratings yet
- QPostHerpeticNeauralgia NSingh PDFDocument3 pagesQPostHerpeticNeauralgia NSingh PDFRincy RincyNo ratings yet
- MacFarlane - Chronic Pain in DogsDocument9 pagesMacFarlane - Chronic Pain in DogsSara ConnorNo ratings yet
- 2014 Chronic Pain. The Role of Learning and Brain PlasticityDocument12 pages2014 Chronic Pain. The Role of Learning and Brain PlasticityCristian OyarzoNo ratings yet
- Issue 43 Spring 2009 PDFDocument16 pagesIssue 43 Spring 2009 PDFSumitha RenganathanNo ratings yet
- Abdominal Visceral Pain: Clinical AspectDocument4 pagesAbdominal Visceral Pain: Clinical AspectMagdy GabrNo ratings yet
- Diabetic Peripheral Neuropathic Pain (DPNP)Document11 pagesDiabetic Peripheral Neuropathic Pain (DPNP)gjgibson2784No ratings yet
- AAHAAAFP Pain Management GuidelinesDocument15 pagesAAHAAAFP Pain Management GuidelinesMr. questionNo ratings yet
- O R o F A C I A L P A I NDocument15 pagesO R o F A C I A L P A I Nsherani999No ratings yet
- Koes2006 PDFDocument5 pagesKoes2006 PDFDewi FathmahNo ratings yet
- Managing Low Back Pain in Primary Care: Chris G Maher, Director Chris Lin, Research FellowDocument5 pagesManaging Low Back Pain in Primary Care: Chris G Maher, Director Chris Lin, Research FellowPaulina ChangoNo ratings yet
- Neurostimulation For Neuropathic Pain: Outcomes and New ParadigmsDocument8 pagesNeurostimulation For Neuropathic Pain: Outcomes and New Paradigmssenad becarevicNo ratings yet
- Postoperative Pain Management Techniques and ModalitiesDocument48 pagesPostoperative Pain Management Techniques and ModalitiesRun HajNo ratings yet
- Topical Meds for Neuropathic Orofacial PainDocument13 pagesTopical Meds for Neuropathic Orofacial PainMarco Antonio Morales OsorioNo ratings yet
- Approach To The Patient With PainDocument22 pagesApproach To The Patient With PainPrincewill SeiyefaNo ratings yet
- PottDocument2 pagesPottkimNo ratings yet
- Clinical Review - FullDocument5 pagesClinical Review - FullBenvenuto AxelNo ratings yet
- Pathophysiology of Non Specific Arm PainDocument10 pagesPathophysiology of Non Specific Arm PainMárcio DominguesNo ratings yet
- 69 20070406145732 AbsDocument5 pages69 20070406145732 AbsEvaldo MamedesNo ratings yet
- A Review On Oral and Dental PainDocument5 pagesA Review On Oral and Dental PainzainaNo ratings yet
- Analgesics: Opioid Analgesics and Antagonist by DR - Humaira AnserDocument91 pagesAnalgesics: Opioid Analgesics and Antagonist by DR - Humaira Anserraffia mahakNo ratings yet
- Greene, S. A. Chronic Pain Pathophysiology and Treatment Implications. Topics in Companion Animal Medicine, v.25, n.1, p.5-9. 2010 PDFDocument5 pagesGreene, S. A. Chronic Pain Pathophysiology and Treatment Implications. Topics in Companion Animal Medicine, v.25, n.1, p.5-9. 2010 PDFFran WermannNo ratings yet
- Benson Pudendal NeuralgiaDocument6 pagesBenson Pudendal NeuralgiaCronoshineNo ratings yet
- Neuropathic Pain: Redefinition and A Grading System For Clinical and Research Purposes - TreedeDocument8 pagesNeuropathic Pain: Redefinition and A Grading System For Clinical and Research Purposes - TreedeNahu SteinmannNo ratings yet
- Peran Akupunktur Medik Pada Kasus NyeriDocument155 pagesPeran Akupunktur Medik Pada Kasus NyeriSilvia HandikaNo ratings yet
- Back PainDocument18 pagesBack PainCabdiladif Ahmed McrfNo ratings yet
- 31 Penodynia-HosthotaADocument2 pages31 Penodynia-HosthotaAMarius CiobotaruNo ratings yet
- Vertigo Vertigo: Pembimbing: Dr. Nella, Sp. SDocument40 pagesVertigo Vertigo: Pembimbing: Dr. Nella, Sp. SAbdil AbdelNo ratings yet
- Centrally Mediated Abdominal Pain SyndromesDocument4 pagesCentrally Mediated Abdominal Pain SyndromesPolo Good BoyNo ratings yet
- PainDocument3 pagesPainMabesNo ratings yet
- Herniated Lumbar Intervertebral Disk: Epidemiology and Natural HistoryDocument6 pagesHerniated Lumbar Intervertebral Disk: Epidemiology and Natural HistoryGeysel SuarezNo ratings yet
- Manajemen NyeriDocument33 pagesManajemen NyeriEL SHITANo ratings yet
- Pain Management AulDocument23 pagesPain Management AulauliaulfaNo ratings yet
- Acupuncture: An Overview of Scientific EvidenceDocument18 pagesAcupuncture: An Overview of Scientific EvidenceIvonne Flores FernándezNo ratings yet
- Pain MNG in KidneyDocument8 pagesPain MNG in KidneyWaqar GhoryNo ratings yet
- MUCLecture 2023 101956636Document27 pagesMUCLecture 2023 101956636علي الاسديNo ratings yet
- Neuropathic Pain v.2Document12 pagesNeuropathic Pain v.2Aulia FitraniNo ratings yet
- Lower Back PainDocument9 pagesLower Back PainKrishelle Kate PannigNo ratings yet
- Anti Nyeri Saraf The Pharmacological TherapyDocument12 pagesAnti Nyeri Saraf The Pharmacological TherapyTiara Renita LestariNo ratings yet
- Technical Analysis GuideDocument3 pagesTechnical Analysis GuideQwerty QwertyNo ratings yet
- Prod 212867Document4 pagesProd 212867Qwerty QwertyNo ratings yet
- DR Jaudy Interview Living in Sickness EnglishDocument4 pagesDR Jaudy Interview Living in Sickness EnglishQwerty QwertyNo ratings yet
- Day 3Document2 pagesDay 3Qwerty QwertyNo ratings yet
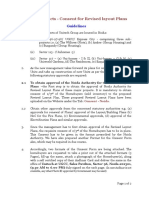
- Consent GuidelinesDocument2 pagesConsent GuidelinesQwerty QwertyNo ratings yet
- Approved Siteplan Noida 117Document1 pageApproved Siteplan Noida 117Qwerty QwertyNo ratings yet
- Get Set Day-2Document1 pageGet Set Day-2Qwerty QwertyNo ratings yet
- What ATF - CVTF To Use For ToyotaDocument7 pagesWhat ATF - CVTF To Use For ToyotaSydneyKasongoNo ratings yet
- Basic Load (Individual) Veterinarian Field PackDocument3 pagesBasic Load (Individual) Veterinarian Field PackJohn MillerNo ratings yet
- Holy Week Labyrinth GuideDocument4 pagesHoly Week Labyrinth GuideEileen Campbell-Reed100% (1)
- SAQ Ans 6Document3 pagesSAQ Ans 6harshanauocNo ratings yet
- 2019 Indonesia Salary GuideDocument32 pages2019 Indonesia Salary Guideiman100% (1)
- Integrated Marketing Communication PlanDocument5 pagesIntegrated Marketing Communication Planprojectwork185No ratings yet
- Overview of Research ProcessDocument31 pagesOverview of Research Processprema balusamyNo ratings yet
- Filipino Nationalism LessonDocument24 pagesFilipino Nationalism LessonIan Jay TumulakNo ratings yet
- MPX English Final Version VOLUME 3Document878 pagesMPX English Final Version VOLUME 3Adrian MacayaNo ratings yet
- Acer Aspire 4535 (Compal LA-4921P) PDFDocument57 pagesAcer Aspire 4535 (Compal LA-4921P) PDFMustafa AkanNo ratings yet
- Madagascar SslevMg v2Document11 pagesMadagascar SslevMg v2Thyan AndrianiainaNo ratings yet
- Unit 5: Structural Modelling: Block II: From Analysis To DesignDocument76 pagesUnit 5: Structural Modelling: Block II: From Analysis To DesignPatrick FarahNo ratings yet
- Remote Control Panel (RCP) User'S GuideDocument13 pagesRemote Control Panel (RCP) User'S GuideAdrian PuscasNo ratings yet
- Islamic Center Design With Islamic ArchiDocument11 pagesIslamic Center Design With Islamic ArchiMuhammad Sufiyan SharafudeenNo ratings yet
- Labconco-3905503 Rev e Purifier Hepa Filtered and Class I Filtered Enclosures User ManualDocument77 pagesLabconco-3905503 Rev e Purifier Hepa Filtered and Class I Filtered Enclosures User ManualCalixto GrajalesNo ratings yet
- HL-1060 User, Parts, and Service Manual 02Document6 pagesHL-1060 User, Parts, and Service Manual 02วรพงษ์ กอชัชวาลNo ratings yet
- Lab Practice # 01 An Introduction To MatlabDocument10 pagesLab Practice # 01 An Introduction To MatlabGhulam Abbas LashariNo ratings yet
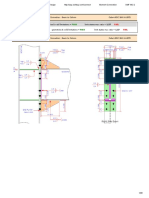
- Result Summary - Overall: Moment Connection - Beam To Column Code AISC 360-16 LRFDDocument29 pagesResult Summary - Overall: Moment Connection - Beam To Column Code AISC 360-16 LRFDYash Suthar100% (2)
- 4684Document2 pages4684Harish Kumar M0% (1)
- St. Augustine School of Nursing: Republic of The Philippines Department of Education SASN - Las PiñasDocument2 pagesSt. Augustine School of Nursing: Republic of The Philippines Department of Education SASN - Las PiñasCarl Joseph MasujerNo ratings yet
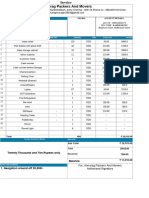
- Titan InvoiceDocument1 pageTitan Invoiceiamdhanush017No ratings yet
- RLT-Guideline Certification: Herstellerverband Raumlufttechnische Geräte E. V. AHU Manufacturer AssociationDocument22 pagesRLT-Guideline Certification: Herstellerverband Raumlufttechnische Geräte E. V. AHU Manufacturer AssociationJorge RoblesNo ratings yet
- Vici Line Card 2015Document14 pagesVici Line Card 2015Argel Linard Francisco MabagaNo ratings yet
- Man 400eDocument324 pagesMan 400eLopez Tonny100% (1)
- S7 - Q2 - Answer KeyDocument11 pagesS7 - Q2 - Answer KeyRaniel LacuarinNo ratings yet
- Families of Carbon Compounds: Functional Groups, Intermolecular Forces, & Infrared (IR) SpectrosDocument79 pagesFamilies of Carbon Compounds: Functional Groups, Intermolecular Forces, & Infrared (IR) SpectrosRuryKharismaMuzaqieNo ratings yet
- Chapter 24 Study QuestionsDocument3 pagesChapter 24 Study QuestionsAline de OliveiraNo ratings yet
- Project management software enables collaborationDocument4 pagesProject management software enables collaborationNoman AliNo ratings yet
- String inverter comparisonDocument4 pagesString inverter comparisonRakesh HateyNo ratings yet
- DP-10/DP-10T/DP-11/DP-15/DP-18 Digital Ultrasonic Diagnostic Imaging SystemDocument213 pagesDP-10/DP-10T/DP-11/DP-15/DP-18 Digital Ultrasonic Diagnostic Imaging SystemDaniel JuarezNo ratings yet