You might also like
- Radiomics and Its Clinical Application: Artificial Intelligence and Medical Big DataFrom EverandRadiomics and Its Clinical Application: Artificial Intelligence and Medical Big DataNo ratings yet
- Articulo FisioterapiaDocument10 pagesArticulo FisioterapiaMonica LopezNo ratings yet
- Artificial Intelligence Will Soon Change The Landscape of Medical PhysicsDocument3 pagesArtificial Intelligence Will Soon Change The Landscape of Medical Physicsxiwevi4103No ratings yet
- 2019 - Zhou - Caregiver-Delivered Stroke Rehabilitation in Rural ChinaDocument6 pages2019 - Zhou - Caregiver-Delivered Stroke Rehabilitation in Rural ChinaWarsi MaryatiNo ratings yet
- Graham 2006Document18 pagesGraham 2006Sii Odong OdongNo ratings yet
- Teori-Teori Perubahan PerilakuDocument13 pagesTeori-Teori Perubahan PerilakuihsanNo ratings yet
- Stroke Disability and Physiotherapy Interventions: A Quantitative Evaluation of Physiotherapy Treatment Approaches' in ZambiaDocument9 pagesStroke Disability and Physiotherapy Interventions: A Quantitative Evaluation of Physiotherapy Treatment Approaches' in ZambiaPaulomds1991No ratings yet
- A Study to Assess the Effectiveness of Structured Teaching Programme on Knowledge Regarding Body Mechanics in Reducing Low Back Pain Among Staff Nurse at Selected Department of Sharda Hospital of Greater Noida, Uttar PradeshDocument7 pagesA Study to Assess the Effectiveness of Structured Teaching Programme on Knowledge Regarding Body Mechanics in Reducing Low Back Pain Among Staff Nurse at Selected Department of Sharda Hospital of Greater Noida, Uttar PradeshInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- The Impact of Physical Therapy Following Cervical Spine Surgery For Degenerative Spine Disorders: A Systematic ReviewDocument17 pagesThe Impact of Physical Therapy Following Cervical Spine Surgery For Degenerative Spine Disorders: A Systematic ReviewKyle RobinNo ratings yet
- Ethical AnalysisDocument4 pagesEthical Analysisapi-520841770No ratings yet
- SkjaervenoneDocument16 pagesSkjaervenonePrincess Edelweiss CorpuzNo ratings yet
- Interventions Used For Rehabilitation and Prevention of Patellar Tendinopathy in Athletes A Survey of Brazilian Sports Physical TherapistsDocument8 pagesInterventions Used For Rehabilitation and Prevention of Patellar Tendinopathy in Athletes A Survey of Brazilian Sports Physical TherapistsRonny Araya AbarcaNo ratings yet
- Administrative or Educational Medicine: ISPRM - June 12-16, 2011, San Juan, Puerto RicoDocument157 pagesAdministrative or Educational Medicine: ISPRM - June 12-16, 2011, San Juan, Puerto RicoAugusto FuscoNo ratings yet
- PTJ 1383Document14 pagesPTJ 1383marcus souzaNo ratings yet
- Complementary Therapies in MedicineDocument8 pagesComplementary Therapies in Medicinekhadesakshi55No ratings yet
- Attitudes and Barriers Towards Continuing Professional Development Among Physiotherapists in South-Eastern NigeriaDocument9 pagesAttitudes and Barriers Towards Continuing Professional Development Among Physiotherapists in South-Eastern Nigeriaangenicanor7No ratings yet
- The Clinical Implementation of Pain Neuroscience Education: A Survey StudyDocument13 pagesThe Clinical Implementation of Pain Neuroscience Education: A Survey Studycookiepower54321No ratings yet
- Physical Function in Hospice Patients and Physiotherapy Interventions: A Profile of Hospice PhysiotherapyDocument8 pagesPhysical Function in Hospice Patients and Physiotherapy Interventions: A Profile of Hospice PhysiotherapyAnggita Setya LudtianingmaNo ratings yet
- 0849BA768880Document9 pages0849BA768880angenicanor7No ratings yet
- Pzaa 180Document10 pagesPzaa 180Ajeeta KulkarniNo ratings yet
- Moss 2009Document7 pagesMoss 2009Natalia López Aliaga UndaNo ratings yet
- Morley PT Resume 5Document3 pagesMorley PT Resume 5api-422030113No ratings yet
- Critical Appraisal - Research and Evidence: Maisie Sheahan (21215414)Document5 pagesCritical Appraisal - Research and Evidence: Maisie Sheahan (21215414)Jan MackeyNo ratings yet
- An Online Survey of NursingDocument10 pagesAn Online Survey of NursingwilmaNo ratings yet
- Effects of Distraction On Children's Pain and Distress During Medical Procedures A Meta-AnalysisDocument4 pagesEffects of Distraction On Children's Pain and Distress During Medical Procedures A Meta-AnalysisMiguel TuriniNo ratings yet
- Saudi SurveyDocument12 pagesSaudi SurveyNaveen KumarNo ratings yet
- PTJ 20080139Document13 pagesPTJ 20080139Martina SimangunsongNo ratings yet
- Fuentes 2010Document22 pagesFuentes 2010RodrigoAndresVenegasGodoyNo ratings yet
- Bennell. JAMA, 2014Document11 pagesBennell. JAMA, 2014Santiago CerfogliNo ratings yet
- Intensive & Critical Care Nursing: Research ArticleDocument7 pagesIntensive & Critical Care Nursing: Research ArticleEviNo ratings yet
- Knowledge Attitudes and Barriers Towards Evidence Ba - 2017 - Hong Kong PhysioDocument9 pagesKnowledge Attitudes and Barriers Towards Evidence Ba - 2017 - Hong Kong PhysioAnuj ShandilyaNo ratings yet
- Management of Plantar Heel Pain. A Best Practice Guide Informed by A Systematic Review, Expert Clinical Reasoning and Patient ValuesDocument14 pagesManagement of Plantar Heel Pain. A Best Practice Guide Informed by A Systematic Review, Expert Clinical Reasoning and Patient ValuesJesusNavarrete97No ratings yet
- A Systematic Review of Treatments For Mild Traumatic Brain InjuryDocument3 pagesA Systematic Review of Treatments For Mild Traumatic Brain InjurySergio Machado NeurocientistaNo ratings yet
- Listening Is Therapy Patient Interviewing From A Pain Science PerspectiveDocument13 pagesListening Is Therapy Patient Interviewing From A Pain Science PerspectiveDuvan CarvajalNo ratings yet
- Critical Appraisal of EvidenceDocument5 pagesCritical Appraisal of EvidenceLADY JOWAHER ALLASNo ratings yet
- Evaluation of Psychiatric Morbidity in The Community Through Application of Schedule For Clinical Assessment in Neuropsychiatry (Scan)Document6 pagesEvaluation of Psychiatric Morbidity in The Community Through Application of Schedule For Clinical Assessment in Neuropsychiatry (Scan)Dhrubajyoti BhuyanNo ratings yet
- Management of Plantar Heel Pain: A Best Practice Guide Informed by A Systematic Review, Expert Clinical Reasoning and Patient ValuesDocument14 pagesManagement of Plantar Heel Pain: A Best Practice Guide Informed by A Systematic Review, Expert Clinical Reasoning and Patient ValuesMaximiliano LabraNo ratings yet
- FMS Squat Assessment and 2D Video Motion Analysis As Screening inDocument12 pagesFMS Squat Assessment and 2D Video Motion Analysis As Screening inAgus TinaNo ratings yet
- AAEMS Webinar 5 June 2020Document1 pageAAEMS Webinar 5 June 2020John DoeNo ratings yet
- 5-2016 42 Ijmah GoniometeryDocument7 pages5-2016 42 Ijmah GoniometeryNatalie AcostaNo ratings yet
- Manual Therapy: Neil Langridge, Lisa Roberts, Catherine PopeDocument6 pagesManual Therapy: Neil Langridge, Lisa Roberts, Catherine PopeVizaNo ratings yet
- Physical Therapy in Sport: Literature ReviewDocument9 pagesPhysical Therapy in Sport: Literature ReviewPrincess Dianna SulitNo ratings yet
- Documento 4aDocument8 pagesDocumento 4aBelen SozaNo ratings yet
- Joseph Michael Pellerito, JR, MS, OTR Eds Driver RehabilitationDocument671 pagesJoseph Michael Pellerito, JR, MS, OTR Eds Driver Rehabilitationsarawu9911No ratings yet
- Asian Nursing ResearchDocument7 pagesAsian Nursing ResearchWayan Dyego SatyawanNo ratings yet
- Jsaa 086Document11 pagesJsaa 086Elías Coreas SotoNo ratings yet
- OT in The ICU. Revision de Mas de 200 ArticulosDocument8 pagesOT in The ICU. Revision de Mas de 200 ArticulosFlorencia Yael ItovichNo ratings yet
- Journal Homepage: - : IntroductionDocument8 pagesJournal Homepage: - : IntroductionIJAR JOURNALNo ratings yet
- BMC Pediatrics: Effectiveness of Physical Therapy Interventions For Children With Cerebral Palsy: A Systematic ReviewDocument10 pagesBMC Pediatrics: Effectiveness of Physical Therapy Interventions For Children With Cerebral Palsy: A Systematic ReviewERICKNo ratings yet
- Jiwa 1Document10 pagesJiwa 1Sa'adahNo ratings yet
- Caru2020 Article ChildrenSPhysicalActivityBehavDocument12 pagesCaru2020 Article ChildrenSPhysicalActivityBehavkaterinaNo ratings yet
- Fbe - EcuadorDocument7 pagesFbe - EcuadorJoselyn VelasquezNo ratings yet
- Evaluating Preferences For Online Psychological Interventions - 2023 - PsychiatDocument10 pagesEvaluating Preferences For Online Psychological Interventions - 2023 - Psychiattito syahjihadNo ratings yet
- Opioid Analgesics: Symposium On Pain MedicineDocument12 pagesOpioid Analgesics: Symposium On Pain Medicineyunica simanjuntakNo ratings yet
- Manipulation and Mobilization For Treating Chronic Low Back Pain: A Systematic Review and Meta-AnalysisDocument14 pagesManipulation and Mobilization For Treating Chronic Low Back Pain: A Systematic Review and Meta-AnalysisradenbagasNo ratings yet
- K Rivet Amico CV May 20 2018 v2Document27 pagesK Rivet Amico CV May 20 2018 v2api-424535213No ratings yet
- RH Del MS en ACV PDFDocument12 pagesRH Del MS en ACV PDFDiego VolattiNo ratings yet
- Physiological ParametersDocument4 pagesPhysiological ParametersBryan NguyenNo ratings yet
- 9635 34327 1 PBDocument2 pages9635 34327 1 PBTheepan ThuraiNo ratings yet
- Article 7Document9 pagesArticle 7Hamza DibNo ratings yet
- LBP2Document2 pagesLBP2Agus TinaNo ratings yet
- CTS1Document3 pagesCTS1Agus TinaNo ratings yet
- CRS 1Document3 pagesCRS 1Agus TinaNo ratings yet
- Lower Extremity Strengthening - Home Exercise Program: 1. Ankle PumpsDocument3 pagesLower Extremity Strengthening - Home Exercise Program: 1. Ankle PumpsAgus TinaNo ratings yet
- FMS Squat Assessment and 2D Video Motion Analysis As Screening inDocument12 pagesFMS Squat Assessment and 2D Video Motion Analysis As Screening inAgus TinaNo ratings yet
- Reliability and Validity of Standing Balance Measurements With A Motion Analysis SystemDocument8 pagesReliability and Validity of Standing Balance Measurements With A Motion Analysis SystemAgus TinaNo ratings yet
- Rajat Chawla: About MeDocument2 pagesRajat Chawla: About MeRajat ChawlaNo ratings yet
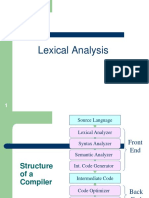
- Lexical AnalysisDocument38 pagesLexical Analysissaeed khanNo ratings yet
- Annual Report 2020 PDFDocument165 pagesAnnual Report 2020 PDFNRNo ratings yet
- Ansible TutorialDocument39 pagesAnsible Tutorialswathi sree100% (1)
- Text Classification To Predict Skin Concerns Over Skincare Using Bidirectional Mechanism in Long Short-Term MemoryDocument11 pagesText Classification To Predict Skin Concerns Over Skincare Using Bidirectional Mechanism in Long Short-Term MemoryCSIT iaesprimeNo ratings yet
- Mercedes Clase S S Guard 2014 INTDocument28 pagesMercedes Clase S S Guard 2014 INTShreyasNo ratings yet
- Threat HuntingDocument2 pagesThreat HuntingDrShubhamangala SunilaNo ratings yet
- Annex B: Application Information For Ampacity CalculationDocument16 pagesAnnex B: Application Information For Ampacity Calculationfa2iiNo ratings yet
- Variance and Standard DeviationDocument17 pagesVariance and Standard DeviationPuja GahatrajNo ratings yet
- Thesis-Speech Recognition MarkovDocument65 pagesThesis-Speech Recognition MarkovTuul TriyasonNo ratings yet
- Ansys Icepak Users GuideDocument1,110 pagesAnsys Icepak Users GuideEsa0% (1)
- BS 4422 2005Document84 pagesBS 4422 2005Dave WilliamsNo ratings yet
- AZ900 Exam Questions Good OneDocument172 pagesAZ900 Exam Questions Good OneShubham Bhaumik100% (1)
- Terastandard - Bsi Bs Iso 5597 267Document26 pagesTerastandard - Bsi Bs Iso 5597 267baladiroyaNo ratings yet
- Algorithm and FlowchartDocument34 pagesAlgorithm and Flowchartmd sufiyanNo ratings yet
- Sentiment Emotion RecognitionDocument6 pagesSentiment Emotion RecognitionSam RockNo ratings yet
- SAP ECC and S4 HANADocument10 pagesSAP ECC and S4 HANASoumya PandaNo ratings yet
- Begin Your Mind Map!: How To Create Mind MapsDocument13 pagesBegin Your Mind Map!: How To Create Mind MapsAnanditaKarNo ratings yet
- Business Certificate Timetable August 2023 Draft Edited 1 1pdf 1686898228811Document3 pagesBusiness Certificate Timetable August 2023 Draft Edited 1 1pdf 1686898228811Sada DahonestNo ratings yet
- Lia Aftanty - 21202241042 - Business PresentationDocument3 pagesLia Aftanty - 21202241042 - Business PresentationLia AftantyNo ratings yet
- DS PPTDocument221 pagesDS PPTanilperfectNo ratings yet
- EGA Pipa ConduitDocument2 pagesEGA Pipa ConduitDerahamaniNo ratings yet
- 11.2.4.4 Packet Tracer - Configuring Port Forwarding On A Linksys Router InstructionsDocument2 pages11.2.4.4 Packet Tracer - Configuring Port Forwarding On A Linksys Router InstructionsLiyanNo ratings yet
- Integrity of Subsea Control UmbilicalDocument11 pagesIntegrity of Subsea Control Umbilicalxinlin.cppNo ratings yet
- A Novel Method For Reconciliation - Julian Et. AlDocument12 pagesA Novel Method For Reconciliation - Julian Et. AlIgnacio UribeNo ratings yet
- PCCCR001Document7 pagesPCCCR001dennisplazaNo ratings yet
- Xerox Phaser 3635mfp - Service ManualDocument202 pagesXerox Phaser 3635mfp - Service ManualFritz BukowskyNo ratings yet
- Lawson Industries, IncDocument4 pagesLawson Industries, IncTony DiStasioNo ratings yet
- 80 High Pressure Piston CompressorDocument10 pages80 High Pressure Piston CompressorSerwis SprężarekNo ratings yet
- Creating Thematic Maps in MapInfo - Geo InformationDocument9 pagesCreating Thematic Maps in MapInfo - Geo InformationMaxim GhereaNo ratings yet