You might also like
- Iep Cheat SheetDocument11 pagesIep Cheat Sheetapi-343665078100% (2)
- Business Proposal LetterDocument12 pagesBusiness Proposal LetterJakeRyanHermosoNo ratings yet
- Benoit Mandelbrot Fractal GeometryDocument19 pagesBenoit Mandelbrot Fractal Geometryindrabudhi100% (1)
- Japan Culture LessonDocument13 pagesJapan Culture Lessonapi-629723918No ratings yet
- Saranya .A: Contact DetailsDocument5 pagesSaranya .A: Contact DetailsCynosure- RahulNo ratings yet
- BLUF Writing FormatDocument9 pagesBLUF Writing FormatSveto Cvetkovski100% (1)
- Secret of Teams Field GuideDocument65 pagesSecret of Teams Field GuideTufail Shaikh100% (2)
- Education JapanDocument15 pagesEducation JapanDylanEga CandradipuraNo ratings yet
- Resume Staff NurseDocument3 pagesResume Staff NurseRetteri KUMARANNo ratings yet
- Vikraman Curriculum WordDocument6 pagesVikraman Curriculum WordVikram SamyNo ratings yet
- Lois Bio DataDocument4 pagesLois Bio DataLois RajuNo ratings yet
- RESUME Yamini1Document2 pagesRESUME Yamini1indisammultiservicesNo ratings yet
- Annex A - Employment Application - UpdatedDocument4 pagesAnnex A - Employment Application - UpdatedAbdurrahman FadlyNo ratings yet
- APPLICATION FORM OHM UpdateDocument5 pagesAPPLICATION FORM OHM UpdateRevi ManrafiNo ratings yet
- Suguna CV PDFDocument7 pagesSuguna CV PDFSreejesh PillaiNo ratings yet
- CMSA Examination Application 69156 2 2 2023Document1 pageCMSA Examination Application 69156 2 2 2023Markhum GoundenNo ratings yet
- Annexure 1: Approval Form. Details To Be Provided by The Student Along With Vaccination ProofsDocument1 pageAnnexure 1: Approval Form. Details To Be Provided by The Student Along With Vaccination ProofsSrikari BNo ratings yet
- Clinical Elective ApplicationDocument2 pagesClinical Elective ApplicationUsama SajidNo ratings yet
- St. Mary's School: General Bhagat Marg, Pune-1Document3 pagesSt. Mary's School: General Bhagat Marg, Pune-1jitendraNo ratings yet
- Curriculum Vitae: 1. Personal Details: Ms. Jayanthi.JDocument6 pagesCurriculum Vitae: 1. Personal Details: Ms. Jayanthi.JRadha ThangamNo ratings yet
- People 360 CVDocument4 pagesPeople 360 CVLey AndeNo ratings yet
- Resume and Cover LetterDocument2 pagesResume and Cover Letterapi-656966222No ratings yet
- CV of Kh. Risal AhamedDocument2 pagesCV of Kh. Risal AhamedMahfuz Hasan TonmoyNo ratings yet
- Singapore FSL New CVDocument2 pagesSingapore FSL New CVAgon AchlysNo ratings yet
- Hadba Mohammad 1063942Document5 pagesHadba Mohammad 1063942fmvxlxdziltmjfurtuNo ratings yet
- Resume Annai CollageDocument2 pagesResume Annai CollageTHAMIZBROWSING CENTERNo ratings yet
- Wa0001.Document4 pagesWa0001.tanmai nooluNo ratings yet
- DHANYADocument3 pagesDHANYADhanya SidhuNo ratings yet
- Employee Application FormDocument5 pagesEmployee Application FormRatih. Angelina97No ratings yet
- Jennilou Arante1Document1 pageJennilou Arante1John Carlo Araza BuedronNo ratings yet
- Mediassist Claim FormDocument5 pagesMediassist Claim FormsureshNo ratings yet
- Declaration - Undertaking Form (Session 2018-19) - ALLEN Career Institute PDFDocument1 pageDeclaration - Undertaking Form (Session 2018-19) - ALLEN Career Institute PDFRishabh KhandelwalNo ratings yet
- Rindy Aryantika Wahyu Nugroho 18036Document6 pagesRindy Aryantika Wahyu Nugroho 18036Widiya BudiNo ratings yet
- Proforma For College - Information Regarding Fee, Bond - Conditions EtcDocument2 pagesProforma For College - Information Regarding Fee, Bond - Conditions EtcSRUTHI K SETHUMADHAVANNo ratings yet
- Application Letter GRIETZYDocument10 pagesApplication Letter GRIETZYgrietzymiralozano75No ratings yet
- Cathy's Scholarship FormDocument5 pagesCathy's Scholarship Formkasara catherineNo ratings yet
- Declaration - 21244292 - 2 - 3 - 2021 11 - 18 - 25 PMDocument1 pageDeclaration - 21244292 - 2 - 3 - 2021 11 - 18 - 25 PMMichael KorsNo ratings yet
- Domiciliary Claim Form (Employee Id: 1025615) Claim No: D0110191025615C001Document1 pageDomiciliary Claim Form (Employee Id: 1025615) Claim No: D0110191025615C001kasi tcsNo ratings yet
- Menteri Sosial Republik IndonesiaDocument1 pageMenteri Sosial Republik IndonesiaYunusNstNo ratings yet
- Dr. Mabin Sultana Keya: Resume ofDocument3 pagesDr. Mabin Sultana Keya: Resume ofRazib ZoyNo ratings yet
- Veena ResumeDocument2 pagesVeena ResumeindisammultiservicesNo ratings yet
- Acknowledgement & Declaration Form (Session 2022-23) 22612229Document1 pageAcknowledgement & Declaration Form (Session 2022-23) 22612229NaraHari ReddyNo ratings yet
- AaaaDocument2 pagesAaaaRohail Khan NiaziNo ratings yet
- JEEVADocument2 pagesJEEVAJeevaNo ratings yet
- Merit Number 43. I Have Been Posted at Taluka Hospital Kotri Thru Letter NoDocument1 pageMerit Number 43. I Have Been Posted at Taluka Hospital Kotri Thru Letter NoZaheer AliNo ratings yet
- FanisaDocument2 pagesFanisaLuluk Indah CahyaniNo ratings yet
- Cvjeevamanik PDFDocument2 pagesCvjeevamanik PDFbharathi yenneNo ratings yet
- Proforma For College - Information Regarding Fee, Bond - Conditions EtcDocument2 pagesProforma For College - Information Regarding Fee, Bond - Conditions EtcThe Indian DentistNo ratings yet
- Cover Letter LihaDocument1 pageCover Letter LihaLiha LihaNo ratings yet
- Guidance and Application ProcessDocument4 pagesGuidance and Application ProcessTONY GO AWAYNo ratings yet
- Penang Adventist Hospital,: Application For Hospital Aid PositionDocument1 pagePenang Adventist Hospital,: Application For Hospital Aid PositionsowndaryasivasangkarNo ratings yet
- CVDocument3 pagesCVSeenha Dewan100% (2)
- Lavanya CVDocument5 pagesLavanya CVlavanruth93No ratings yet
- Phar200 Acceptance Letter PDFDocument2 pagesPhar200 Acceptance Letter PDFNuhu SibaNo ratings yet
- RE: Application For Nursing Staff at Dr. Soekardjo HospitalDocument2 pagesRE: Application For Nursing Staff at Dr. Soekardjo HospitalIndra WijayaNo ratings yet
- Jasmine New Patient 2Document2 pagesJasmine New Patient 2Jasmine MaxwellNo ratings yet
- Updated Matrix Registration Form.Document2 pagesUpdated Matrix Registration Form.Siti ZainunNo ratings yet
- Curriculum Vitae: OF Fatama Akter RipaDocument2 pagesCurriculum Vitae: OF Fatama Akter RipaMayer DoyaNo ratings yet
- Job Application FormDocument9 pagesJob Application FormQhwamë ÊpysødëNo ratings yet
- Curriculum VitaeDocument3 pagesCurriculum VitaeKomalo William chiaNo ratings yet
- Emergency Medical FormDocument1 pageEmergency Medical FormDarren MorrisonNo ratings yet
- Curriculum Vitae: Experience Summary: Ancy T CheriyanDocument3 pagesCurriculum Vitae: Experience Summary: Ancy T CheriyanGloria JaisonNo ratings yet
- CV UpdatesDocument2 pagesCV UpdatesIbrahim Payaz M CPNo ratings yet
- Resume 2014 Terbaru Dan TerkiniDocument7 pagesResume 2014 Terbaru Dan TerkiniNufusYatNo ratings yet
- 8th English Phy EduDocument132 pages8th English Phy EduPoonam DeviNo ratings yet
- Cpar Week 10Document28 pagesCpar Week 10Diane TayobanaNo ratings yet
- Std06 III Maths EM WWW - Governmentexams.co - in PDFDocument65 pagesStd06 III Maths EM WWW - Governmentexams.co - in PDFsubha pratha subhaNo ratings yet
- Least Learned 4TH QTRDocument1 pageLeast Learned 4TH QTRGregory M. CoronadoNo ratings yet
- 111-Article Text-233-1-10-20190124Document12 pages111-Article Text-233-1-10-20190124putriNo ratings yet
- Proposal Defence GuideDocument2 pagesProposal Defence GuideMohd Suhaidi SallehNo ratings yet
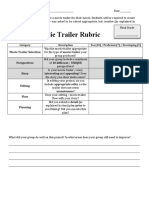
- Capstone Movie Trailer - RubricDocument1 pageCapstone Movie Trailer - RubricMichaelNo ratings yet
- Partisipasi Masy Dalam AMDALDocument106 pagesPartisipasi Masy Dalam AMDALgreenaksesNo ratings yet
- Allie Matarasso ResumeDocument1 pageAllie Matarasso Resumeapi-243273519No ratings yet
- 1-Classroom DynamicsDocument28 pages1-Classroom Dynamicsakhu_79No ratings yet
- University of Mumbai: Syllabus For: S. Y. B. Sc. /S. Y. B. A. Program: B.Sc. /B.A. Course: MathematicsDocument16 pagesUniversity of Mumbai: Syllabus For: S. Y. B. Sc. /S. Y. B. A. Program: B.Sc. /B.A. Course: MathematicsajayNo ratings yet
- Iloilo Federation of Junior Philippine Institute of AccountantsDocument8 pagesIloilo Federation of Junior Philippine Institute of AccountantsLysha DalipeNo ratings yet
- Compiled Pre Board 1Document175 pagesCompiled Pre Board 1tine avanceNo ratings yet
- King Arthur and His KnightsDocument26 pagesKing Arthur and His KnightsSofito DerradjNo ratings yet
- Candidate Profile Form MOL IndiaDocument4 pagesCandidate Profile Form MOL IndiamishratrilokNo ratings yet
- Art Movements Mini Lesson-2Document7 pagesArt Movements Mini Lesson-2api-545455548No ratings yet
- CMI Guidelines For InteroperabilityDocument241 pagesCMI Guidelines For InteroperabilityAnonymous i632Db4vgZNo ratings yet
- Features of Online TeachingDocument12 pagesFeatures of Online Teachingantonytreesa8No ratings yet
- DLP 5 and 6 Pe6Document3 pagesDLP 5 and 6 Pe6Jesson Albaran100% (1)
- INTJ Brief DescriptionDocument2 pagesINTJ Brief DescriptionIllusion ShNo ratings yet
- Learning Competency Monitoring Form (LCMF) : 3 QuarterDocument4 pagesLearning Competency Monitoring Form (LCMF) : 3 QuarterLevie CatalbasNo ratings yet
- PM 101Document17 pagesPM 101Kamran QamarNo ratings yet
- Education Amidst PovertyDocument1 pageEducation Amidst PovertyJessie L. Labiste Jr.No ratings yet