You might also like
- Carsinoma NasopharyngealDocument9 pagesCarsinoma NasopharyngealRahma R SNo ratings yet
- Nasopharyngeal Carcinoma in Children and AdolescentsDocument5 pagesNasopharyngeal Carcinoma in Children and AdolescentsSyifa MunawarahNo ratings yet
- 2021 Consolidation Theraphy in Esophageal CancerDocument6 pages2021 Consolidation Theraphy in Esophageal CancerykommNo ratings yet
- IAEA HPFX 2015Document6 pagesIAEA HPFX 2015Johana PatiñoNo ratings yet
- Dietary Supplement Use in Ambulatory Cancer Patients: A Survey On Prevalence, Motivation and AttitudesDocument9 pagesDietary Supplement Use in Ambulatory Cancer Patients: A Survey On Prevalence, Motivation and AttitudespilarerasoNo ratings yet
- Ja Oude 2019Document23 pagesJa Oude 2019Arlette M.No ratings yet
- Primary Surgery Versus Chemoradiotherapy For Advanced Oropharyngeal Cancers: A Longitudinal Population StudyDocument7 pagesPrimary Surgery Versus Chemoradiotherapy For Advanced Oropharyngeal Cancers: A Longitudinal Population StudyLuvita Amallia SyadhatinNo ratings yet
- Preoperative Clinical Pathway of Breast Cancer Patients: Determinants of Compliance With EUSOMA Quality IndicatorsDocument8 pagesPreoperative Clinical Pathway of Breast Cancer Patients: Determinants of Compliance With EUSOMA Quality Indicatorsyongky sugandaNo ratings yet
- Annals Case Reports PDF Final Final.25.05.l22.Document13 pagesAnnals Case Reports PDF Final Final.25.05.l22.rossbar13No ratings yet
- 10.1245/s10434 018 6369 XDocument9 pages10.1245/s10434 018 6369 Xsayumiholic89No ratings yet
- Triple Negative Breast CancerDocument5 pagesTriple Negative Breast CancerDr SrigopalNo ratings yet
- The OncologistDocument7 pagesThe OncologistManunart FeungpeanNo ratings yet
- Acute Toxicity of Definitive Chemoradiation in Patients With Inoperable or Irresectable Esophageal CarcinomaDocument6 pagesAcute Toxicity of Definitive Chemoradiation in Patients With Inoperable or Irresectable Esophageal Carcinomavirender suhagNo ratings yet
- Pi Is 1879850016300947Document7 pagesPi Is 1879850016300947Daniela GordeaNo ratings yet
- Factors Associated With Short-Term Mortality After Surgical Oncologic EmergenciesDocument12 pagesFactors Associated With Short-Term Mortality After Surgical Oncologic EmergenciesErinda SafitriNo ratings yet
- Brief CommunicationDocument13 pagesBrief CommunicationsantovazNo ratings yet
- Survival Rates For Patients With Resected Gastric Adenocarcinoma Finally Have Increased in The United StatesDocument7 pagesSurvival Rates For Patients With Resected Gastric Adenocarcinoma Finally Have Increased in The United StatesXavier QuinteroNo ratings yet
- Tratat ClorambucilDocument6 pagesTratat ClorambucilDiegoPeixotoNo ratings yet
- Clinical Impact of External Radiotherapy in Non-Metastatic Esophageal Cancer According To Histopathological SubtypeDocument12 pagesClinical Impact of External Radiotherapy in Non-Metastatic Esophageal Cancer According To Histopathological SubtypesilviailieNo ratings yet
- Mertens2021 Article TransthoracicVersusTranshiatalDocument9 pagesMertens2021 Article TransthoracicVersusTranshiatalDr Shiv ChopraNo ratings yet
- Radioterapia en CacUDocument6 pagesRadioterapia en CacUVicente RamosNo ratings yet
- Researcharticle Open AccessDocument10 pagesResearcharticle Open AccessChairul Nurdin AzaliNo ratings yet
- Neoadjuvant Paclitaxel For Operable Breast Cancer: Multicenter Phase II Trial With Clinical OutcomesDocument6 pagesNeoadjuvant Paclitaxel For Operable Breast Cancer: Multicenter Phase II Trial With Clinical OutcomesSubhash SugathanNo ratings yet
- Effect of Gap Length and Position On Results of Treatment of Cancer of The Larynx in Scotland by Radiotherapy.. A Linear Quadratic AnalysisDocument9 pagesEffect of Gap Length and Position On Results of Treatment of Cancer of The Larynx in Scotland by Radiotherapy.. A Linear Quadratic AnalysisrgergerNo ratings yet
- Annotated BibDocument16 pagesAnnotated Bibapi-542958465No ratings yet
- Histopathological Description of Testis Carcinoma and Therapy in Patients at Dr. Hasan Sadikin General Hospital During 2017-2020 REV 31 - 08Document15 pagesHistopathological Description of Testis Carcinoma and Therapy in Patients at Dr. Hasan Sadikin General Hospital During 2017-2020 REV 31 - 08Titus RheinhardoNo ratings yet
- 1677 5538 Ibju 42 04 0694Document10 pages1677 5538 Ibju 42 04 0694Lucas VibiamNo ratings yet
- Abdominoperineal Resection For Squamous Cell Anal Carcinoma: Survival and Risk Factors For RecurrenceDocument8 pagesAbdominoperineal Resection For Squamous Cell Anal Carcinoma: Survival and Risk Factors For RecurrenceWitrisyah PutriNo ratings yet
- De Novo Stage 4 Metastatic Breast Cancer: A Surgical Disease?Document3 pagesDe Novo Stage 4 Metastatic Breast Cancer: A Surgical Disease?jenmercadoNo ratings yet
- Treatment Completion and Costs of A Randomized Trial of Rifampin For 4 Months Versus Isoniazid For 9 MonthsDocument5 pagesTreatment Completion and Costs of A Randomized Trial of Rifampin For 4 Months Versus Isoniazid For 9 MonthsSyairah Banu DjufriNo ratings yet
- Moretto 2014Document8 pagesMoretto 2014Silvie WidyaNo ratings yet
- Efficacy and Safety of Vismodegib in Patients With Advanced Basal Cell Carcinoma (BCC) : 12-Month Update of The ERIVANCE BCC StudyDocument1 pageEfficacy and Safety of Vismodegib in Patients With Advanced Basal Cell Carcinoma (BCC) : 12-Month Update of The ERIVANCE BCC Studyjuloc34No ratings yet
- Pathologic Response When Increased by Longer Interva - 2016 - International JouDocument10 pagesPathologic Response When Increased by Longer Interva - 2016 - International Jouwilliam tandeasNo ratings yet
- Original Research PaperDocument4 pagesOriginal Research PaperDr SrigopalNo ratings yet
- Allen2021 Article ChemotherapyVersusChemotherapyDocument8 pagesAllen2021 Article ChemotherapyVersusChemotherapyXavier QuinteroNo ratings yet
- Rajappa 2019Document6 pagesRajappa 2019abdulrazaqNo ratings yet
- Nimotuzumab With Induction Chemotherapy and Chemo-Radiation in Patients With Advanced Head and Neck CancerDocument8 pagesNimotuzumab With Induction Chemotherapy and Chemo-Radiation in Patients With Advanced Head and Neck Cancerdewi ratnasariNo ratings yet
- (583950958) Journal Leucopenia Treatment Effiicacy NPCDocument8 pages(583950958) Journal Leucopenia Treatment Effiicacy NPCDaniel HoseaNo ratings yet
- Piis0167814019331123 230304 134522Document7 pagesPiis0167814019331123 230304 134522Samuel Kelvin RuslimNo ratings yet
- Male Breast Cancer: An Institutional ExperienceDocument5 pagesMale Breast Cancer: An Institutional ExperienceIJAR JOURNALNo ratings yet
- Aldrink2018 DikonversiDocument31 pagesAldrink2018 DikonversiNadenka BellaNo ratings yet
- annonc_mdw587.026Document1 pageannonc_mdw587.026Aaron Paul BernasNo ratings yet
- 8424365Document8 pages8424365Melody CyyNo ratings yet
- Myositis Abstract v5-TMDocument5 pagesMyositis Abstract v5-TMcaptainessliliNo ratings yet
- Tyroid JournalDocument8 pagesTyroid JournalMukhamad Arif MunandarNo ratings yet
- Erbitux MonotherapyDocument7 pagesErbitux MonotherapyMaulik PatelNo ratings yet
- Impact of Time From Completion of Neoadjuvant Chemotherapy To Surgery On Survival Outcomes in Breast Cancer PatientsDocument7 pagesImpact of Time From Completion of Neoadjuvant Chemotherapy To Surgery On Survival Outcomes in Breast Cancer PatientsPani lookyeeNo ratings yet
- Journal Reading Etika MarcoDocument26 pagesJournal Reading Etika MarcoMarco GunawanNo ratings yet
- Nej Mo A 1414882Document9 pagesNej Mo A 1414882Corina Hagiu-RaduNo ratings yet
- Prediction Model For Shortterm Mortality After Palliative Therapy For Patients Having Advanced Cancer - A Cohort Study From Routine Electronic Medical DataDocument10 pagesPrediction Model For Shortterm Mortality After Palliative Therapy For Patients Having Advanced Cancer - A Cohort Study From Routine Electronic Medical DataHollis LukNo ratings yet
- Society of Surgical Oncology 67th Annual Cancer SymposiumDocument198 pagesSociety of Surgical Oncology 67th Annual Cancer Symposiummc_nsNo ratings yet
- Predicting The Risk of Malignancy in Adnexal Masses Based On IOTA AJOG 2016Document14 pagesPredicting The Risk of Malignancy in Adnexal Masses Based On IOTA AJOG 2016Fernando Suarez ChumaceroNo ratings yet
- Does The Timing of Surgery After Neoadjuvant Therapy in Breast Cancer Patients Affect The Outcome?Document6 pagesDoes The Timing of Surgery After Neoadjuvant Therapy in Breast Cancer Patients Affect The Outcome?Pani lookyeeNo ratings yet
- Treatment Patterns and Outcomes For Patients With Unresectable Stage III and Metastatic Melanoma in The USADocument14 pagesTreatment Patterns and Outcomes For Patients With Unresectable Stage III and Metastatic Melanoma in The USAAditya Gilang Nur PratamaNo ratings yet
- Simanjuntak 2018 J. Phys. Conf. Ser. 1073 042021 PDFDocument8 pagesSimanjuntak 2018 J. Phys. Conf. Ser. 1073 042021 PDFEko RistiyantoNo ratings yet
- Treatment Results For Patients With Squamous-Cell Carcinoma of The Anus, A Single Institution Retrospective AnalysisDocument10 pagesTreatment Results For Patients With Squamous-Cell Carcinoma of The Anus, A Single Institution Retrospective AnalysisJENIFER KARINA PUTZ LORENZINo ratings yet
- Original ArticleDocument6 pagesOriginal ArticleGaluin KulaimNo ratings yet
- Prognostic Factors in Nasopharyngeal Carcinoma With Synchronous Liver Metastasis: A Retrospective Study For The Management of TreatmentDocument7 pagesPrognostic Factors in Nasopharyngeal Carcinoma With Synchronous Liver Metastasis: A Retrospective Study For The Management of TreatmentChairul Nurdin AzaliNo ratings yet
- Clinical StudyDocument7 pagesClinical StudyTit fuckerNo ratings yet
- Welfare Services For Challenged ChildrenDocument42 pagesWelfare Services For Challenged ChildrenRahul Dhaker70% (10)
- Scissor Lift ProcedureDocument2 pagesScissor Lift ProcedureAdhi LatifNo ratings yet
- Pengumuman Jadwal Rapid Test Antigen Gratis Bagi Peserta Ujian SKB CPNS Pemerintah Kota Pangkalpinang 2021Document16 pagesPengumuman Jadwal Rapid Test Antigen Gratis Bagi Peserta Ujian SKB CPNS Pemerintah Kota Pangkalpinang 2021Syahrul SalehNo ratings yet
- PostPartum Family Planning PDFDocument34 pagesPostPartum Family Planning PDFRyan Michael OducadoNo ratings yet
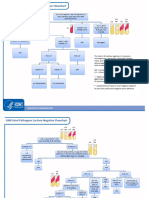
- GNR Stool Pathogens Lactose Negative FlowchartDocument2 pagesGNR Stool Pathogens Lactose Negative FlowchartKeithNo ratings yet
- Aaron Choco de Guzman - BOSH LA 1Document3 pagesAaron Choco de Guzman - BOSH LA 1Aaron Choco De GuzmanNo ratings yet
- Johnson 2020 IOP Conf. Ser. Mater. Sci. Eng. 993 012022Document13 pagesJohnson 2020 IOP Conf. Ser. Mater. Sci. Eng. 993 012022astrid abigail blas sanchezNo ratings yet
- Chrome Lignosulfonate (CLS)Document5 pagesChrome Lignosulfonate (CLS)sajad gohariNo ratings yet
- Research Paper Topics For Developmental PsychologyDocument7 pagesResearch Paper Topics For Developmental PsychologyxbvtmpwgfNo ratings yet
- ANA MAPEH S2017 Ans KeyDocument15 pagesANA MAPEH S2017 Ans KeyVan Errl Nicolai SantosNo ratings yet
- Appointment - CR22 Crane Operator - 2021Document2 pagesAppointment - CR22 Crane Operator - 2021carlthiahNo ratings yet
- Ik Gujral Punjab Technical University Jalandhar, Kapurthala: Sess Sem Sub Code Sub Title Course/BranchDocument178 pagesIk Gujral Punjab Technical University Jalandhar, Kapurthala: Sess Sem Sub Code Sub Title Course/BranchMohit KaundalNo ratings yet
- Experienced Pharmacist Seeking New OpportunityDocument3 pagesExperienced Pharmacist Seeking New OpportunityIman ElshafieNo ratings yet
- Use of Maternal Health Services and Pregnancy Outcomes in NigeriaDocument235 pagesUse of Maternal Health Services and Pregnancy Outcomes in NigeriaAnn Merlin JobinNo ratings yet
- 175 Hys, Matuszek, Olejnik, BierczyńskiDocument9 pages175 Hys, Matuszek, Olejnik, BierczyńskiRadek PolonusNo ratings yet
- Benefits of Eating Dark Chocolate and White Chocolate Bars in Third Year Psychology Students in Cavite State University Silang CampusDocument12 pagesBenefits of Eating Dark Chocolate and White Chocolate Bars in Third Year Psychology Students in Cavite State University Silang CampusPRINCE SARNONo ratings yet
- Act Cart InterventionDocument21 pagesAct Cart Interventionapi-645942287No ratings yet
- Strengthening Mental Health and Psychosocial Support Systems and ServicesDocument116 pagesStrengthening Mental Health and Psychosocial Support Systems and ServicesPan PanNo ratings yet
- CHN Files Complete 1Document316 pagesCHN Files Complete 1ASTR4 BABYNo ratings yet
- Sylvia PlathDocument12 pagesSylvia Plathapi-534201968No ratings yet
- Face Eyes Nose Programme 2019Document13 pagesFace Eyes Nose Programme 2019Renato GoodfellowNo ratings yet
- Do Genes Determine Champions?Document6 pagesDo Genes Determine Champions?mensrea0No ratings yet
- Etched Cast RestorationsDocument41 pagesEtched Cast Restorationssharanya chekkarrajNo ratings yet
- Epidemiological StudiesDocument14 pagesEpidemiological StudiesMuhammad Touseef TahirNo ratings yet
- Learning Activity Sheet: HairdressingDocument5 pagesLearning Activity Sheet: Hairdressingmaricel ubaldoNo ratings yet
- RX Kianbradleyjowett 20240319 080316 0000Document1 pageRX Kianbradleyjowett 20240319 080316 0000cleofeleighclarkNo ratings yet
- 1st Summative Test in in English 6 Q1 Answer KeyDocument4 pages1st Summative Test in in English 6 Q1 Answer KeyGessle GamirNo ratings yet
- Distraction Techniques For Face and Smile Aesthetic Preventing Ageing DecayDocument10 pagesDistraction Techniques For Face and Smile Aesthetic Preventing Ageing DecayAarónNo ratings yet
- Chapter 33 Health AssessmentDocument2 pagesChapter 33 Health AssessmentHanz RapadasNo ratings yet
- List of Allianz Efu Network (Panel) Hospitals: Hospital Name Address Telephone # KarachiDocument6 pagesList of Allianz Efu Network (Panel) Hospitals: Hospital Name Address Telephone # KarachiFaizan BasitNo ratings yet