You might also like
- Colloidal Gold: Principles, Methods, and ApplicationsFrom EverandColloidal Gold: Principles, Methods, and ApplicationsNo ratings yet
- Jurnal Rapid Covid 1Document4 pagesJurnal Rapid Covid 1Dewi Setyaning ValiantoNo ratings yet
- Immunohematology and Transfusion Medicine: A Case Study ApproachFrom EverandImmunohematology and Transfusion Medicine: A Case Study ApproachNo ratings yet
- Test Rapid Igg Igm Ifu EngDocument3 pagesTest Rapid Igg Igm Ifu Engno-replyNo ratings yet
- Step Step: Test ProcedureDocument2 pagesStep Step: Test Procedurespeedy.catNo ratings yet
- Result InterpretationDocument1 pageResult InterpretationARUN KumrNo ratings yet
- COVID-19 IgM/IgG Rapid Test Kit InstructionsDocument4 pagesCOVID-19 IgM/IgG Rapid Test Kit InstructionsMatibar RahmanNo ratings yet
- Mybiosource: Human Novel Coronavirus Nucleoprotein (N) / Spike Glycoprotein (S) Antibody Immunochromatography Assay KitDocument3 pagesMybiosource: Human Novel Coronavirus Nucleoprotein (N) / Spike Glycoprotein (S) Antibody Immunochromatography Assay KitCHMALNo ratings yet
- Result InterpretationDocument1 pageResult InterpretationMohamed SameerNo ratings yet
- COVIDDocument24 pagesCOVIDRida ArifNo ratings yet
- Vidas Sars CovDocument40 pagesVidas Sars Covbudi darmantaNo ratings yet
- Crimean-Congo Haemorrhagic Fever Diagnosis: Hervé ZellerDocument28 pagesCrimean-Congo Haemorrhagic Fever Diagnosis: Hervé ZellerHardik VasnavalaNo ratings yet
- One Step Sars Cov2covid 19iggigm Test 3Document7 pagesOne Step Sars Cov2covid 19iggigm Test 3MariaNo ratings yet
- Result InterpretationDocument1 pageResult InterpretationMarimuthu ThiyagarajanNo ratings yet
- Epilepsy research identifies potential miRNA-based drug targetsDocument39 pagesEpilepsy research identifies potential miRNA-based drug targetshosur mvNo ratings yet
- Clinical Specimens Study Report for STANDARDTM Q COVID-19 TestDocument4 pagesClinical Specimens Study Report for STANDARDTM Q COVID-19 Testniluh suwasantiNo ratings yet
- Report of Mr. Sham Ajay NimjeDocument1 pageReport of Mr. Sham Ajay NimjeRed Light HackersNo ratings yet
- COVID-19 IgG/IgM Rapid Test ResultsDocument4 pagesCOVID-19 IgG/IgM Rapid Test ResultsUruda O Alienígena Quase AlienadoNo ratings yet
- IgM Rapid Gold PDFDocument2 pagesIgM Rapid Gold PDFLeo LgNo ratings yet
- LF G3920SA 0010 Clinical ReportDocument16 pagesLF G3920SA 0010 Clinical ReportRoxana HermosoNo ratings yet
- Molecular Diagnostics COVID-19 Virus Qualitative RT PCRDocument2 pagesMolecular Diagnostics COVID-19 Virus Qualitative RT PCRmanishNo ratings yet
- Enzyme Immunoassays For The Diagnostics of Infection Caused by Sars-Cov-2 Virus (Covid-19)Document12 pagesEnzyme Immunoassays For The Diagnostics of Infection Caused by Sars-Cov-2 Virus (Covid-19)Abdalazeez AlsayedNo ratings yet
- GENEDIA W ONE COVID-19 IgM - IgG BrochureDocument2 pagesGENEDIA W ONE COVID-19 IgM - IgG BrochureBPG ServiceNo ratings yet
- 2019-Ncov Igg / Igm Detection Kit (Colloidal Gold-Based) : Rapid Detection Within 10 Min. No Equipments RequiredDocument4 pages2019-Ncov Igg / Igm Detection Kit (Colloidal Gold-Based) : Rapid Detection Within 10 Min. No Equipments RequiredYelisa SofiaNo ratings yet
- Rapid test detects COVID-19 antibodies in bloodDocument2 pagesRapid test detects COVID-19 antibodies in bloodemmalyneNo ratings yet
- EN COVID19 Infoflyer PDFDocument2 pagesEN COVID19 Infoflyer PDFNaaksh84No ratings yet
- 2-COVID-19 IgM IgG Rapid Test-Instructions For UseDocument2 pages2-COVID-19 IgM IgG Rapid Test-Instructions For UseUruda O Alienígena Quase AlienadoNo ratings yet
- Faqs On Diagnostic Testing For Sars-Cov-2Document7 pagesFaqs On Diagnostic Testing For Sars-Cov-2indraNo ratings yet
- Comparison of Real-Time Reverse Transcriptase Polymerase Chain Reaction (RT-PCR) and Igm-Igg Antibody Test For The Diagnosis of Sars-Cov-2 InfectionDocument18 pagesComparison of Real-Time Reverse Transcriptase Polymerase Chain Reaction (RT-PCR) and Igm-Igg Antibody Test For The Diagnosis of Sars-Cov-2 InfectionRizki AzpiNo ratings yet
- Rapid Test CovidDocument2 pagesRapid Test CovidYuzia Birthdie C UNo ratings yet
- SRBD AntigenDocument4 pagesSRBD Antigenniluh suwasantiNo ratings yet
- Experiment 14Document4 pagesExperiment 14benj panganibanNo ratings yet
- Mycobacterium Tuberculosis With Low-And High-Level ResistanceDocument6 pagesMycobacterium Tuberculosis With Low-And High-Level ResistanceGirish Kishor PaiNo ratings yet
- Prueba Covid Edison PDFDocument3 pagesPrueba Covid Edison PDFEdison Esteban ErasNo ratings yet
- COVID-19 Antibody Test ResultsDocument1 pageCOVID-19 Antibody Test ResultsCakar KlimentNo ratings yet
- Tell Me Fast COVID-19 Antibody TestDocument8 pagesTell Me Fast COVID-19 Antibody TestDortmunderNo ratings yet
- MEGNA HEALTH RAPID COVID-19 IgM/IgG COMBO TEST KITDocument7 pagesMEGNA HEALTH RAPID COVID-19 IgM/IgG COMBO TEST KITMarjorie K. DungalaNo ratings yet
- Covid-19 RT PCR Test Sample Type: Method UsedDocument1 pageCovid-19 RT PCR Test Sample Type: Method UsedAditya UrkudeNo ratings yet
- TeikyoDocument6 pagesTeikyoERIE YUWITA SARINo ratings yet
- ArchitechDocument5 pagesArchitechERIE YUWITA SARINo ratings yet
- Covid-19 Igm/ Igg Rapid Test Kit: InistDocument2 pagesCovid-19 Igm/ Igg Rapid Test Kit: InistDr ThietNo ratings yet
- COVID-19 리플렛 20TDocument2 pagesCOVID-19 리플렛 20TRysla BaliNo ratings yet
- 0310 젠바디 COVID-19 리플렛Document2 pages0310 젠바디 COVID-19 리플렛Fara EsterNo ratings yet
- Patient Report: Results Hiv Blot 2.2 IggDocument1 pagePatient Report: Results Hiv Blot 2.2 IggLufkin BarazarteNo ratings yet
- Covid-19 Igg/Igm Rapid Test Cassette (Whole Blood/Serum/Plasma - Cassette) Product Code: Ccov-200Document2 pagesCovid-19 Igg/Igm Rapid Test Cassette (Whole Blood/Serum/Plasma - Cassette) Product Code: Ccov-200Thiago GalloNo ratings yet
- Report of Mr. Ashish VermaDocument1 pageReport of Mr. Ashish Vermaaman vermaNo ratings yet
- Chembio-DPP-ifu - 0 - Antibody Testing #1Document31 pagesChembio-DPP-ifu - 0 - Antibody Testing #1Heidi RegisterNo ratings yet
- Sheeba SaleemaDocument1 pageSheeba SaleemaSAMIKSHA GHOSHALNo ratings yet
- Inserto RapiGEN COVID 19 IgG IgM DuoDocument2 pagesInserto RapiGEN COVID 19 IgG IgM DuoMacarena VegaNo ratings yet
- EUA Abbott Iggarch IfuDocument12 pagesEUA Abbott Iggarch IfuAbhinavNo ratings yet
- Detection of Sars-Cov-19 Delta Mutant by RT-PCR: A. Sample CollectionDocument4 pagesDetection of Sars-Cov-19 Delta Mutant by RT-PCR: A. Sample CollectionInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Molecular Biology Laboratory ReportDocument1 pageMolecular Biology Laboratory ReportSukumar VadiveluNo ratings yet
- Efficacy of A Test Retest Strategy in Residents AnDocument4 pagesEfficacy of A Test Retest Strategy in Residents AnTari AudinaNo ratings yet
- 8 - Product Performance - Panbio COVID-19Document45 pages8 - Product Performance - Panbio COVID-19Emanuel MontesNo ratings yet
- Paul Andrei Malaborbor - F - 04082022070806Document1 pagePaul Andrei Malaborbor - F - 04082022070806EG MCNo ratings yet
- Ms. SUSHILA FUNDE0 - REPORTDocument1 pageMs. SUSHILA FUNDE0 - REPORTSHITAL KHEDKARNo ratings yet
- PI-M-PIMA-01-EN v13 m-PIMA HIV-12 Detect Cartridge Guide - ENDocument44 pagesPI-M-PIMA-01-EN v13 m-PIMA HIV-12 Detect Cartridge Guide - ENndamnsad23No ratings yet
- Comparison of Commercial RT PCR Diagnostic Kits For COVID 19Document11 pagesComparison of Commercial RT PCR Diagnostic Kits For COVID 19Taufik NurhidayatNo ratings yet
- COVID-19 IVD Raw Material Product Catalogue Aids Diagnostic DevelopmentDocument6 pagesCOVID-19 IVD Raw Material Product Catalogue Aids Diagnostic Developmentsang9eNo ratings yet
- Anteceden Diagnostic Performance of Seven Rapid IgG IgM Antibody Tests and Theeuroimmun IgA IgG ELISA in COVID 19 PatientsDocument6 pagesAnteceden Diagnostic Performance of Seven Rapid IgG IgM Antibody Tests and Theeuroimmun IgA IgG ELISA in COVID 19 PatientsOmar Cucho GamboaNo ratings yet
- Transfusion Ternate 2019. LugyantiDocument28 pagesTransfusion Ternate 2019. LugyantiAi SidiumarNo ratings yet
- Who Recommended Hand-Rub FormulationDocument9 pagesWho Recommended Hand-Rub FormulationSaeed Mohammed100% (2)
- Hospital Monitoring ChartDocument4 pagesHospital Monitoring ChartAi SidiumarNo ratings yet
- Hospital Monitoring ChartDocument4 pagesHospital Monitoring ChartAi SidiumarNo ratings yet
- Bab 10Document29 pagesBab 10Ai SidiumarNo ratings yet
- BAB 2 Triage AnakDocument23 pagesBAB 2 Triage AnakAi SidiumarNo ratings yet
- Tirfor: Lifting and Pulling Machines With Unlimited Wire RopeDocument26 pagesTirfor: Lifting and Pulling Machines With Unlimited Wire RopeGreg ArabazNo ratings yet
- Solutions: Spheres, Cones and CylindersDocument13 pagesSolutions: Spheres, Cones and CylindersKeri-ann MillarNo ratings yet
- Fashion Cycle StepsDocument2 pagesFashion Cycle Stepssaranya narenNo ratings yet
- Lineapelle: Leather & Non-LeatherDocument16 pagesLineapelle: Leather & Non-LeatherShikha BhartiNo ratings yet
- Grade 8 Lily ExamDocument3 pagesGrade 8 Lily ExamApril DingalNo ratings yet
- Casestudy3 Hbo MaDocument2 pagesCasestudy3 Hbo Ma132345usdfghjNo ratings yet
- Winkens Et Al 2009Document8 pagesWinkens Et Al 2009Marta SanchezNo ratings yet
- ElectricalDocument30 pagesElectricalketerNo ratings yet
- Admission Procedure For International StudentsDocument8 pagesAdmission Procedure For International StudentsAndreea Anghel-DissanayakaNo ratings yet
- Ahu, Chiller, Fcu Technical Bid TabulationDocument15 pagesAhu, Chiller, Fcu Technical Bid TabulationJohn Henry AsuncionNo ratings yet
- College of Physical Therapy Produces Skilled ProfessionalsDocument6 pagesCollege of Physical Therapy Produces Skilled ProfessionalsRia Mae Abellar SalvadorNo ratings yet
- Android TabletsDocument2 pagesAndroid TabletsMarcus McElhaneyNo ratings yet
- 20ME901 Automobile Engineering Unit 3Document74 pages20ME901 Automobile Engineering Unit 36044 sriramNo ratings yet
- Timber, PVCu and aluminium window and door hardware systemsDocument24 pagesTimber, PVCu and aluminium window and door hardware systemsOmul Fara NumeNo ratings yet
- Multivariate Analysis Homework QuestionsDocument2 pagesMultivariate Analysis Homework Questions歐怡君No ratings yet
- Google Search StringsDocument12 pagesGoogle Search StringsPrashant Sawnani100% (1)
- Types of NumbersDocument11 pagesTypes of NumbersbrajanosmaniNo ratings yet
- PropensityModels PDFDocument4 pagesPropensityModels PDFSarbarup BanerjeeNo ratings yet
- Muv PDFDocument6 pagesMuv PDFDenisse PxndithxNo ratings yet
- PiXL Knowledge Test ANSWERS - AQA B1 CORE Science - Legacy (2016 and 2017)Document12 pagesPiXL Knowledge Test ANSWERS - AQA B1 CORE Science - Legacy (2016 and 2017)Mrs S BakerNo ratings yet
- Chapter 2 RM - Research ProcessDocument46 pagesChapter 2 RM - Research ProcesseyasuNo ratings yet
- EPISIOTOMYDocument17 pagesEPISIOTOMYKaye Arriane TenorioNo ratings yet
- DLL Grade7 First 1solutions ConcentrationDocument5 pagesDLL Grade7 First 1solutions ConcentrationJaneth de JuanNo ratings yet
- Design & Construction of Substation 16P Painting System ComplianceDocument103 pagesDesign & Construction of Substation 16P Painting System ComplianceRamil LazNo ratings yet
- Document-SAP EWM For Fashion 1.0: 1.general IntroductionDocument3 pagesDocument-SAP EWM For Fashion 1.0: 1.general IntroductionAnonymous u3PhTjWZRNo ratings yet
- Chanel SWOT AnalysisDocument5 pagesChanel SWOT AnalysisJeish KimNo ratings yet
- Decembermagazine 2009Document20 pagesDecembermagazine 2009maria_diyah4312No ratings yet
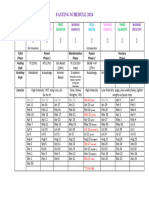
- Moon Fast Schedule 2024Document1 pageMoon Fast Schedule 2024mimiemendoza18No ratings yet
- Virtio-Fs - A Shared File System For Virtual MachinesDocument21 pagesVirtio-Fs - A Shared File System For Virtual MachinesLeseldelaterreNo ratings yet
- 2010-12 600 800 Rush Switchback RMK Service Manual PDFDocument430 pages2010-12 600 800 Rush Switchback RMK Service Manual PDFBrianCook73% (11)