You might also like
- Research Presentations of Dietetic Internship Participants: Research Proceedings - Nutrition and Food SectionFrom EverandResearch Presentations of Dietetic Internship Participants: Research Proceedings - Nutrition and Food SectionNo ratings yet
- Nihms 1503143 Niños y CariesDocument20 pagesNihms 1503143 Niños y CariesLuis franNo ratings yet
- Nihms-1503143-Niños y CariesDocument20 pagesNihms-1503143-Niños y CariesLuis franNo ratings yet
- Sugarpaper 1Document12 pagesSugarpaper 1api-440285766No ratings yet
- Evaluating The Effects of Sugary Beverage Consumption On Child Health in Ghana-JosephineDocument21 pagesEvaluating The Effects of Sugary Beverage Consumption On Child Health in Ghana-JosephineJosephine NarteyNo ratings yet
- Parenthood-A Contributing Factor To Childhood Obesity: ISSN 1660-4601Document11 pagesParenthood-A Contributing Factor To Childhood Obesity: ISSN 1660-4601Syindri AnnisaNo ratings yet
- Early Childhood Caries and Intake of 100 Percent Fruit JuiceDocument8 pagesEarly Childhood Caries and Intake of 100 Percent Fruit JuiceJavier Farias VeraNo ratings yet
- Grupo 3Document9 pagesGrupo 3Michel Vilarinho CarvalhoNo ratings yet
- Oral - Health - and Obesity Policy Brief 2011Document12 pagesOral - Health - and Obesity Policy Brief 2011Anonymous JzT9lVCcNo ratings yet
- ESSINGTON. Legislating Weight Loss. Are Antiobesity Public Health Policies Making An ImpactDocument9 pagesESSINGTON. Legislating Weight Loss. Are Antiobesity Public Health Policies Making An ImpactNina NavajasNo ratings yet
- Exposure To Food Advertising On Television, Food Choices and Childhood ObesityDocument29 pagesExposure To Food Advertising On Television, Food Choices and Childhood ObesityAzam Ali ChhachharNo ratings yet
- EnglishDocument9 pagesEnglishapi-245723352No ratings yet
- The Role of High Sugar Consumption On Diabetes Development Among Adults Living in The United States Research PaperDocument12 pagesThe Role of High Sugar Consumption On Diabetes Development Among Adults Living in The United States Research Paperapi-301801285No ratings yet
- 552.full DisparitiesDocument4 pages552.full DisparitiesFiorellaBeatrizNo ratings yet
- Kids' Sugary Drink Habits Start EarlyDocument4 pagesKids' Sugary Drink Habits Start EarlyAireeseNo ratings yet
- Preventing Childhood Overweight and Obesity: Parents Can Make A DifferenceDocument20 pagesPreventing Childhood Overweight and Obesity: Parents Can Make A DifferenceProject PANo ratings yet
- Peds 2012-1210 FullDocument8 pagesPeds 2012-1210 FullPutu BudiastawaNo ratings yet
- Community Health Project Assignment 01068804Document14 pagesCommunity Health Project Assignment 01068804John HortonNo ratings yet
- Consumption of Sugar-Sweetened Beverages in Mississippi: Is There A Disparity? Behavioral Risk Factor Surveillance System, 2012Document9 pagesConsumption of Sugar-Sweetened Beverages in Mississippi: Is There A Disparity? Behavioral Risk Factor Surveillance System, 2012Fitri RachmadaniNo ratings yet
- JADA 2011 Dye 173 83Document12 pagesJADA 2011 Dye 173 83Risal RisamsahNo ratings yet
- Obese Lotas Brief 2010Document4 pagesObese Lotas Brief 2010bbmantapNo ratings yet
- Policy On Snacks and Sugar-Sweetened BeveragesDocument2 pagesPolicy On Snacks and Sugar-Sweetened BeveragesمعتزباللهNo ratings yet
- Sugar Sweetened Beverages: Factors Affecting Consumption and Level of Awareness On Its Effects To Health Among Nursing Students of Mindanao State University-SuluDocument8 pagesSugar Sweetened Beverages: Factors Affecting Consumption and Level of Awareness On Its Effects To Health Among Nursing Students of Mindanao State University-SuluPsychology and Education: A Multidisciplinary JournalNo ratings yet
- Allentown EpidemiologyDocument14 pagesAllentown Epidemiologyapi-417952873No ratings yet
- HLTH 634 Literature ReviewDocument6 pagesHLTH 634 Literature Reviewapi-362128412No ratings yet
- Drinking Water Linked To Fewer Sugary Drinks. ExerciseDocument3 pagesDrinking Water Linked To Fewer Sugary Drinks. ExerciseRafael FreitasNo ratings yet
- fsn310 - Research PaperDocument8 pagesfsn310 - Research Paperapi-300301211No ratings yet
- Understanding The CauseDocument1 pageUnderstanding The CauseMay Dianne Mansia BautistaNo ratings yet
- Related Literature-StudiesDocument3 pagesRelated Literature-StudiesClarissa MorteNo ratings yet
- Yeayy 6Document11 pagesYeayy 6Amirudin AzhariNo ratings yet
- International Breastfeeding JournalDocument7 pagesInternational Breastfeeding Journalastuti susantiNo ratings yet
- Action On Salt ResponseDocument2 pagesAction On Salt Responsetijak88617No ratings yet
- Influence of Parenting Practices On Eating Behaviors of Early Adolescents During Independent Eating Occasions: Implications For Obesity PreventionDocument19 pagesInfluence of Parenting Practices On Eating Behaviors of Early Adolescents During Independent Eating Occasions: Implications For Obesity PreventionAL-AMEENNo ratings yet
- Content ServerDocument15 pagesContent ServerIrvingHernándezNo ratings yet
- Poor DietDocument9 pagesPoor Dietzegeyebirhanu8No ratings yet
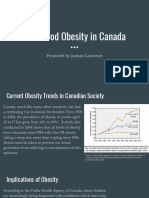
- Childhood Obesity in Canada: Presented by Jaiman LawrenceDocument11 pagesChildhood Obesity in Canada: Presented by Jaiman LawrenceJaiman LawrenceNo ratings yet
- Hs A220 (Us & Alaskan Health Indicators)Document8 pagesHs A220 (Us & Alaskan Health Indicators)teddzquizzerNo ratings yet
- Caregivers' Knowledge of Sugar and Control Over Children's Sugar ConsumptionDocument10 pagesCaregivers' Knowledge of Sugar and Control Over Children's Sugar ConsumptionKatherine VilchezNo ratings yet
- Preventing Obesity and Promoting Cardiometabolic Health: The Promise and Potential of Policies and The Affordable Care ActDocument5 pagesPreventing Obesity and Promoting Cardiometabolic Health: The Promise and Potential of Policies and The Affordable Care ActKristine Anne SorianoNo ratings yet
- Edited Sugary Drinks and Child ObesityDocument4 pagesEdited Sugary Drinks and Child ObesityChristopher Rodriguez PerezNo ratings yet
- Childhood Obesity A Global Public Health Crisis (International Journal of Preventif Medicine)Document7 pagesChildhood Obesity A Global Public Health Crisis (International Journal of Preventif Medicine)faisalNo ratings yet
- A Public Health ConcernDocument2 pagesA Public Health Concernjansen nacarNo ratings yet
- Sugar Drink Consumption Fact SheetDocument3 pagesSugar Drink Consumption Fact SheetMarcosNo ratings yet
- Running Head: PROGRAM DESIGN: Childhood Obesity: Risk Factors & ImplicationsDocument34 pagesRunning Head: PROGRAM DESIGN: Childhood Obesity: Risk Factors & Implicationsapi-338691074No ratings yet
- Example Database IADocument11 pagesExample Database IAnhukhanh1304No ratings yet
- Recomendaciones de DietaDocument3 pagesRecomendaciones de DietaAna CristernaNo ratings yet
- Pi Is 1499404614000827Document7 pagesPi Is 1499404614000827rarazkanthapamenangNo ratings yet
- Research Paper On Childhood Obesity and Fast FoodDocument6 pagesResearch Paper On Childhood Obesity and Fast Foodugmhvdulg100% (1)
- Edna Batong BuhayDocument20 pagesEdna Batong Buhayjingky SallicopNo ratings yet
- Parental Perception of Childhood Obesity in School Age ChildrenDocument10 pagesParental Perception of Childhood Obesity in School Age Childrenapi-282993082No ratings yet
- Childhood Obesity Research Paper ExampleDocument5 pagesChildhood Obesity Research Paper Examplecakvaw0q100% (1)
- HS390 Group6 ResearchDocument6 pagesHS390 Group6 Researchjoseyalm2323No ratings yet
- Obesidad InfantilDocument13 pagesObesidad InfantilBrenda Anali Pariona NapaNo ratings yet
- F Is For Fat: How Obesity Threatens America's FutureDocument124 pagesF Is For Fat: How Obesity Threatens America's FutureDaniel J. SchneiderNo ratings yet
- Selbrede Anna Synthesispaper 5 31Document13 pagesSelbrede Anna Synthesispaper 5 31api-320307298No ratings yet
- Cause and Effect in Childhood ObesityDocument17 pagesCause and Effect in Childhood ObesitySharon V.No ratings yet
- Literature Review FinalDocument11 pagesLiterature Review Finalapi-253949835No ratings yet
- Learning Task Academic ReadingDocument2 pagesLearning Task Academic ReadingYoshe Kartika SentosaNo ratings yet
- Nutrients: Ffee Consumption Among Adults in The UnitedDocument13 pagesNutrients: Ffee Consumption Among Adults in The UnitedPhan Ngọc Thùy TrangNo ratings yet
- Articole MihDocument6 pagesArticole MihNicole StoicaNo ratings yet
- 47 Calderara 2005-02-04Document5 pages47 Calderara 2005-02-04Nicole StoicaNo ratings yet
- 1 Ijerph-18-11411-V2Document11 pages1 Ijerph-18-11411-V2Nicole StoicaNo ratings yet
- 3 Proceeding Ichs 2015-57-63Document7 pages3 Proceeding Ichs 2015-57-63Nicole StoicaNo ratings yet
- 5 TinanoffandPalmerJPHD2000Document10 pages5 TinanoffandPalmerJPHD2000Nicole StoicaNo ratings yet
- 11 Fayle 2003-03-03Document6 pages11 Fayle 2003-03-03Nicole StoicaNo ratings yet
- 6 Alaluusua2010Document6 pages6 Alaluusua2010Nicole StoicaNo ratings yet
- Comentarii ArticoleDocument1 pageComentarii ArticoleNicole StoicaNo ratings yet
- 1 Tagelsirahmed2020Document11 pages1 Tagelsirahmed2020Nicole StoicaNo ratings yet
- Martinez 10.1111@j.1365-263X.2011.01172.xDocument10 pagesMartinez 10.1111@j.1365-263X.2011.01172.xNicole StoicaNo ratings yet
- The Importance of Upper First Permanent Molars Position For The Orthognatic OcclusionDocument7 pagesThe Importance of Upper First Permanent Molars Position For The Orthognatic OcclusionNicole StoicaNo ratings yet
- Aldossary2018 FirstMolarsDocument7 pagesAldossary2018 FirstMolarsNicole StoicaNo ratings yet
- Comprehensive Management of Severe Dental Fluorosis With Adhesively Bonded All-Ceramic RestorationsDocument15 pagesComprehensive Management of Severe Dental Fluorosis With Adhesively Bonded All-Ceramic RestorationsNicole StoicaNo ratings yet
- Preserving Pulp Vitality: Simon Stone, John Whitworth, and Robert WassellDocument6 pagesPreserving Pulp Vitality: Simon Stone, John Whitworth, and Robert WassellNicole StoicaNo ratings yet
- Rde 44 S1Document215 pagesRde 44 S1Nicole StoicaNo ratings yet
- Journal of Dentistry: SciencedirectDocument8 pagesJournal of Dentistry: SciencedirectNicole StoicaNo ratings yet
- More Milk, Stronger Teeth? (Part I)Document4 pagesMore Milk, Stronger Teeth? (Part I)Nicole StoicaNo ratings yet
- 2022 Grade 10 Study GuideDocument85 pages2022 Grade 10 Study Guideeskaykhan11No ratings yet
- 2013 Red Sox Postseason GuideDocument267 pages2013 Red Sox Postseason Guidejen_rogers295100% (1)
- Oracle Apps Isourcing Process FlowDocument4 pagesOracle Apps Isourcing Process FlowRamesh GarikapatiNo ratings yet
- Ipcr Aegp2Document13 pagesIpcr Aegp2Anjo Ellis0% (1)
- Pneumatic Valve With Diaphragm: Instruction, Use and Maintenance ManualDocument50 pagesPneumatic Valve With Diaphragm: Instruction, Use and Maintenance ManualRicardo CalderonNo ratings yet
- Exercises For Functional AnalysisDocument10 pagesExercises For Functional AnalysisEDU CIPANANo ratings yet
- Basics of RainforestsDocument14 pagesBasics of RainforestspsrelianceNo ratings yet
- Nike Marketing Plan PDFDocument1 pageNike Marketing Plan PDFSumaira Binte SaleemNo ratings yet
- ECE Formula SheetDocument7 pagesECE Formula SheetMahendra ReddyNo ratings yet
- First Quarter Examination in PracticalDocument2 pagesFirst Quarter Examination in PracticalMark Anthony B. AquinoNo ratings yet
- Grlweap 2005Document3 pagesGrlweap 2005José RuizNo ratings yet
- Kali Kaula A Manual of Tantric Magick HardbackDocument3 pagesKali Kaula A Manual of Tantric Magick Hardbackalintuta20% (1)
- Clarion CX Basics FundamentalsDocument15 pagesClarion CX Basics FundamentalsRajesh VenkatNo ratings yet
- Aubrey Jaffer: Scheme Implementation Version 5f1Document149 pagesAubrey Jaffer: Scheme Implementation Version 5f1kevinmcguireNo ratings yet
- Backup PolicyDocument2 pagesBackup PolicyEdwin SemiraNo ratings yet
- The Yocum Library Online Database Passwords: All SubjectsDocument3 pagesThe Yocum Library Online Database Passwords: All SubjectsJHSNo ratings yet
- Sample For Solution Manual Theory and Design For Mechanical Measurements 6th Edition by Figliola & BeasleyDocument30 pagesSample For Solution Manual Theory and Design For Mechanical Measurements 6th Edition by Figliola & BeasleyM.R.ZNo ratings yet
- Chapter 1: IntroductionDocument34 pagesChapter 1: IntroductionIntan AifatikaNo ratings yet
- BMC Analytics For BSM 7.6.04 Reference GuideDocument68 pagesBMC Analytics For BSM 7.6.04 Reference GuideCecilio GutierrezNo ratings yet
- Tomato BankDocument67 pagesTomato Bankkmusatheek musatheekNo ratings yet
- The Igloo PartyDocument11 pagesThe Igloo PartyRaghav MalhotraNo ratings yet
- Generators Portable Supersilent DCA60SSI2 Rev 3 STD Manual DataId 19056 Version 1Document164 pagesGenerators Portable Supersilent DCA60SSI2 Rev 3 STD Manual DataId 19056 Version 1andrealunalogoNo ratings yet
- 2023 Global State of Digital Trust Infographic FinalDocument1 page2023 Global State of Digital Trust Infographic Finalhakkan meierNo ratings yet
- Induction Motor NotesDocument20 pagesInduction Motor NotesMani SaiNo ratings yet
- Quantity Calculation FormatDocument8 pagesQuantity Calculation FormatNabraiz AnsariNo ratings yet
- Sebaceous Gland Secretion Is A Major Physiologic Route of Vitamin E Delivery To SkinDocument5 pagesSebaceous Gland Secretion Is A Major Physiologic Route of Vitamin E Delivery To SkinumegeeNo ratings yet
- Final Edit Na Talaga ToDocument82 pagesFinal Edit Na Talaga ToExequel DionisioNo ratings yet
- N5K Troubleshooting GuideDocument160 pagesN5K Troubleshooting GuideLenin KumarNo ratings yet
- Carboxylic Acids and Their DerivativeDocument43 pagesCarboxylic Acids and Their DerivativenathasyaNo ratings yet
- .50 BMG - Wikipedia PDFDocument13 pages.50 BMG - Wikipedia PDFAce ActionNo ratings yet